
Abstract
Herein we describe a case of a 56-years old patient presented with general malaise, anorexia and progressive weight loss for about 5years associated recently with diarrhoea and repeated syncopal attacks for 1month. On admission, he had splenomegaly and his laboratory studies showed macrocytic hyperchromic haemolytic anemia [Hb = 9.4g/dl] and a significant hyponatremia [Na+ = 111mmol/l]. Endocrinological evaluation revealed an isolated adrenocorticotropin deficiency (IAD) with a manifest hypoaldosteronism. On treatment with cortisone, both anemia and hyponatremia (but not splenomegaly) were markedly improved. Our case may represent an evidence for the pathogenesis of erythropoietic dysfunction in patients of adrenocortical insufficiency.
Introduction
Impairment of adrenal cortical function may be due to intrinsic disease of adrenal gland, or may be secondary to chronic suppression of ACTH secretion or synthesis. It has been well documented that isolated deficiency of adrenocorticotropin (ACTH) is a rare cause of secondary adrenocorticotropin insufficiency it causes mild to moderate anemia that responds to hormonal replacement therapy (adrenalectomy-like effect in experimental animals) (1,9). Previous reports in the literature showed a correlation between ACTH deficiency and anaemia with a varying degree of severity according to the patient's general health condition and an associated anorexia attributed to cortisol deficiency. The actual mechanism by which ACTH deficiency affects erythropoiesis is not clear but many authors insure this effect depending on different suggestions. Although isolated ACTH frequently discussed before, our case consider as the first study reporting a case of IAD associated with haemolytic anaemia and splenomegaly, with dramatic improvement following the cortisone replacement therapy.
Case Report
A 56-years old man developed general malaise and anorexia approximately 5years prior to admission. He reported a weight loss of about 11kg with impaired mental activity during this period. He was referred to our hospital for evaluation of repeated attacks of diarrhoea of about 1month which was worsened recently and associated with lethargy and repeated sense of impending syncope. On admission he was 150cm in height and weighted 35.9kg. His blood pressure was 106/68mmHg, body temperature was 36.7C° and pulse rate was 80/min and regular. There was pale conjunctiva but no jaundice. Chest and cardiac examinations were normal. On abdominal examination, tenderness of the left hypochondrium and splenomegaly (4 fingers below the costal margin) were noticed. The spleen was soft with a smooth surface. There was no abnormal skin pigmentation or edema. The axillary and pubic hair was preserved. Neurological examination was unremarkable. The patient's family history was irrelevant.
Splenomegaly was confirmed by sonography (11.4cm × 14.4cm) and abdominal CT (Fig. 1). Hematological tests showed hyperchromic macrocytic anemia with reticulocytosis and a Haptoglobin level less than 6mg/ml while other parameters were normal (Table 1). Both direct and indirect coombs' tests were negative. Also Hams test and Sugar-water test were negative. Bone marrow examination showed cellular hyperplasia and increased reticuloblast. Based on the above data, haemolytic anaemia was diagnosed. Laboratory investigations showed marked hyponatremia (serum Na+= 111mmol/L) while the serum K+ and Cl+concentrations were 4.2mmol/L and 79mmol/L respectively. Total bilirubin was 1.7 mg/dl, hormonal studies showed a very low plasma cortisol level at the baseline (3.2 µg/dl) while ACTH level was within normal range. Serum cortisol concentration was not increased after intravenous injection of ACTH 250 µg but the urinary output of synacthen was increased to normal level after intramuscular injection of long-acting ACTH 1mg for 3 days. Plasma ACTH did not respond to neither corticotropin-releasing factor (CRF)-stimulation test (100 µg i.v.) nor hypoglycemia induced by an insulin-loading test. Serum levels of growth hormone (GH) and Luteinizing hormone (LH) were slightly higher than normal and were increased in response to hypothalamic hormones-stimulation tests (GHRH 100 µg and LHRH 100 µg i.v. respectively). The serum levels of other pituitary hormones were normal (Table 2). Magnetic resonance imaging (MRI) of the head showed a normal pituitary gland. From all these data, a partial isolated ACTH deficiency (IAD) was diagnosed.

CT of the patient showing splenomegally as indicated by the white arrows.
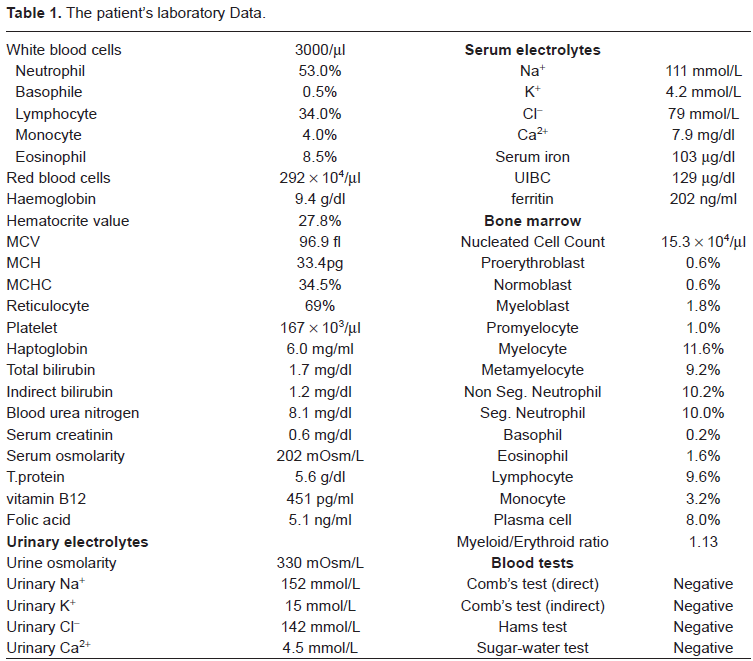
The patient's laboratory Data.
