
Abstract
Splenic cysts are uncommon and are classified as primary cysts or secondary cysts based on the presence or absence of an intact epithelial lining, respectively. Epidermoid cysts have an epithelial lining of stratified squamous epithelium and have been reported in normal and intra-pancreatic accessory spleens. An 18-year-old girl presented with a symptomatic, uncomplicated splenic cyst causing massive splenomegaly and symptoms due to mass effect. Peripheral cytopaenias and lymphoproliferative neoplasm were excluded. Preoperative computed tomography was suggestive of a large splenic cyst causing massive splenomegaly and marked loco-regional pressure effects. Open splenectomy was performed and histology confirmed an epidermoid cyst with no features of malignancy. Splenic epidermoid cysts are a rare cause of massive splenomegaly. Surgical intervention is recommended due to symptoms and the risk of complications.
Introduction
Splenic cysts are uncommon. They were originally classified by Fowler as primary cysts or secondary cysts based on the presence or absence of an intact epithelial lining, respectively. Newer classifications further subdivided primary cysts into parasitic or non-parasitic forms. Non-parasitic cysts could be congenital or neoplastic, traumatic and degenerative. Epidermoid cysts, together with dermoid and endodermoid cysts, constitute the types of congenital cysts. 1
Epidermoid cysts have an epithelial lining of stratified squamous epithelium and have been reported in normal and intra-pancreatic accessory spleens. These cysts, when small and in accessory locations, are detected incidentally during imaging. When enlarged they may present as an abdominal mass with non-specific abdominal pain or cyst-related complications. 2
This is a case of a young female presenting with massive splenomegaly due to an epidermoid cyst.
Case
An 18-year-old female was referred with progressive abdominal distension, low-grade abdominal pain and backache of 6 months. She was constitutionally well and her general examination was normal. She had a large intra-abdominal mass extending across the midline, occupying the entire abdomen except the right lower quadrant. It was smooth, firm and non-tender, with well-defined margins and percussion dullness continuously extending to the splenic region.
Her full blood count and blood picture were normal and bone marrow biopsy did not reveal a lymphoproliferative disorder. Abdominal ultrasonography showed a large cystic lesion arising from the spleen. A subsequent abdominal computed tomography (CT) scan confirmed massive splenomegaly with a large cyst measuring 9.4 × 21 × 16 cm compressing and displacing the liver, left kidney and pancreas (Figure 1). She was vaccinated against capsulated organisms and scheduled for splenectomy. Preoperative CEA and CA 19-9 were not performed. A diagnosis of a large splenic cyst causing massive splenomegaly and mass effect was made although the aetiology remained uncertain. A decision to perform surgery was made on both diagnostic and therapeutic grounds.

Contrast enhanced CT abdomen showed massive splenomegaly with a large cyst measuring 9.4 × 21 × 16 cm compressing and displacing the liver, left kidney and pancreas.
Splenectomy was performed through a midline incision (Figure 2). The early postoperative period was complicated by acute respiratory distress due to the collapse of the contralateral lung secondary to a bronchial mucus plug. Bronchoscopy and mucus plug extraction with air insufflation of the lung led to rapid improvement. She was discharged on the fourth postoperative day. The patient was followed up at a clinic level at 2 weeks, 4 weeks and 3 months post-surgery and was clinically well.

Post-splenectomy specimen.
Pathological examination revealed a spleen measuring 23 × 17 × 14 cm with a smooth outer surface and intact capsule. It contained a unilocular cyst measuring 21 × 9 × 2.5 cm with light brown fluid. Microscopy showed a fibrous cyst wall lined with squamous epithelium. The splenic parenchyma was histologically unremarkable with no evidence of malignancy. These morphological features were consistent with a primary, unilocular epidermoid cyst. Cyst fluid analysis was not performed and immunohistochemical staining facilities of the cyst wall for CA19-9 were not available (Figure 3).
