
Abstract
Concha bullosa is a common anatomical variation involving pneumatization of the middle turbinate. Although usually asymptomatic, a large concha bullosa can obstruct nasal airflow and cause related symptoms. Rhinoliths, calcified formations typically found in the inferior meatus, rarely appear within concha bullosa. This report presents a rare case of a rhinolith within a giant concha bullosa in a 15-year-old male experiencing progressive, unilateral nasal obstruction. Computed tomography (CT) revealed a densely-calcified mass inside of an extensive concha bullosa, accompanied by nasal septal deviation and maxillary sinus opacity. The patient underwent successful endoscopic sinus surgery with excision of the concha bullosa’s lateral and medial laminae, facilitating complete rhinolith removal and correction of septal deviation. Postoperative follow-up over 6 months showed complete symptom resolution with no recurrence. This case underscores the importance of CT imaging in evaluating unusual nasal obstructions and highlights endoscopic sinus surgery as an effective approach for extensive concha bullosa. The findings emphasize careful consideration of anatomical variations in clinical practice and contribute to the limited literature on rhinolith formation within concha bullosa. Further studies are warranted to understand the pathogenesis of rhinoliths in nasal anatomical variations.
Introduction
Concha bullosa is a frequently-observed anatomical variation, with prevalence rates reported between 14% and 53%. 1 It is not classified as a disease, but rather as a structural variation characterized by the presence of pneumatization within the turbinate, resulting from an ethmoidal air cell forming inside of it. Generally, concha bullosa is asymptomatic; however, larger conchae may lead to clinical symptoms, including nasal obstruction, headache, and disturbances in olfactory function. 2 Rhinoliths are calcified formations that develop around an endogenous or exogenous core. They most commonly occur in the inferior meatus. 3 The occurrence of a rhinolith within concha bullosa is exceedingly rare, with only a few documented cases in the literature. Here, we report a distinctive case of a rhinolith arising within a giant concha bullosa.
Case Presentation
A 15-year-old male arrived at the otorhinolaryngology clinic with bilateral nasal obstruction, more pronounced on the left side, which had been developing over the past few months. There was no history of rhinorrhea, epistaxis, anosmia, headache, or systemic symptoms. The patient’s medical and surgical history was unremarkable, and he did not report any nasal trauma. Anterior rhinoscopy revealed a large mass with normal mucosa occupying the left nasal cavity and displacing the nasal septum to the right. A computed tomography (CT) scan showed a giant concha bullosa on the left, causing a rightward deviation of the nasal septum and compression of the right middle turbinate, leading to osteomeatal complex obliteration and complete right maxillary sinus opacity. Additionally, a triangular-shaped densely-calcified mass was detected within the concha bullosa (Figure 1). The patient was scheduled for endoscopic sinus surgery under general anesthesia. The procedure involved excising the lateral wall of the concha bullosa and parts of the medial wall extending to the nasal cavity floor. A rhinolith was discovered and removed from the concha bullosa, appearing as a firm calcified mass (Figure 2). Subsequently, septoplasty and right maxillary sinusotomy were performed. The postoperative period was uneventful, and monthly follow-ups for 6 months showed complete symptom resolution and no recurrence evidence.
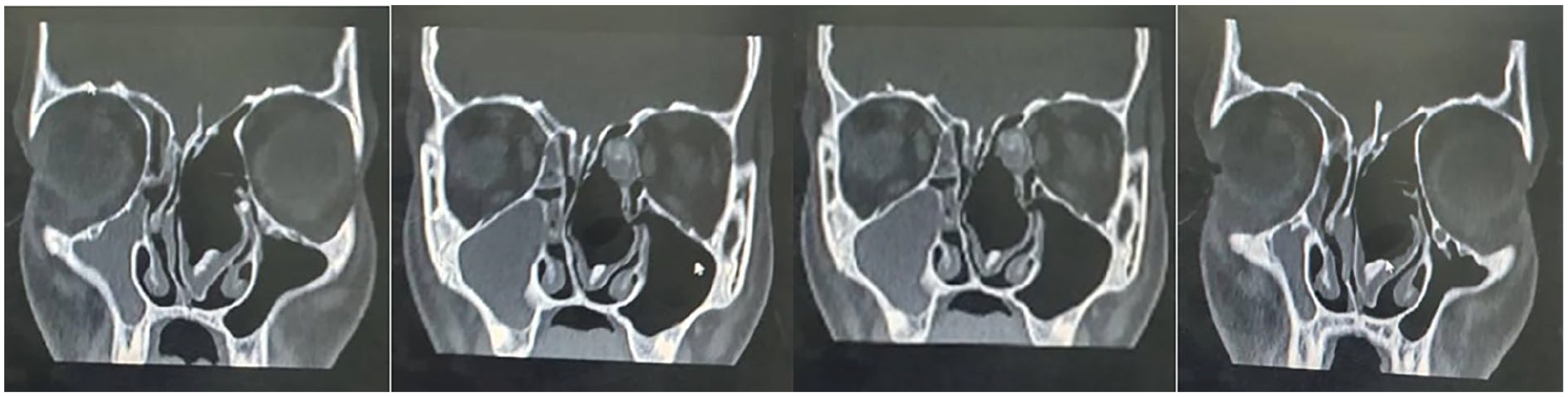
Non-contrast CT scan, coronal view, showing a giant concha bullosa of the left middle turbinate with a deviation of the nasal septum to the right and complete opacity of the right maxillary sinus. With rhinolith within the giant concha bullosa.

