
Abstract
Background
Nasal irrigation is among the most widely used treatment modalities for sinonasal diseases. The extent of irrigation is well studied in operated sinuses but not for non-operated sinuses. Moreover, the preferred head positioning during irrigation is not known. Herein, we studied the extent of nasal irrigation in cadaveric heads with non-operated sinuses.
Methods
Nine cadaveric heads were used. Normal saline solution mixed with radiological contrast material was used to irrigate the nasal cavities with the heads in 2 different positions: standing-leaning-forward (SLF) and Head-down forward (HDF). After each irrigation, computed tomography images of the head were acquired. The extent of irrigation was assessed for each subunit of the sinonasal cavity.
Results
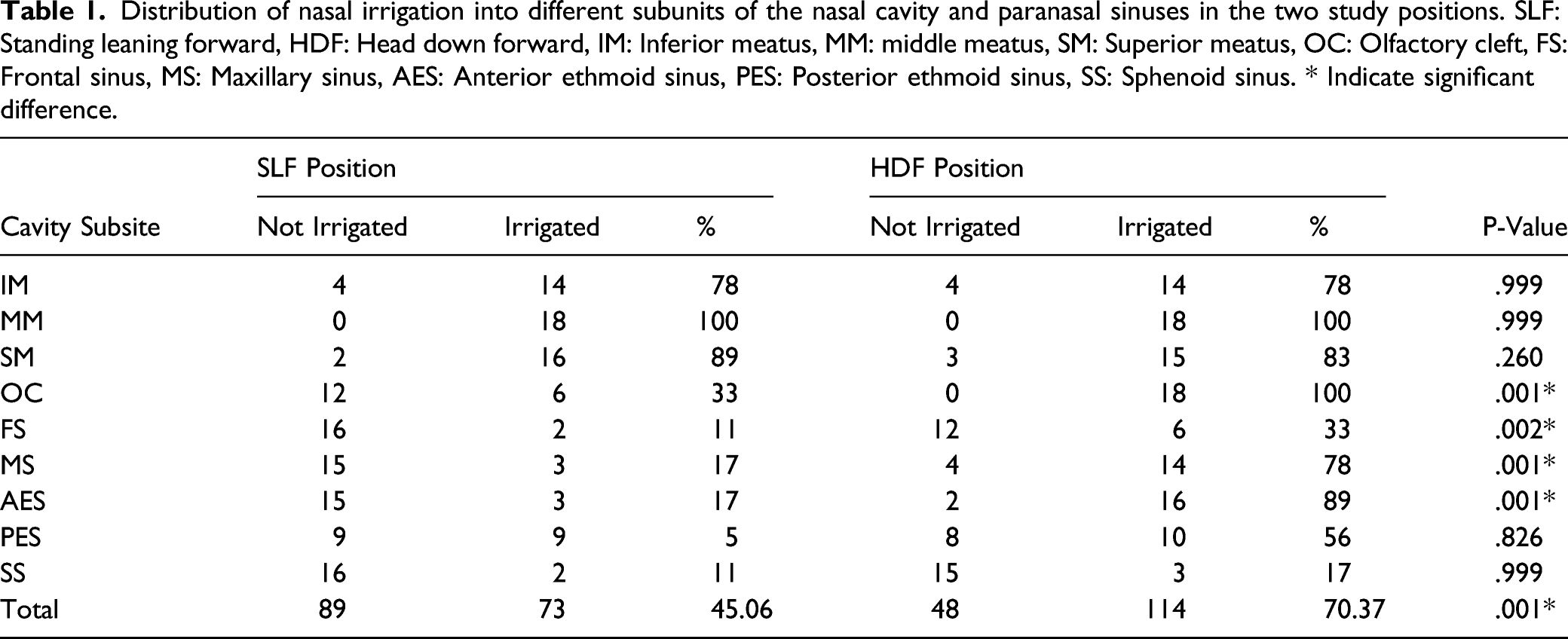
Irrigation was performed twice on a total of 18 sides, each time in 1 position. Nine subunits were evaluated: inferior, middle, and superior meati; the olfactory cleft; and the frontal, maxillary, anterior, and posterior ethmoid and sphenoid sinuses. The extent of irrigation was significantly better in the HDF position for the olfactory cleft (100% vs 33%), P-value=.001, frontal sinus (33% vs 11%), P-value=.002, maxillary sinus (78% vs 17%), P-value=.001, and anterior ethmoid sinus (89% vs 17%), P-value=.001. There was no significant difference in the extent of irrigation between the 2 positions for the other evaluated subunits. The overall extent of irrigation was 70.37% of the subunits in HDF position and 45.06% of the subunits for SLF position, P-value= .001
Conclusions
Nasal irrigation reached the cavities of non-operated paranasal sinuses. However, while the extent of irrigation was limited in the SLF, it was well achieved in the HDF position. Studies on the clinical efficacy of irrigation in this position are recommended.
