
Abstract
Background:
Visceral leishmaniasis is a vector-borne disease caused by Leishmania donovani transmitted by sand fly species. It is the third most common vector-borne disease globally. Visceral leishmaniasis is endemic in Ethiopia with an estimated annual incidence ranging from 3700 to 7400 cases. This research aimed to assess the clinical presentations and laboratory profiles of visceral leishmaniasis for early diagnosis and timely initiation of management.
Objective:
To describe the clinical and laboratory manifestation and diagnostic modalities of visceral leishmaniasis among adult patients admitted to Felege Hiwot Hospital, from 1 September 2016 to 30 August 2019.
Method:
Institution-based retrospective cross-sectional study was conducted among 141 patients admitted to Felege Hiwot Hospital from 1 September 2016 to 30 August 2019. Descriptive statistics were used to describe the clinical presentation and laboratory profiles of patients with visceral leishmaniasis.
Results:
Among a total of 141 enrolled patients in the study, males were affected 13-fold. Most of them were travelers to endemic areas during the winter season for labor work. The mean duration of illness was 48 days. Common symptoms were fever (96.5%), weightless (82.5%), jaundice (18.4%), vomiting/diarrhea (13.5%), and bleeding episodes (11.3%). Splenomegaly was seen in 98.6%, ascites in 35.5%, and lymphadenopathy in 9.9%. Lymphadenopathy was seen significantly in HIV patients (40%). Anemia was seen in 95%, thrombocytopenia in 90.2%, leukopenia in 86.4%, and pancytopenia in 79.4%. Half of the patients had coinfection. Neutropenic sepsis was seen in 21.3%. The diagnosis was made by tissue aspiration in 65% of patients.
Conclusion:
The majority of patients who were diagnosed to have visceral leishmaniasis were young male adults who traveled to the endemic areas seasonally. Fever and splenomegaly were seen as the commonest clinical presentation. Lymphadenopathy occurred in high frequency among HIV co-infected patients. Anemia was the commonest hematologic finding.
Background
Leishmaniasis is the third most common vector-borne disease causing an estimated 1.98 million disability-adjusted life years and 57,000 deaths per year globally.1,2 There are two major clinical forms of leishmaniasis: cutaneous leishmaniasis (CL) and visceral leishmaniasis (VL). 3 VL which is commonly known as kala-azar is caused by Leishmania donovani, which predominantly affects tissue macrophages.4,5
The geographical distribution of the diseases depends on sand fly species acting as vectors, their ecology, and the conditions of internal development of the parasite. 6 VL is the most prevalent form in eastern Africa in general and in Ethiopia in particular. In Ethiopia, VL is reported to be widespread over the arid and semi-arid parts of the country. In Ethiopia, the annual burden of VL ranges from 2000 to 4500 cases. Some of the factors found to be associated with the spread include population movements to and from endemic focus areas, poverty, and malnutrition associated with the presence of the sand fly vector and reservoirs.7–9 Amhara region is one of the endemic regions in the country, particularly in the Humera, Metema, Libokemkem, and Fogera areas. Coinciding with the HIV epidemic, the burden of VL has dramatically increased in Ethiopia over the last 10 years.10,11 Among selected populations, such as in Humera, Ethiopia, the proportion with coinfection was 15%–30%. 12
VL is a chronic, systemic disease characterized by fever, hepatosplenomegaly, lymphadenopathy, pancytopenia, weight loss, weakness, and, if untreated, death.13–16 VL affects mainly of hematopoietic system manifested with leukopenia (96.6%), anemia (94.9%), thrombocytopenia (90.5%), and pancytopenia.17–24
VL is diagnosed using serologic tests (either direct agglutination test (DAT) or recombinant kinesin protein (RK-39) dipstick) and confirmed parasitologically by the microscopic demonstration of amastigotes of Leishmania donovani bodies in Giemsa-stained tissue aspirates of the spleen, bone marrow, or lymph node. 15 In resource-limited areas or inconclusive results, VL can be diagnosed by case definition. The VL case definition is a person who presents with fever for more than 2 weeks and an enlarged spleen (splenomegaly) and/or enlarged lymph nodes (lymphadenopathy), or either loss of weight, anemia, or leucopenia. 8 Knowing the specific clinical features and laboratory profiles of VL is important for the community for early presentation and for health professionals for early diagnosis and timely initiation of proper management of the disease condition.
