
Abstract
Background
Antral irrigation earlier had an important role in the diagnosis and treatment of rhinosinusitis. Nowadays, it is often considered too unpleasant. However, the experience of patients of this procedure has been very seldom evaluated. Nor has the effect on pain in rhinosinusitis been evaluated. The aim of this study was to evaluate patients’ experience of discomfort and pain during antral irrigation. We also assessed facial pain caused by rhinosinusitis before the procedure and pain soon after the procedure.
Methods
Doctors and 121 patients completed their questionnaires independently after antral irrigation in a university clinic, in a private hospital, and at a communal health center.
Results
Patients experienced mild pain during antral irrigation (mean and median visual analog scale score: <3). Their experience of pain during antral irrigation was closely comparable to pain during dental calculus scaling. Facial pain assessed before antral irrigation decreased quickly after the procedure.
Conclusions
Antral irrigation was well tolerated as an outpatient procedure. The procedure seems to relieve facial pain caused by the disease quickly. The role of antral irrigation in the treatment of acute rhinosinusitis will need further investigation.
Introduction
Acute rhinosinusitis is a common disease, which still has challenges in its diagnostics and treatment. It usually responds well to conservative treatment and about 80% of patients will recover within 2 weeks without antibiotics. 1 However, in some cases, the symptoms can be severe and/or first-line treatment may have been ineffective. In these patients, antral irrigation may be considered. It helps to confirm the diagnosis and to differentiate from other types of facial pain, provides reliable sample for bacterial analysis, and may also relieve facial pain and pressure.
Antral irrigation has for long been the gold standard procedure for the diagnosis of rhinosinusitis in clinical research studies and it was also recommended for treatment of maxillary sinusitis in selected cases.2,3 However, the usefulness of antral irrigation in the treatment of rhinosinusitis has been surprisingly scantily studied and the studies that have been done are old. 4 For the time being, there is no published evidence that antral irrigation would reduce symptoms or recovery time in acute rhinosinusitis and its use has gradually decreased. Recently, optional methods for the collection of microbial samples have been introduced.5,6 In 2011, Desrosiers and his coworkers 7 stated that when culture is required for unusual evolution or complication of acute rhinosinusitis, sampling should be performed either by maxillary tap or endoscopically guided culture. In European position paper on rhinosinusitis and nasal polyposis (EPOS) 2012, antral irrigation was found to be useful for confirming bacteriological diagnosis in intensive care unit patients, 8 but it was not included in diagnostics or treatment of acute maxillary rhinosinusitis in nonhospitalized, nonsedated patients. Apprehensions of painfulness during antral irrigation may also have an effect on its use in diagnostics and treatment.5,9
A recommendation for treatment by antral irrigation in severe or prolonged cases after appropriate medical therapy has failed is still included in Finnish guidelines for rhinosinusitis based on good clinical experience.10,11 Clinical trials are needed to validate or discard this practice. As the first step in evaluation of antral irrigation, we wanted to investigate patients’ experience of this procedure and whether it could be recommended to be suitable for outpatient practice. We also asked the patients to evaluate facial pain before and right after the procedure.
Materials and Methods
The study was conducted during the year 2011 at an outpatient clinic of the Ear, Nose, and Throat (ENT) Hospital of the Helsinki University Hospital (HUH), in an ENT specialist's private practice in Helsinki, and at a communal health center in ähtäri, a small town in Central Finland.
The Finnish Medical Society Duodecim publishes clinical treatment guidelines (www.kaypahoito.f). The guideline for acute rhinosinusitis gives advices for diagnostics and medical treatment. It recommends antral irrigation for severe or prolonged symptoms of acute rhinosinusitis after appropriate medical therapy has failed. The procedure removes secretions from the maxillary sinus, opens the maxillary ostium for a moment, and gives an opportunity to take a bacterial sample. It usually relieves facial pain in acute rhinosinusitis.10,11 The patients in our study were treated according to this guideline. In the year 2011, a sinus X-ray was still commonly taken before sending the patient to HUH for consultation.
Technique of antral irrigation
Local anesthesia is introduced to the inferior meatus with a cotton-tipped applicator soaked in local anesthetic or with a mixture of lidocaine hydrochloride and prilocaine hydrochloride (EMLA cream, Astra-Zeneca) instilled with a suction needle and a syringe. Maxillary sinus puncture is performed with a straight needle (circumference: 1.3-2 mm, length: 12 cm) under the inferior turbinate. The stylet is removed and a 100 mL syringe is connected to the needle with a prefilled silicon tube and a connector. Irrigation is performed with warm (38°C) physiological saline solution with the patient sitting in a forward leaning position.