Introduction
Chronic rhinosinusitis is a common clinical condition currently understood to be related to an abnormal immune system reaction leading to inflammation. Based on this concept, the current treatment is mainly directed at controlling the immune system locally or systemically. Intranasal medications including saline irrigations and local steroid are the most widely accepted initial treatment modality.1 Different forms of local medication dispensers have been studied, including sprays, drops, irrigation, ointments, exhalation delivery systems, and drug-releasing implants.1,2 Several studies evaluated the extent of drops and sprays on non-operated paranasal sinuses. The extent of irrigation has been studied, as well, in the operated cases, where all sinuses are directly and widely opened to the nasal cavities.3-5 The extent of delivery of nasal irrigation to the non-operated paranasal sinus cavities has not been studied well in the literature. Therefore, our study aimed to assess the extent of nasal irrigation in non-operated cadaveric heads in 2 different positions, standing-leaning-forward (SLF) and head-down forward (HDF) position. The SLF is a position where the patient is supposed to stand or sit while his head is leaning forward in a 30-degree angle (see figure 1). The HDF position is a position where the patient is supposed to be on the ground over his forehead, knees, and feet (see figure 2). We anticipate that our study will have a positive impact on the understanding of the modalities of nasal irrigation and proper head positioning during its administration for non-operated patients who need nasal irrigations for sinonasal diseases. This study is timely as there has been more recent interest on the utility of nasal irrigations in non-operated patient (usually with topical steroids) in an effort to avoid surgery during the COVID-19 pandemic. The current