Methods
Study area
The study was done at Felege Hiwot Hospital (FHH). It is one of the largest referral public hospitals in the country found in Bahir Dar, Amhara region, 565 km North West of Addis Ababa, the capital city of Ethiopia. It was established in 1963, serving more than 7 million people in the surrounding area.
Study design and period
A hospital-based retrospective cross-sectional study was done among adults with VL admitted to FHH from 1 September 2016 to 30 August 2019. The study was conducted from 1 November 2019 to 30 January 2020.
Sample size determination
All 141 patients diagnosed with VL who had a complete chart admitted to FHH medical ward from 1 September 2016 to 30 August 2019 were included as study units. No sampling technique was utilized since all cases of visceral leishmania were analyzed.
Sampling technique
Out of a total of 158 patients with VL admitted in the medical ward from 1 September 2016 to 30 August 2019; 141 patients were selected as a study sample. Others were excluded from the study.
Inclusion and exclusion criteria
Inclusion criteria
All patients with the diagnosis of VL were admitted to the FHH medical ward from 1 September 2016 to 30 August 2019.
Exclusion criteria
VL patients admitted to FHH medical ward from 1 September 2016 to 30 August 2019 and who withdraw from the management or had incomplete data charts were excluded from the study.
Operational definitions
Tissue aspiration
Samples are taken from spleen, lymph node, or bone marrow via needle aspiration and subjected for histopathologic study to diagnose leishmaniasis.
VL is a systemic parasitic disease diagnosed by visualization of amastigotes from splenic, lymph node, or bone marrow aspiration, positive rk39, and/or case definition. RK39 is a serologic rapid test done for travelers from non-endemic to endemic areas to leishmaniasis.
Withdraw from treatment
Patients left the hospital before completing the treatment or before the declaration of cure.
Data collection
Data was collected using a structured checklist from charts of adult patients admitted with VL. The data collection checklist was taken from a modified national Leishmaniasis Disease Record Form that includes patient socio-demographic information, basic clinical information at admission, leishmaniasis diagnosis, treatment, and discharge status and modified to the required variables. The data were collected by trained two BSc nurses and one BSc nurse supervisor. Data collection was done from 1 October 2019 to 31 October 2019.
Data processing and analysis
The data were entered and cleaned using Epi Data version 3.1 and exported to SPSS version 23 for further analysis. The descriptive analysis was done by simple frequencies and proportions, and the result was presented by tables and graphs.
Results
Demographic characteristics
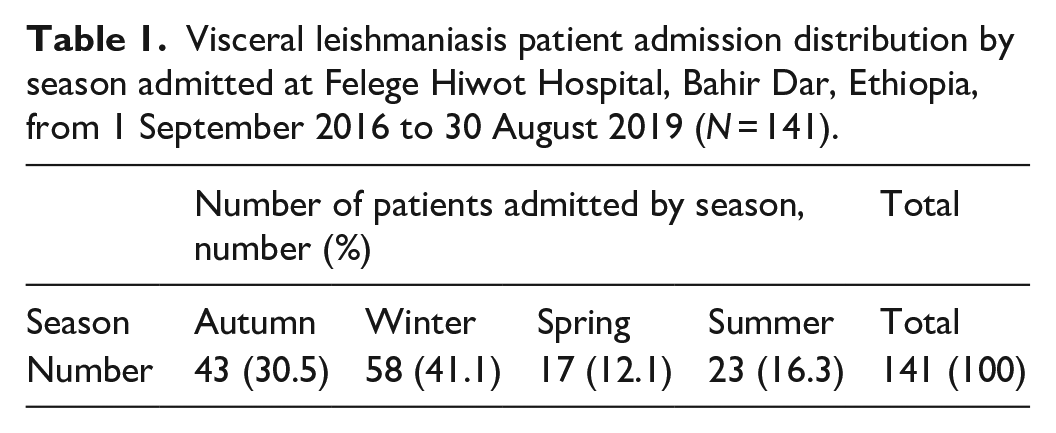
There were 131 males (92.9%) with an overall 13.1:1 male-to-female ratio. The mean age at diagnosis was 26.96 years with the age range of 18–77 years. There were 66 (46.8%) patients admitted during 2009 EC (Table 1).
Visceral leishmaniasis patient admission distribution by season admitted at Felege Hiwot Hospital, Bahir Dar, Ethiopia, from 1 September 2016 to 30 August 2019 (N = 141).