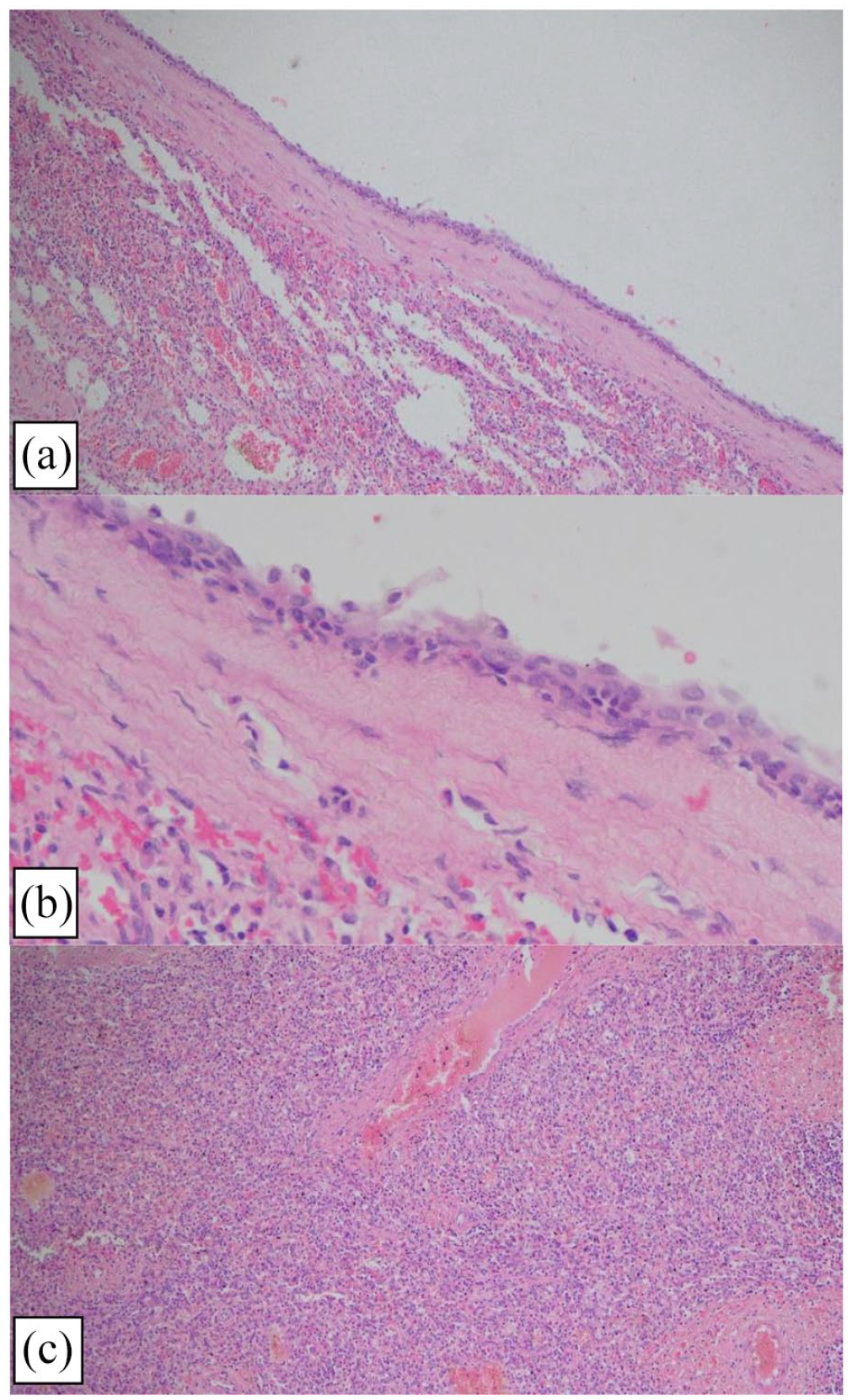
H&E staining of the specimen (a: ×40, b: ×100) revealed a fibrous cyst wall lined with squamous epithelium suggestive of a primary, benign, epidermoid cyst. (c) Normal background splenic tissue.
Discussion
Splenic cysts have been described since the 1930s, and remain a rare clinical entity.3,4 Fowler’s division of splenic cysts into true/primary cysts and false/secondary cysts based on the presence or absence of an epithelial lining remains valid to date, 3 though subdivisions have since been described. 4
Hansen et al. 4 divided primary cysts into parasitic and non-parasitic forms. Parasitic cysts are endemic to South America and the Mediterranean and are frequently caused by infection with Echinococcus granulosus. Newer classifications classify non-parasitic cysts further to congenital, neoplastic, traumatic and degenerative cysts. Congenital cysts may be epidermoid, dermoid or endodermoid cysts.1,5
Secondary cysts occur in the setting of trauma, infections such as tuberculosis, mononucleosis and splenic infarctions. Traumatic splenic pseudocysts account for 75% of all non-parasitic cysts. 1
Epidermoid cysts of the spleen, such as seen in this patient, have an overall incidence of 0.07% 5 and account for only 10% of all non-parasitic splenic cysts. They are lined by keratinizing or non-keratinizing epithelium which may be squamous or cuboidal. They are mesothelial in origin and have focal squamous metaplasia. The cyst wall is fibrotic with a variety of trabecular architecture with yellow proteinaceous content. It is thought that these congenital cysts arise from either the embryonic inclusion of epithelial cells from adjacent structures followed by cystic dilatation or due to invagination of mesothelium from the capsule surface.1,5–7 Trauma-induced squamous metaplasia of cells lining splenic sinuses is another hypothesis. 4
Epidemiologically, 67.2% of epidermoid cysts have been described in a normal spleen, and 32.2% in accessory intrapancreatic splenic tissue. More than 90% of splenic epidermoid cysts were unilocular. 2 Splenic epidermoid cysts occur mostly between the second and fourth decades with a median age at detection of 19 years and have a female preponderance of 70%. 2 This case of a large splenic epidermoid cyst is in an 18-year-old female, is unilocular, and in the normal spleen, resembling the typical epidemiology of the epidermoid cyst albeit in a slightly younger patient.