The patients were informed about the study at the end of their visit. If the patient was willing to participate, he/she completed an informed consent form and filled in a questionnaire before leaving the clinic or at home on the same day. The questionnaires were handed to the nurses or returned by prepaid mail in a closed envelope. The treating physician did not see their answers. The physicians completed their part of the questionnaire at the end of the patients’ visit. The researchers opened and analyzed the data after all the patients had returned the questionnaires.
The patients’ questionnaire included questions about previous experiences of antral irrigation, as well as current symptoms both before and immediately after the procedure. The patients evaluated the severity of facial pain and nasal obstruction on a 10 cm visual analog scale (VAS). VAS values >0 to 3 were graded as mild, >3 to 7 as moderate, and >7 as severe. 12 The same scale was also used in determining the severity of pain caused by antral irrigation. The patients compared the current procedure with their previous experiences. Additionally, they evaluated using VAS their sensation of other common medical procedures, such as having a blood sample taken or dental restoration. The physicians’ questionnaire inquired about their degree and level of experience, way of application, and choice of local anesthetics, as well as the doctors’ impression about the discomfort caused by the irrigation to the patients. We also asked whether the physician experienced any anxiety when performing the procedure.
The study was approved by the Operative Ethics Committee of the Helsinki and Uusimaa Hospital District. This study has been conducted according to the Declaration of Helsinki.
A professional statistician performed the statistical analysis. The Mann-Whitney U-test was used to compare two independent samples and the Kruskall-Wallis analysis of variance was used for comparison of several independent samples. The Wilcoxon signed-rank test was conducted for paired values, eg, when pain was compared before and after antral irrigation. Spearman's rank correlation test was used to assess the connection between the severities of different symptoms. All analyses were conducted with the statistical software NCSS 8 (Number Cruncher Statistical Systems, LLC, Kaysville, UT, USA). P-values <0.05 were considered significant.
Results
Background data
The study population consisted of 121 patients (age range: 18–82 years; mean: 39.2 years; 62% female) undergoing antral irrigation because of symptoms of acute rhinosinusitis. Most patients (100 patients, 82.6%) were from HUH, 11 (9.1%) patients from a private outpatient practice in Helsinki, and 10 (8.2%) from a communal health center in Central Finland. In most cases (n = 69, 58%), antral irrigation was performed by ENT residents from HUH, followed by ENT specialists (n = 26, 22%), medical students under supervision of an ENT specialist (n = 17, 14%), or general practitioners (n = 6, 7%). Fourteen patients had unilateral pain. Bilateral antral irrigation was performed in 95 patients (79%). Pus was found in maxillary sinuses of 83 patients (69%). More than half of the patients (71 patients, 59%) had undergone antral irrigation earlier. The mean duration of symptoms of rhinosinusitis was 31 days (median: 19 days; range: 0–330 days).
Patients’ experience of pain
Patients evaluated their pain on a VAS scale ranging from 0 to 10. The right and left sides were evaluated separately. Antral irrigation was divided into phases: application of the anesthetic, insertion of the needle (maxillary sinus puncture), and the act of rinsing. Patients were asked to evaluate each phase separately on the VAS.
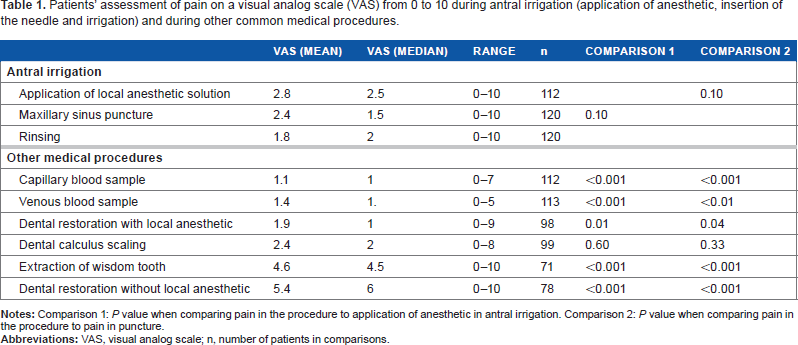
Patients experienced the pain caused by antral irrigation as mild (Table 1, Fig. 1). Application of the local anesthetic (mean: 2.8; median: 2.5; range: 0–10) was the most unpleasant part, followed by insertion of the needle, ie, puncture (mean: 2.4; median: 1.5; range: 0–10). The duration of the patients’ symptoms prior to antral irrigation, the amount or type of effusion obtained from the sinus, or patients’ former experiences of irrigation were not related to the experience of pain during antral irrigation.