Eighty-seven percent of patients were travelers from non-endemic areas to lowland areas of northwestern Ethiopia, particularly Humera and Metema which are endemic to VL.
Clinical profiles
The mean duration of compliance before admission was 48 days with a range of 15–180 days. Fever was the most common complaint followed by weight loss among admitted patients with VL (Table 2).
Frequency of symptoms in patients admitted with the diagnosis of VL admitted at Felege Hiwot Hospital, Bahir Dar, Ethiopia, from 1 September 2016 to 30 August 2019 (N = 141).

VL: visceral leishmaniasis.
Of the total 141 studied patients, 109 patients (77.3%) had documentation on HIV status and of this 10 patients (9.2%) were tested positive. All of the patients who were diagnosed to have HIV had a history of fever during admission (Table 3). In this study, having concomitant HIV infection had no static significance for types of symptoms of VL patients (p > 0.05).
Association of clinical symptoms of VL patients with HIV status admitted at Felege Hiwot Hospital from 1 September 2016 to 30 August 2019 (N = 141).

VL: visceral leishmaniasis.
Palpable splenomegaly was seen in 139 patients (98.6%) with a mean palpable spleen size of 8.4 cm (2–21 cm). It was the most common sign of VL during the study period (Table 4).
Frequency of clinical signs in VL patients regardless of HIV status admitted at Felege Hiwot Hospital from 1 September 2016 to 30 August 2019 (N = 141).

VL: visceral leishmaniasis.
As described in Table 5, only palpable lymphadenopathy is found to be significantly associated with HIV-positive patients (9.1% vs 40%, p = 0.003).
Association of clinical signs and HIV status in VL patients admitted to Felege Hiwot Hospital from 1 September 2016 to 30 August 2019 (N = 141).

VL: visceral leishmaniasis.*p-value is statistically significant.
Of the total, 69 patients (48.9%) were having documented coinfection and neutropenic sepsis is found to be the commonest coinfection (21.3%) of all VL patients documented (Figure 1). The commonest hematologic profile was found to be anemia which was seen in 134 (95%) patients. In general, pancytopenia was seen in 112 (79.4%) patients with VL (Figure 2).
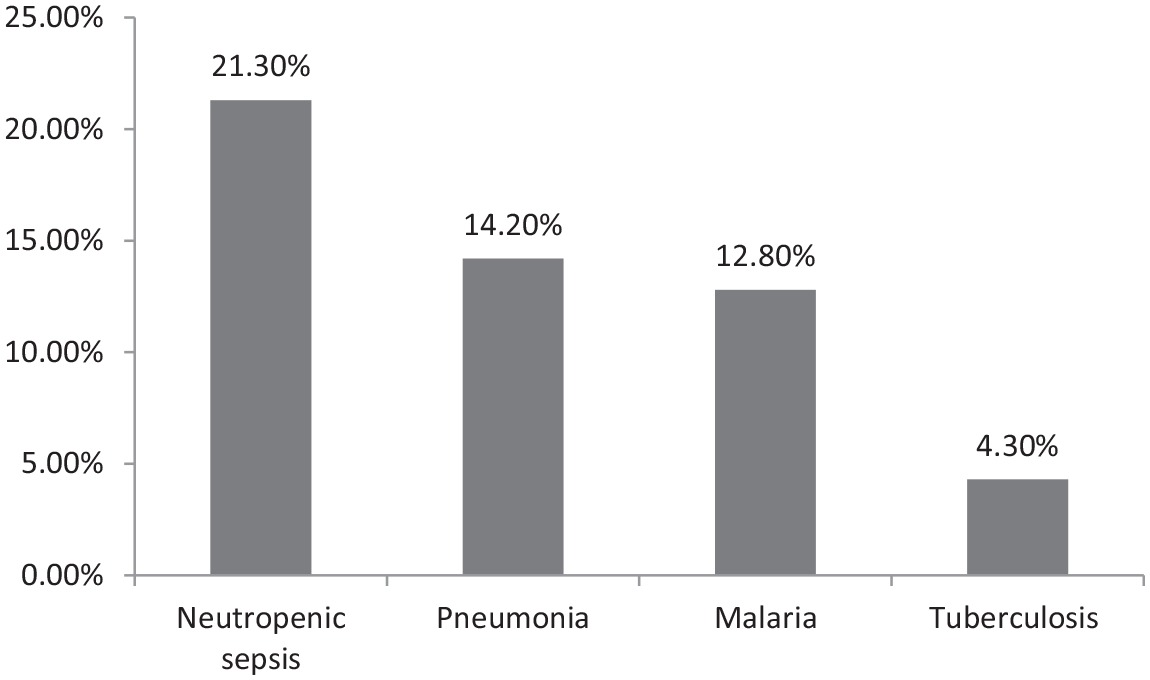
Bar graph showing rate of coinfection in VL patients admitted at Felege Hiwot Hospital, Bahir Dar, Ethiopia, from 1 September 2016 to 30 August 2019 (N = 141).