Splenic epidermoid cysts are slow-growing and grow to much larger sizes than their intrapancreatic counterparts (median size 14 vs 4.2 cm). 2 This is the basis for the latter being incidentally detected late (median age – 43 years) and being asymptomatic. 2 More than 70% of splenic cysts present as painless abdominal masses and epigastric fullness along with non-specific symptoms such as nausea, vomiting, weight loss and flatulence.2,4 Capsular stretch may result in abdominal pain. Displacement of adjacent organs such as the stomach and kidney can cause early satiety, hypertension and proteinuria. 1 Cyst complications such as rupture, bleeding and infection are responsible for emergency presentations. Rupture into the peritoneal cavity can lead to haemoperitoneum with chemical and secondary bacterial peritonitis. Transdiaphragmatic rupture can lead to haemothorax. 8 More than half of the asymptomatic group will have a palpable mass and the remainder will be detected incidentally during imaging. 2 This patient probably had the asymptomatic slow-growing phase of the cyst for several years prior until it grew large enough to occupy a significant portion of the abdominal cavity and become symptomatic, causing non-specific abdominal pain and backache and visible and palpable abdominal mass over the preceding 6-month period. Although there was no evidence of compression of adjacent viscera in the clinical history, displacement of the liver, pancreas and left kidney was evident on CT.
Contrast-enhanced helical CT delineates the cyst and its relationship to nearby structures. MRI also provides similar information but is limited in availability. 1 There are no distinctive radiological features to help differentiate these cysts from each other and malignant cysts.2,9 Hence, CT was the imaging modality of choice for diagnosis and planning of surgery. Due to constraints with availability and lack of significant additional information, an MRI was not performed.
High production of tumour antigens such as CA19-9, CEA, CA 125, CA50 is associated with true primary splenic cysts and can be found both in the serum and cyst fluid. 6 CA19-9 may be secreted by the squamous epithelial lining of epidermoid cysts and hence may be used preoperatively for diagnosis and postoperatively for surveillance. 1 Elevated CA 19-9 and CEA levels raise concern of a malignant cystic neoplasm. 2 These tumour markers lack sensitivity and specificity in the aetiological diagnosis of splenic cysts and were not performed in the current case.
Although non-operative management has been recommended by Hansen et al. for cysts <5 cm in diameter and asymptomatic cases, there is no consensus. Current reviews support surgical management for cysts >4 cm. The potential for cysts to rupture, bleed or become infected is greater with the increase in size. 5 Spleen sparing techniques, such as percutaneous aspiration, operative cyst marsupialization and fenestration, and partial splenectomy, have been described but with limited results.1,10 Percutaneous aspiration has a high recurrence rate and leads to perisplenic adhesions, making subsequent surgery challenging. The intervention has been recommended for larger cysts, even if asymptomatic due to the risks of infection, bleeding and rupture. 2 Minimal access surgery is probably better for peripherally located secondary cysts due to lesser postoperative pain and shorter hospital stays. Large, deep, primary cysts may be difficult to approach laparoscopically 1 and open splenectomy has been the historical standard for surgical management of splenic cysts.6–12 Reports show that 88.5% of epidermoid cysts were operated on due to symptoms or complications, and the remainder due to suspicion of malignancy. 2 The prognosis of splenic epidermoid cysts is good. 13
In this case, an 18-year-old girl presented with a symptomatic, uncomplicated large splenic cyst causing massive splenomegaly and symptoms due to mass effect. Peripheral cytopaenias and lymphoproliferative neoplasm were excluded by haematological and bone marrow investigations. Preoperative CT was suggestive of a large splenic cyst causing massive splenomegaly and marked loco-regional pressure effects. Open splenectomy was performed considering the size of the cyst and histology confirmed an epidermoid cyst with no features of malignancy. Epidermoid cysts of the spleen are a rare clinical entity and there is a limited understanding of its aetiology and optimal management strategy. 10
Conclusion
Splenic cysts are a rare clinical entity of which epidermoid cysts are a minority. Symptoms are related to cyst size and mass effect due to displacement of adjacent organs. The risk of complications is high in cysts more than 4–5 cm in diameter. Surgical intervention is recommended due to symptoms and risk of complications. Open splenectomy was the historical standard but spleen-preserving techniques and minimal access surgery are gaining popularity.
Footnotes
Acknowledgements
The ward team at the University Surgical Unit was involved in managing this patient.
Author contributions
D.M.G. contributed to Writing – original draft, Writing – review and editing, Visualization; S.S. contributed to Writing – review and editing, supervision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.