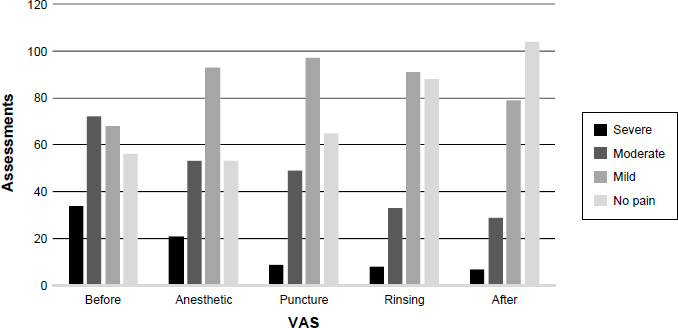
Number of pain assessments on Vas scale before, during, and after antral irrigation. Left and right sides were evaluated separately (severe: Vas > 7-10, black; moderate: Vas > 3-7, dark gray; mild: Vas > 0-3, light gray; no pain: Vas = 0, lightest gray).
Patients’ assessment of pain on a visual analog scale (VAS) from 0 to 10 during antral irrigation (application of anesthetic, insertion of the needle and irrigation) and during other common medical procedures.
Local anesthesia was achieved with EMLAcream in 44 patients (36%), lidocaine–adrenaline solution mixture (lidocaine hydrochloride 40 mg/mL and adrenaline 1:1000) in 54 patients (45%), or cocaine–adrenaline solution in 23 patients (19%). There was no difference in pain assessments between the anesthetic solutions either during application of the anesthetic (P = 0.77) or while inserting the needle in the maxillary sinus (P = 0.9).
Comparison of antral irrigation to other minor medical procedures
Patients were also asked to evaluate the pain caused by other minor medical procedures (Table 1). Having a blood sample taken and dental restoration with anesthetic were found to be less painful than antral irrigation, whereas extraction of wisdom tooth and dental restoration without anesthetic were found more painful than irrigation. Pain during dental calculus scaling did not differ from pain during antral irrigation.
Physicians’ evaluation and professional experience
The physicians’ evaluation of pain in antral irrigation did not differ from the patients’ assessment (application of anesthetics: P = 0.34; maxillary sinus puncture: P = 0.80). They assessed pain to be less severe during insertion of the needle than during application of anesthetic (patients: P = 0.10; physicians: P = 0.001). The doctors’ mean anxiety during the procedure was 1.1.
Patients’ experience of pain and discomfort during antral irrigation was not related to physicians’ professional experience (application of anesthetics: P = 0.70; maxillary sinus puncture: P = 0.56). Physicians’ anxiety also did not correlate with the patients’ experience of pain (application of anesthetics: P = 0.49; maxillary puncture: P = 0.77).
Free comments
In the free text section of the questionnaire, patients’ most common comments on antral irrigation were as follows: not painful/went well/not bad (n = 24), not as bad as expected (n = 17), relieves pressure/pain (n = 11), recommendable (n = 7); or unpleasant (n = 19), unpleasant but not painful (n = 10), exciting/frightening (n = 8), and painful/quite painful (n = 8).
Would I go through it again?
More than half of the patients (72 patients, 59.5%) replied that they would undergo antral irrigation again “by all means” and almost all the rest (43 patients, 35.5%) would agree to a repuncture in case their physicians found it medically indicated. One patient (0.8%) replied that he/she would probably refuse a repuncture. None of the patients chose the alternative “I would definitely refuse a repuncture,” while five patients (4.1%) did not answer the question.
Facial pain before and after antral irrigation
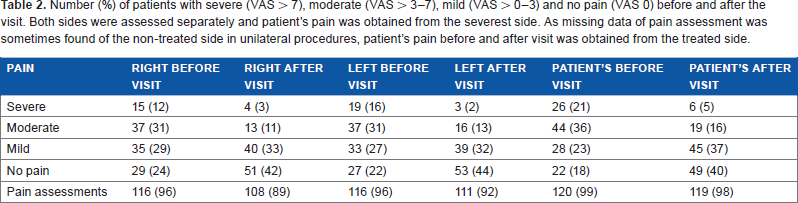
Patients’ facial pain was obtained from the severest side. Twenty-six patients (21%) had severe pain and 44 patients (36%) had moderate pain before antral irrigation. Number of patients with severe or moderate pain decreased to half after antral irrigation (Table 2). Patients’ mean facial pain caused by rhinosinusitis was relieved almost immediately after antral irrigation (Table 3, Fig. 2). Prior to the procedure, the mean assessment of facial pain on a VAS scale was 4.4 (range: 0–10). After some minutes in the waiting room after antral irrigation or the same day at home, the mean VAS was 1.7 (range: 0–10) (P < 0.001). Pus obtained from the maxillary sinus or former experiences of antral irrigation were not related to the decrease of pain.
Number (%) of patients with severe (VAS > 7), moderate (VAS > 3–7), mild (VAS > 0–3) and no pain (VAS 0) before and after the visit. Both sides were assessed separately and patient's pain was obtained from the severest side. As missing data of pain assessment was sometimes found of the non-treated side in unilateral procedures, patient's pain before and after visit was obtained from the treated side.