Bar graph showing the percentage of hematologic profiles in VL patients admitted at Felege Hiwot Referral Hospital, Bahir Dar, Ethiopia from 1 September 2016 to 30 August 2019 (N = 141).
Serologic test (RK39) is done in 121 (85.8%) patients and out of these 86% of patients tested positive. Tissue (bone marrow, lymph node, or spleen) aspiration was done in 99 patients (70.2%) and of these 65% of patients had confirmed VL test results. The results of 11 patients’ tissue aspirations were reported as inconclusive. Thirty (28.9%) patients had tested positive for both histopathology study and serologic test. Twenty-three and 10 patients, whose tissue diagnoses were negative and inconclusive respectively, tested positive for serology test. Among 17 patients who tested negative for serology, 15 (88.2%) patients tested positive for tissue diagnosis. There was only one patient diagnosed by the national case definition of VL with no tissue aspiration or serologic test (Table 6).
Diagnostic modalities used for VL patients admitted at Felege Hiwot Hospital, Bahir Dar, Ethiopia from 1 September 2016 to 30 August 2019 (N = 141).

VL: visceral leishmaniasis.
Discussion
This study is a 3-year retrospective cross-sectional study on the clinical and laboratory profile of 141 VL patients. The result of this study showed as the disease burden of VL still carries notable morbidity among young male adults. Demographically, males are 13-fold more affected than women. The explanation for this is that majorly young males are involved in the harvesting of crops by migrating from non-endemic to endemic areas to VL. The mean age of VL patients was 26.96 years which is consistent with the study done in Gondar University in 2010 and Tigray in 2003.20,21 The morbidity of young adults who have high working potential harms the economy. Regarding seasonal variation of admission, 41.1% of admission was during the winter season. Most of the patients (87%) were travelers from endemic to non-endemic areas to leishmaniasis which is higher than studies done in northwest Ethiopia in 2010. 15 This is could be patients who were admitted to FHH are around Bahir Dar city which is a non-endemic area to VL and those who are living in endemic areas and developed VL may be admitted to their nearby hospitals. Those seasonal migrants travel to the endemic areas for agricultural work particularly for harvesting during the summer and manifest during winter after the expected incubation period.
HIV test was done in 77.3% of patients. Out of this 9.2% of patients were found to be co-infected with HIV. The HIV co-infection rate is lower than a study done in Tigray, 2003 revealed 23% of HIV positive 20 and 38% coinfection in the study from northwest Ethiopia in 2010. 15 The low co-infection rate of HIV in this study may be due to the decreased incidence rate of HIV infection in the country. In addition, the test result was not documented in 31 patients which might underestimate the co-infection rates.
The mean duration of compliance before admission was 48 days. Fever (96.5%) was the commonest compliant and the least common was bleeding episodes (11.3%) in all VL cases and HIV co-infected cases had a usual visceral leishmania presentation as of general population which is consistent with a study done in Gondar, 2010 and a study done in Tigray, 2003.15,20 This might be due to HIV infection was not advanced as the patients were able to do agricultural labor work.
Palpable splenomegaly was seen in 98.6% of all VL patients with a mean palpable spleen size of 8.4 cm. Ascites were seen in 35.5% which are also similar in HIV-infected patients, but lymphadenopathy is dominantly seen in HIV-infected patients (9.1% vs 40%, p = 0.003). This finding is consistent with a study done in northwest Ethiopia and South Sudan, 2013 but higher than a study done in New Delhi and Greece.15,16,18,19 This is could be explained by the high probability of opportunistic infection leading to lymphadenopathy in immunosuppressed (HIV) patients in this area, but further study is needed to know the association and explanations.