study is unique in that it utilizes a radiographically opaque irrigation. The standing leaning forward (SLF) position. A and B, Head positioning. C, Contrast material injection in one nostril and the suction tip at the orifice of the other nostril. The Head Down Forward (HDF) position. A, Head positioning. B, Contrast material injection in one nostril and the suction tip at the orifice of the other nostril.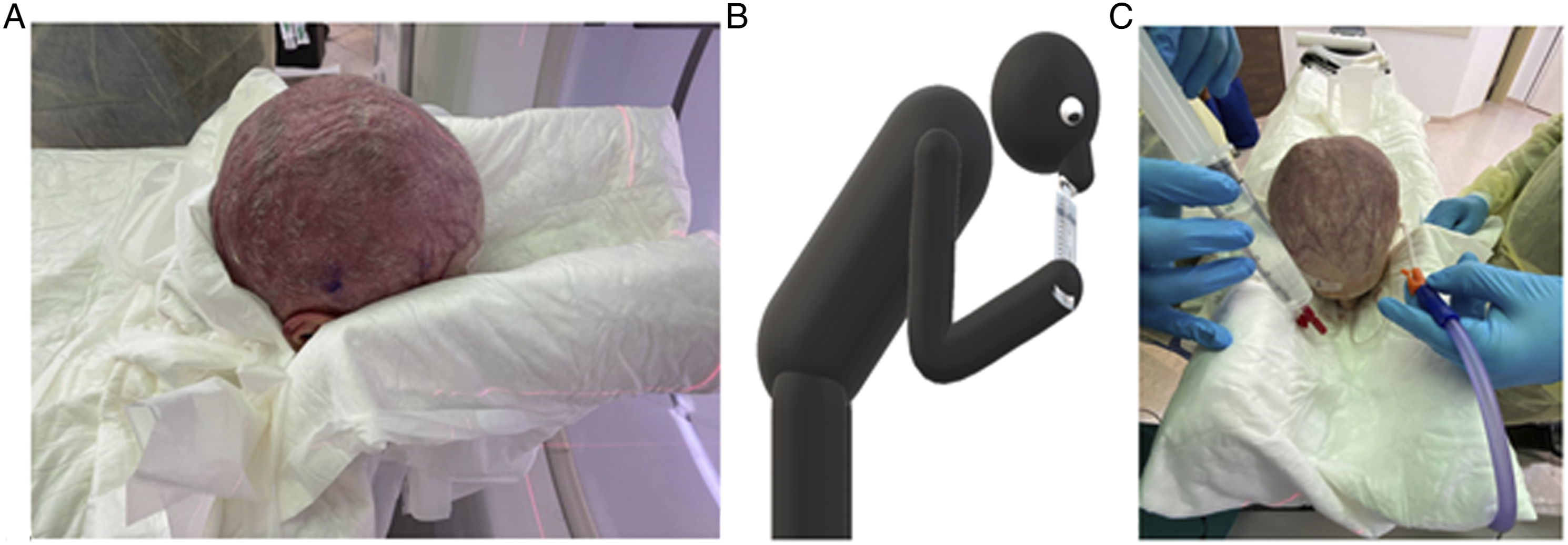

Materials and Methods
This trial was conducted on fresh cadaveric heads in King Saud University, Riyadh, Saudi Arabia. The King Saud University institutional research board approved the study (No. E-20-4619). The trial was performed in accordance with relevant named guidelines and regulations. The cadaveric heads were to be used for skull base dissection course after the trial, and informed consents are obtained from donors. All heads were examined endoscopically and scanned with computed tomography (CT) to confirm that the sinuses have not been violated before by surgery or trauma or are obstructed by any abnormality. For irrigation, we used iodixanol injectable contrast material (Visipaque 320 mg/mL, GE Healthcare Ireland, Cork) mixed with normal saline solution (50 mL Visipaque +200 mL saline). Each head was irrigated with 100 mL, 50 mL each nostril over 5 seconds in 1 position while a suction catheter tip in the other nostril, then vice versa. There was no seal between the nostril and the syringe. Then CT scan was performed while the head remained in the same position within a maximum of 2 minutes (see Figures 1 and 2). After CT scanning, further suctioning done to make sure no residual in the nasal cavities before changing to the other head position. We tried to overcome the washout confirmation by alteration of the sequence of the positions. The first 5 heads were irrigated in the HDF position initially, then