Change of mean pain in groups by severity of pain (VAS > 7 severe, VAS > 3-7 moderate, VAS > 0-3 mild and VAS = 0 no pain). Both sides were assessed separately and patient's pain before and after visit was obtained from the severest side.
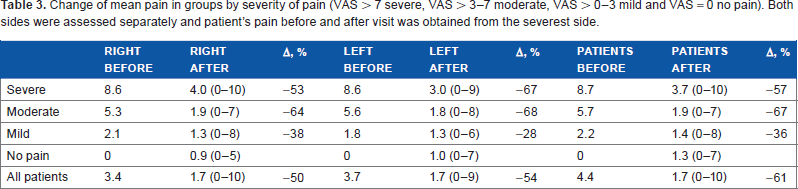
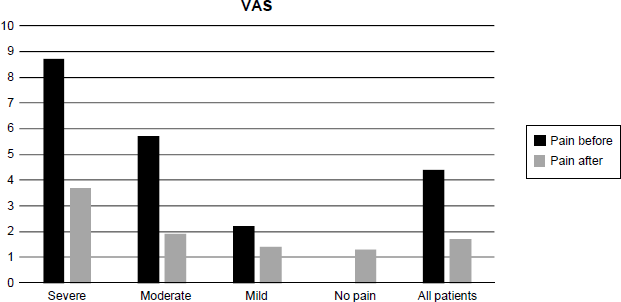
Patients’ evaluation of pain on the VAS scale before and after antral irrigation. Mean facial pain in groups of severity before antral irrigation (black) and after the procedure (gray) is presented (severe: VAS > 7–10; moderate: VAS > 3–7; mild: VAS > 0–3; no pain: VAS = 0). Patients’ pain from the severest side was obtained.
Discussion
Patients assessed pain and discomfort caused by antral irrigation to be mild, and the vast majority would not hesitate to undergo the procedure again. Pain during treatment was not worse than pain caused by the acute rhinosinusitis. When patients evaluated pain in other minor medical procedures, dental calculus scaling was found to be the most closely comparable to antral irrigation. Additionally, we noted a relief in facial pain after the procedure.
Pain and discomfort are always subjective and therefore patients’ point of view should be carefully evaluated. The only study 13 we found on antral irrigation and patient experience was performed in United Kingdom and published in 1987. It stated that 91% of 200 patients were willing to undergo the puncture again. 13 In the present study, this number was 95%. The mean VAS of pain, unpleasantness, and side effects during antral irrigation in the English study was only 21–30 (maximum: 100). This finding is well in accordance with our findings of mild pain, score <3 in mean VAS, during antral irrigation.
When comparing antral irrigation to other minor medical procedures, pain during dental calculus scaling was reported to be closest (Table 1). Informing the patients of minor procedures that are comparable to antral irrigation may help to relieve their anxiety before the procedure. In the present study, neither physicians’ professional experience nor their anxiety had an effect on patients’ experience of pain. Furthermore, physician's evaluation of patient's pain was close to the patient's own assessment, so the patients’ reported experiences during antral irrigation were likely to be well considered.
In the present study, pain was not increased due to the procedure; instead, a quick relief of facial pain after antral irrigation was noticed. Some patients had sought help due to prolonged symptoms of acute rhinosinusitis with only mild pain or no pain, but most of the patients had moderate or severe pain. Decrease of pain right after the procedure is promising, but this finding should be interpreted with caution and studied with a controlled study design with longer follow-up. Questions like whether antral irrigation relieves symptoms in the long run, prevents chronic disease, or decreases treatment costs were not in the scope of this study and need to be determined in a different setting.
Patients’ experiences of pain from previous procedures may be a potential cause of bias due to the time passed. However, when patients evaluated their former antral irrigation and the present one, the latest procedure was experienced to be less unpleasant. This suggests that patients’ assessment of pain in former minor procedures had probably not decreased with time.
Conclusions
Pain during antral irrigation is usually mild and should not hinder this procedure when indicated. Further studies are needed to better elucidate the role of antral irrigation in diagnosis and treatment of acute rhinosinusitis.
Author Contributions
Conceived and designed the experiments: MH, KB, PV. Analyzed the data: KB, PV. Wrote the first draft of the manuscript: KB, PV. Contributed to the writing of the manuscript: PV, KB, LE, MH, SY, ML. Agree with manuscript results and conclusions: PV, KB, LE, MH, SY, ML. Jointly developed the structure and arguments for the paper: KB, LE, MH, PV. Made critical revisions and approved final version: PV, KB, LE, MH, SY, ML. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgments
This work was performed at the ENT Hospital, Helsinki, in Inter-Municipal Health Center of Kuusiokunnat, and in Dextra Medical Center. The results of this study were presented at the 25th Congress of the European Rhinologic Society, held at Amsterdam in June 2014.