Anemia was the commonest hematologic finding occurring in 95% of patients followed by thrombocytopenia (90.2%), leukopenia (86.4%), and pancytopenia (79.4%). In this study, hematologic manifestations were high compared to previous studies done in North West Ethiopia and Greece.18,19 This is likely due to late presentation which leads to bone marrow suppression by the amastigote and inflammation and splenic sequestration from huge splenomegaly.
Coinfection with another pathogen was diagnosed in nearly half of the patients and 21.3% of patients had neutropenic sepsis and all treated with antibiotics and responded. In this study, neutropenic sepsis was higher than the study done in Greece which showed 22% coinfection. 16 This could be explained by the high frequency of leukopenia predisposing to bacterial superinfection, overcrowding, and poor hygiene in this study area.
Tissue aspiration was done for 99 suspected VL patients and Leishmania donovani was seen in 64 patients (65%). The parasitological diagnosis in the study was higher than the study done in Gondar (58.9%) and lower than polymerase chain reaction (PCR) in peripheral blood (73%) which was done in Greece.15,16 The higher parasitological diagnosis in this study could be due to better pathologist experience. Out of 99 patients for whom tissue aspiration was done, 11% of patients had an inconclusive result which is possibly due to sample collection problems in the internal medicine department or sample processing and reporting problems in the pathology unit. The serologic test rk39 was done in 121 (85.8%) patients and out of this 104 (86%) patients were tested positive. This is lower than the average positivity (93.9%) of rk39 compared to the WHO rk39 sensitivity report. 22 Among 64 patients who had confirmed tissue aspiration, 15 (23.4%) tested negative for rk39. This lower positivity of RK39 could be due to immunosuppression from malnutrition, the quality of the test kit, or the technical problem of the laboratory technicians. According to the study done by Hurissa et al. in 2010, VL was confirmed parasitological only in 58.9% which is less than the result seen in this study.7,15,22 The higher positivity of tissue aspiration in this study could be from the higher experience of pathologists in detecting leishmanial species.
Conclusion
Demographical profiles of VL patients show that young males were more affected during winter following the seasonal movement for agricultural purposes. HIV status was found to be positive in 9.2% of patients. The mean duration of illness was 48 days. Fever was the commonest clinical symptom which was also consistent in HIV-positive patients. Splenomegaly was the commonest clinical sign regardless of HIV status. Lymphadenopathy was relatively more common in HIV-positive patients.
Anemia was the commonest hematologic finding. Half of the patients had documented coinfection and neutropenic sepsis was the commonest coinfection. The parasitological diagnosis was made in 65% of tissue-aspirated patients and the remaining patients were diagnosed by serology.
The inclusion of almost all of the symptoms, signs, and laboratory findings of patients with VL is the strength of this study. The limitation of this study is that the sample sizes were small and a retrospective study. The sample size was not calculated and justified as the total number of patients was small in number. HIV test which is a mandatory test according to the national guideline in patients with VL was done only for 77.3% of patients.
Recommendation
This study shows that young adults who traveled to endemic areas were affected most. It is better to work on them either in creating an alternative job in their native place or to have public awareness of the disease and to implement protective measures for migrants. Knowing the typical clinical and laboratory manifestation of VL in the presence of travel history to endemic areas is vital to diagnose VL early and timely institution of appropriate management. Lymph adenopathy occurred in higher frequency in HIV co-infected patients in this study and needs further future study.
Supplemental Material
sj-docx-1-smo-10.1177_20503121211036787 – Supplemental material for Clinical and laboratory profiles of visceral leishmaniasis among adult patients admitted to Felege Hiwot Hospital, Bahir Dar, Ethiopia
Supplemental material, sj-docx-1-smo-10.1177_20503121211036787 for Clinical and laboratory profiles of visceral leishmaniasis among adult patients admitted to Felege Hiwot Hospital, Bahir Dar, Ethiopia by Berhanu Tarekegn and Ayanaw Tamene in SAGE Open Medicine
Footnotes
Acknowledgements
The authors thank all participants of this research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was obtained from the Bahir Dar University, College of Medicine and Health Science Ethics Review Committee, but a specific ethical approval number was not given during that time.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was not taken from study subjects and it was waived by the Bahir Dar University, College of Medicine and Health Science Ethics Review Committee.
Supplemental material
Data extraction format for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.