The patient's hormonal profile.

On treatment with oral cortisone (15mg/d), the patient's general health condition, anemia and hyponatremia (but not splenomegaly) were markedly improved. He was discharged after 1month on hydrocortisone-replacement therapy. Finally, his serum electrolytes, hematocrite and hemoglobin concentrations approached the normal range within about 6 months (Fig. 2). He is followed-up till now for splenomegaly.
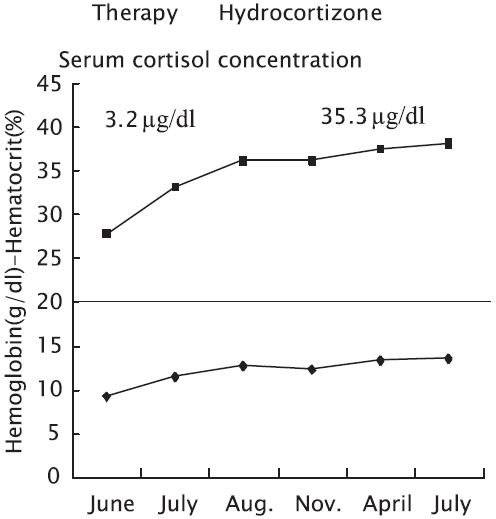
The clinical course of the patient before and after hydrocortisone replacement therapy showing an improvement in the hematocrite value, hemoglobin level and serum cortisol concentration following treatment.
Discussion
On admission, the patient presented with non-specific GIT symptoms as anorexia, nausea, progressive weight loss and diarrhoea in addition to a sense of impending syncope. We initially related the syncope to hypotension but the patient blood pressure was normal 106/68mmHg. Further examinations demonstrated macrocytic hyperchromic anemia (Fig. 2) with significant reticulocytosis and splenomegaly while the serum levels of both vitamin B12 and folic acid were normal. Also significant hyponatremia [Na+= 111 mmol/l] was detected. Both the plasma osmolarity and renin activity were low with concomitant elevation in urine osmolarity. Therefore, the syncope was attributed to both anemia and hyponatremia. Endocrinological evaluation of the patient revealed a low level of serum cortisol with normal level of ACTH. The plasma ACTH level did not respond to CRF-stimulation while other pituitary hormones exhibited normal response patterns. Synacthen level gradually increased on prolonged ACTH-stimulation test. So, we concluded a final diagnosis of partial IAD.
Isolated ACTH deficiency (IAD) a rare cause of secondary adrenocortical insufficiency is typically associated with low serum level of both cortisol and ACTH.1,8 Some reports have described that certain cases of IAD may have low normal plasma cortisol and/or ACTH level. The age incidence of IAD is variable from 45–65years, and patients are usually presented with long-standing non-specific symptoms combined with unusual clinical presentations.1,9,10
Anemia has been reported to occur in cases of IAD. In a previous study of 305 cases of IAD, the average hemoglobin concentration was 11.0 ± 1.8g/dl while very few cases showed sever anemia. 1 Currently, the pathogenesis of anemia in cases of IAD and the mechanisms by which corticotrophins affect erythropoiesis are not well-understood. Many theories had been postulated to support corticotrophin's regulatory role in erythropoiesis including: (1) Cortisol has a stimulatory effect on erythropoietin in the normal and adrenalectomized rats. 11 However; there are no records for the erythropoietin levels in such cases. (2) In addition, previous reports showed that hydrocortisone stimulates human Erythroid burst formation both at physiological and pharmacological concentrations [10−7mol/L and 10−5mol/L respectively] in normal human bone marrow culture. 13 (3) Additionally, corticosteroids significantly improve anemia in patients of immune thrombocytopenic purpura.14,15 (4) Other reports suggested that glucocorticoid may stimulate the proliferation of hemopoietic precursors, change the hemopoietic microenvironment or suppress the function of the cell that inhibits hemopoiesis. 12 This can be supported by the study of Barr et al.; who reported that the stimulation of erythropoiesis is influenced by a population of mature T-lymphocytes. 15 Also, a recent study suggested the effect of stroma cells and cytokines on regulation of hemopoiesis. 1 Our case strongly supports these suggestions as the patient was diagnosed to have haemolytic anemia which was excluded to be of auto-immune nature due to negative immunologic studies. It may be explained by the possible effect of such inhibitory cytokines and changes in hemopoietic microenvironment on RBCs survival. In this case, the patient had splenomegaly which was not improved significantly under hormonal replacement therapy. This splenic enlargement may be attributed to haemolytic anemia and extramedullary erythropoiesis.
Our results may confirm that the adrenocorticotropins have a regulatory role and are necessary for intact erythropoiesis.