changed to the SLF position, and the rest 4 heads were irrigated in an opposite sequence. The extent of irrigation was evaluated for each side of the inferior, middle, and superior meati; olfactory cleft; frontal, maxillary, anterior and posterior ethmoid, and sphenoid sinuses radiologically. Each of these cavities was given the following score: 0, if no contrast was seen; 1, if contrast was seen on 1 side; and 2, if contrast was seen on both sides. The post-irrigation images were independently evaluated by 2 rhinologists (see figure 3). The maximum total score was 18/18 for each subunit. Data were analyzed using the Statistical Package for the Social Sciences (SPSS v. 22; IBM Corp, New York, USA) and the chi-squared test for categorical variables. Paired sample t-test was used for analyzing the mean values. We considered a P-value < .05 to be statistically significant. Computed tomographic images showing the extent of the contrasted saline irrigation. A, In the standing-leaning-forward position, contrast material in the posterior ethmoid air cells and a small amount hugged by the middle turbinates bilaterally can be seen but not in the maxillary or sphenoid sinuses. B and C, In the HDF position, the contrasted irrigation can be seen in both inferior meati, both maxillary sinuses, olfactory clefts, anterior ethmoid air cells, and frontal sinuses. Red arrows indicate the contrast irrigation reaching the subunits.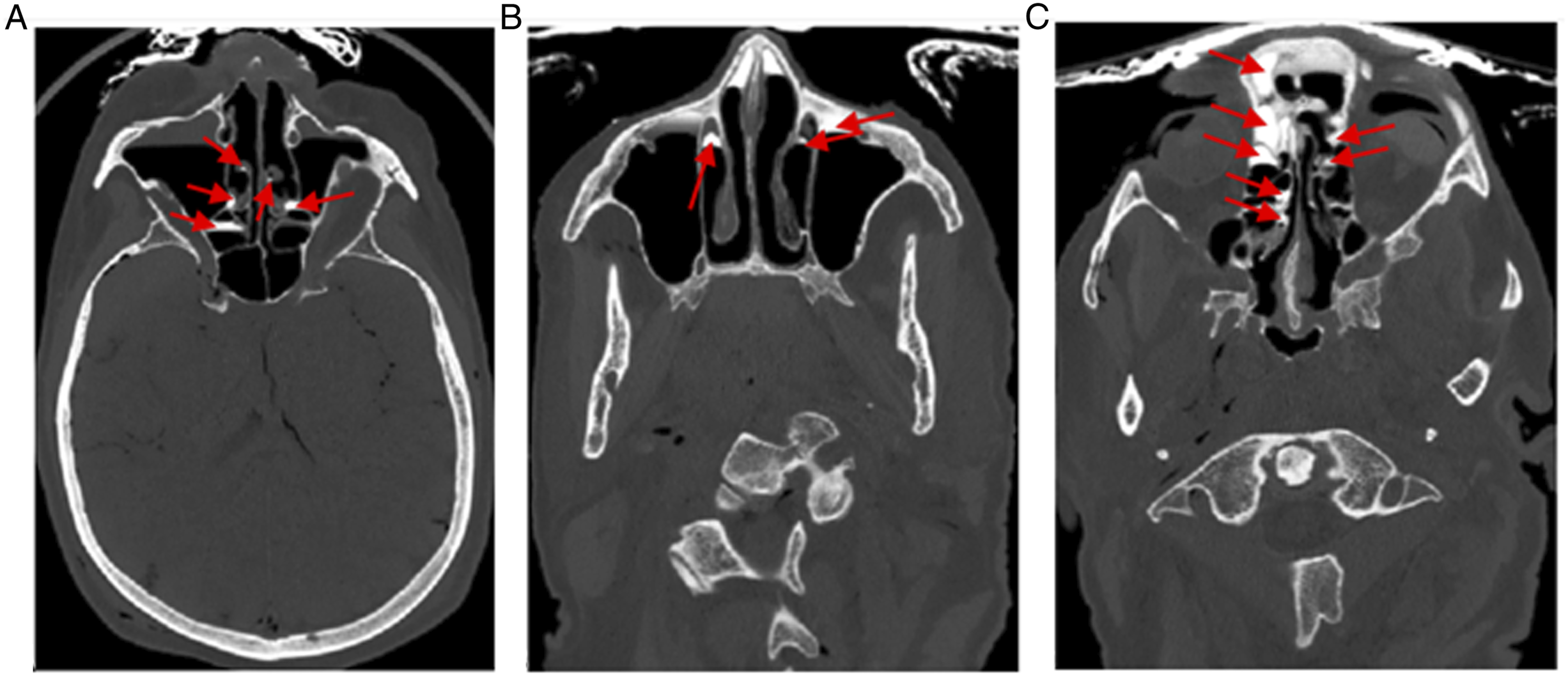
Results
Distribution of nasal irrigation into different subunits of the nasal cavity and paranasal sinuses in the two study positions. SLF: Standing leaning forward, HDF: Head down forward, IM: Inferior meatus, MM: middle meatus, SM: Superior meatus, OC: Olfactory cleft, FS: Frontal sinus, MS: Maxillary sinus, AES: Anterior ethmoid sinus, PES: Posterior ethmoid sinus, SS: Sphenoid sinus. * Indicate significant difference.