Image showing parts of the resected walls of the giant concha bullosa along with the rhinolith (arrow).
Discussion
Concha bullosa is a prevalent case and the most common anatomical variant associated with nasal obstruction and sinusitis, showing in 34% of paranasal CT scans in patients with symptomatic sinus disease.1,4 It involves the pneumatization of the osseous palate of the turbinate, predominantly affecting the middle turbinate, while the inferior turbinate is rarely involved. It can occur unilaterally or bilaterally.2,5 Concha bullosa is categorized into 3 types based on the extent of pneumatization observed on CT scans: lamellar, bulbous, and extensive concha bullosa, with varying incidences. 6 Giant concha bullosa is extremely rare, and all reported cases have been documented individually. The symptoms of concha bullosa are size-dependent, and it is often asymptomatic. When symptomatic, patients may experience nasal obstruction, headache, facial pressure, and anosmia. Nasal endoscopy and CT scans are the best diagnostic tools.1,2 The relationship between concha bullosa and sinusitis is debated, with some studies confirming the connection and others denying it. 7 In our case, right maxillary sinus fullness was likely due to osteomeatal complex obliteration. Studies have also examined the link between concha bullosa and nasal septal deviation, with findings suggesting a significant association between nasal septal convexity away from the concha and the presence of concha bullosa. However, it remains unclear whether the deviation causes the concha bullosa or vice versa. 5 In our patient, the large concha bullosa likely contributed to the deviation. Endoscopic sinus surgery is the preferred treatment for symptomatic concha bullosa. 2 Asymptomatic cases typically do not require surgery. While lamellar and bulbous types usually remain silent, the extensive type often presents a symptomatic clinical picture.2,4 The surgical approaches include lateral and medial laminectomy, total and partial turbinectomy, and crushing, with lateral laminectomy being the most common and total turbinectomy the least common. 2 In our patient, the extensive concha bullosa required the excision of both the lateral and most of the medial lamina. Hanci and Altun compared 3 surgical techniques—lateral laminectomy, medial laminectomy, and crushing—finding that medial laminectomy provided the best improvement in nasal and olfactory functions. 8 Rhinoliths, rare calcifications of endogenous or exogenous origin, are more common in adults than in children and present symptoms such as nasal obstruction, halitosis, nasal discharge, and epistaxis. 3 Various anatomical variations of concha bullosa, including mucosal thickening, polyps within the concha, mucocele, and mucopyocele, have been documented. 9 However, rhinolith within concha bullosa is exceptionally rare. Our case is only the fourth documented instance of rhinolith in concha bullosa, and the first in a giant concha bullosa.3,10,11
The utilization of CT in diagnosing concha bullosa and associated complications is pivotal. The CT scan not only confirmed the presence of a giant concha bullosa but also revealed the deviation of the nasal septum and compression of the right middle turbinate. These findings are crucial for surgical planning and underscore the need for detailed imaging studies in complex cases. Endoscopic sinus surgery remains the cornerstone of treatment for symptomatic concha bullosa. In this case, the excision of both the lateral and most of the medial lamina was necessary due to the extensive size of the concha bullosa. This approach ensured complete removal of the obstructive component and allowed for the extraction of the rhinolith, highlighting the versatility and efficacy of endoscopic techniques in managing such conditions. The presence of a rhinolith within the concha bullosa is an exceptional finding, adding to the complexity of the case. Rhinoliths, although rare, should be considered in the differential diagnosis when dealing with calcified masses within the nasal cavity. This case serves as a reminder of the varied presentations of rhinoliths and their potential association with anatomical variations such as concha bullosa. The uneventful postoperative period and the absence of recurrence over 6 months of follow-up are encouraging. They suggest that endoscopic sinus surgery, when appropriately planned and executed, can yield excellent outcomes in managing giant concha bullosa and associated rhinoliths. Regular follow-up is essential to monitor for any potential recurrence and to ensure sustained symptom resolution. Future studies should aim to elucidate the precise mechanisms leading to the development of rhinoliths within concha bullosa. Additionally, exploring the long-term outcomes of different surgical techniques and their impact on nasal function could provide valuable insights. A larger case series or multicenter studies could help in understanding the prevalence and optimal management strategies for such rare presentations.
Conclusion
This case report highlights the unique presentation and management of a rhinolith within a giant concha bullosa, emphasizing the importance of recognizing anatomical variations in clinical practice. Concha bullosa, while common, typically remains asymptomatic unless it reaches a significant size, as observed in this patient. The presence of a rhinolith within the concha bullosa is exceedingly rare, adding complexity to the clinical scenario. The effective use of CT imaging played a crucial role in diagnosing and planning the surgical approach. Endoscopic sinus surgery proved to be an effective treatment, ensuring the complete removal of the obstructive elements and the rhinolith. Future research should focus on understanding the mechanisms behind rhinolith formation within concha bullosa and the long-term outcomes of various surgical techniques. Larger case series and multicenter studies could provide deeper insights into the prevalence and optimal management of such rare presentations, ultimately improving patient care and outcomes.
Footnotes
Data Availability Statement
The data that support the findings of this study are available from the author or corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethics approval for reporting individual cases. Written informed consent was obtained from the patient’s legal guardian for publication of this case report and accompanying images.