Discussion
The application of local treatments in the nasal cavity to treat or control different pathological conditions is usually part of the standard of care.1,2 Knowing the extent to which these solutions are dispersed within the sinonasal cavities by different methods is important as it helps in selection of the appropriate method. To the best of our knowledge, there are 5 studied positions for the local application of solutions: natural head (vertical plane), head-forward (almost horizontal plane), head-tipped-back, Mygind’s, and HDF positions. 1
The extent of irrigation has been studied for the operated cases and cadavers, where all sinuses are directly and widely opened to the nasal cavities.3-5 Several studies have evaluated the extent of delivery of nasal drops and sprays, which was limited to the nasal cavities and middle meatus.6-12 The extent of delivery using irrigation in non-operated sinuses has only been reported in a single study. In that study, 8 cadaveric heads were irrigated with methylene blue in a forward-tilted position and then assessed endoscopically to determine the extent of distribution of the dye within the nasal cavities. 13
We found that the HDF position allowed better delivery of irrigation to the sinonasal cavities than the SLF position. This supports the results of an earlier study by Kubba et al; 6 they studied the extent of delivery of nasal drops using methylene blue and found that the stain reached the middle meatus in the HDF position. Bateman et al 7 assessed the extent of delivery achieved in head-forward position using sprays and found that the distribution was limited to the anterior part of the nasal cavities, with poor coverage in the area posterior to the nasal valve. However, these studies did not specify whether the endoscopic assessment of the extent of distribution within the nasal cavities was performed while the head remained in the same position.
This study is the first to use CT contrast materials to assess the extent of irrigation within the sinonasal cavities. However, Rudman et al published a pilot trial on the use of cone-beam computed tomography (CBCT) to study deposition patterns of intranasal sprays and drops using radiopaque contrast material on 9 healthy volunteers. In their study, the drops were given in vertex-to-floor position, and the sprays were given in a sitting-with-upright-head position. They found that neither the drops nor the sprays reached the superior nasal spaces or the sinuses. 10 However, their assessment was prone to be affected by a change in head position after administration of the contrast material to fit for the CBCT. This positional change led to a discrepancy in the obvious distribution of the study material.
Sphenoid sinuses are poorly irrigated in either of the positions. The sphenoid sinus ostium is different than all other sinuses. It opens directly to the nasal cavity with no leading channels. Moreover, it is located high up in both irrigation positions used in the study, where the gravity may limit the reach of the irrigation into this sinus.
This study is limited by the small sample size but is similar to other reports in the literature. Other limitations include atrophy of mucosa in cadavers will allow more irrigation to enter the sinuses and may be overestimated here and clinical studies should be done. The presence of more contrast in HDF position in OC and FS could be explained by gravity, but the presence of contrast in MS contradicts that and should be considered. Using the same heads for both irrigation positions can be a limitation as well; however, suctioning of contrast material was done in between. Moreover, the trial started with leaning forward position then the HDF position in 5 heads, then started with the SLF position in the remaining 4 heads, as described in the methodology. However, the results were supporting HDF position. This is indicating indirectly a good washout.
With the findings of this trial, it was very clear that the irrigation reached more subunits in the HDF position. Considering that the inflammation will minimize this extent, with repetition of the irrigation (if it contains steroids) the inflammation will decrease. Accordingly, it is assumed that the extent will improve. Once the local treatment reached the cavities of the paranasal sinuses, the inflammatory process will be controlled from it is anatomical root, the sinus mucosa.
Conclusion
This is the first cadaveric study to radiologically assess and compare 2 different head positions effect on the extent of nasal irrigation within non-operated sinonasal cavities. The extent of nasal irrigation was statistically significant more in the HDF position. Based on our findings, the HDF position is expected to be more beneficial for sinus irrigation in a non-operated sinonasal cavity and olfactory area, while the standing-leaning position is only effective for a washout limited to the nasal cavity. Further studies comparing the clinical outcomes of both positions in non-operated patients are needed.
Footnotes
Acknowledgments
The authors extend their thanks and gratitude to the Saudi Association of Neurological Surgery for offering cadaveric heads to conduct this demonstration trial as part of the skull base surgery course.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.