
Abstract
Introduction
Dilated cardiomyopathy (DCM) is associated with significant morbidity and mortality. Contrast-enhanced cardiac MRI (CE-CMR) can detect potentially prognostic myocardial fibrosis in DCM. We investigated the role of CE-CMR in New Zealand patients with DCM, both Maori and non-Maori, including the characteristics and prognostic importance of fibrosis.
Methods
One hundred and three patients (mean age 58 ± 13, 78 male) referred for CMR assessment of DCM were followed for 660 ± 346 days. Major adverse cardiac events (MACE) were defined as death, infarction, ventricular arrhythmias or rehospitalisation. CE-CMR used cines for functional analysis, and delayed enhancement to assess fibrosis.
Results
Myocardial fibrosis was present in 30% of patients, the majority of which was mid-myocardial (63%). Volumetric parameters were similar in patients with or without fibrosis. At 2 years patients with fibrosis had an increased rate of MACE (HR = 0.77, 95% CI 0.3-2.0). Patients with full thickness or subendocardial fibrosis had the highest MACE, even in the absence of CAD). More Maori had fibrosis on CE-CMR (40% vs. 28% for non-Maori), and the majority (75%) was mid-myocardial. Maori and non-Maori had similar outcomes (25% vs. 24% with events during follow-up).
Conclusions
DCM patients frequently have myocardial fibrosis detected on CE-CMR, the majority of which is mid-myocardial. Fibrosis is associated with worse outcome in the medium term. The information obtained using CE-CMR in DCM may be of incremental clinical benefit.
Introduction
Dilated non-ischaemic cardiomyopathy (DCM) is associated with significant morbidity and mortality. 1 Contrast-enhanced cardiac magnetic resonance imaging (CE-CMR) can detect myocardial scar in vivo with high sensitivity, specificity and spatial resolution, 2 and has the potential to provide diagnostic and prognostic information in this group of patients. Initial reports using CE-CMR suggest that approximately one third of patients with DCM may have myocardial scar, as detected by late gadolinium enhancement (LGE). 3 It has been suggested that the presence of LGE has incremental prognostic implications, 4 and may identify those with DCM at risk of progressive deterioration. We further evaluated this hypothesis in New Zealand patients, including an important cohort of Maori, investigating the frequency and characteristics of LGE, and assessing its prognostic importance in medium-term follow-up.
Methods
Patients
Patients with DCM (n = 103) were prospectively identified between December 1st 2003 and August 31st 2006. Patients were included in the analysis if they had: (a) a clinical presentation of heart failure (b) an echocardiogram demonstrating impaired left ventricular systolic function (ejection fraction <50%) (c) successfully completed a CE-CMR. Patients were excluded if: (a) they had significant coronary artery disease (>50% diameter luminal stenosis in any coronary artery) documented on angiography (b) significant valvular disease (c) cardiomyopathy of known cause including hypertrophic, alcohol- or chemotherapy induced or infiltrative myopathies. Patient events were determined from record review, and all patients continued to undergo follow-up at our institution. The institutional Ethics Committee approved this analysis.
Major adverse cardiac events (MACE) were defined as death, cardiac transplant, sustained ventricular arrhythmias, or rehospitalisation for heart failure.
Cardiac MRI
CE-CMR was performed on a Philips Intera 1.5Tesla magnet using a Synergy Cardiac Coil (Philips, Best). Electrocardiographically gated steady state free precession cine images were acquired in the 2 and 4 chamber, left ventricular outflow tract and short axis views. The sequence parameters were: flip angle 65°, TE = 1.64 ms, TR = 3.3 ms, slice thickness 8 mm. Delayed enhancement imaging was performed after injection of 0.15 mmol/kg gadolinium-based contrast agent (Omniscan, Nycomed Amersham, Oslo). A three dimensional inversion-recovery segmented gradient echo sequence was used in 2 and 4 chamber, left ventricular outflow tract and short axis views. Imaging was commenced 10 minutes after contrast administration using an inversion time optimised to obtain adequate nulling of normal myocardium (260-340 ms). The imaging sequence parameters included an in-plane voxel size 1.2-1.8 × 1.2-1.8 mm2, slice thickness 6 mm, flip angle 15, TE = 3-4 ms, and TR = 8-9 ms. A Philips EzyVision workstation was used for image analysis. LV end-diastolic volume, LV end-systolic volume, LV ejection fraction were calculated from the short axis cine images. Areas of LGE were defined as subendocardial, mid-myocardial or transmural on visual analysis by a consensus of two independent cardiologists.
Statistics
Data are expressed as a mean ± standard deviation (SD). The baseline characteristics of the groups were compared with the independent sample t-test for continuous variables, and Chi-square or Fisher Exact tests for categorical variables. Survival estimates and event rates were compared by the Kaplan-Meier method. The log-rank test was used to compare the Kaplan-Meier survival curves. The duration of follow-up was the day of the CE-CMR scan to August 31st, 2006. A P value of <0.05 was considered significant.
Results
The clinical characteristics of the entire cohort are summarized in Table 1. The mean age was 58 + 13 years, with the majority being male and NYHA Class I. Twenty patients (19%) were New Zealand Maori. The latter were predominantly younger men (mean age 48 ± 16 vs. 61 ± 11, P < 0.05), and had significantly higher rates of diabetes and smoking (Table 2).
Baseline characteristics: entire cohort.

Baseline characteristics: Maori vs. non-Maori.

P < 0.05.
The CE-CMR results are presented in Tables 3 and 4. Myocardial LGE was present in 31 (30%) patients, and was mid-myocardial in 21 patients (20%), transmural in 7 patients (7%) and subendocardial in 3 patients (3%). Representative images of LGE in each category are illustrated in Figure 1. Volumetric measurements were similar in those with or without LGE. A higher proportion of Maori had LGE (40% vs. 28% for non-Maori, P = ns), and the majority was mid-myocardial (75%). Maori patients had significantly larger LV volumes and worse systolic function than non-Maori.
CE-CMR results and MACE: entire cohort.

CE-CMR results and MACE: Maori vs. non-Maori.

P < 0.05.
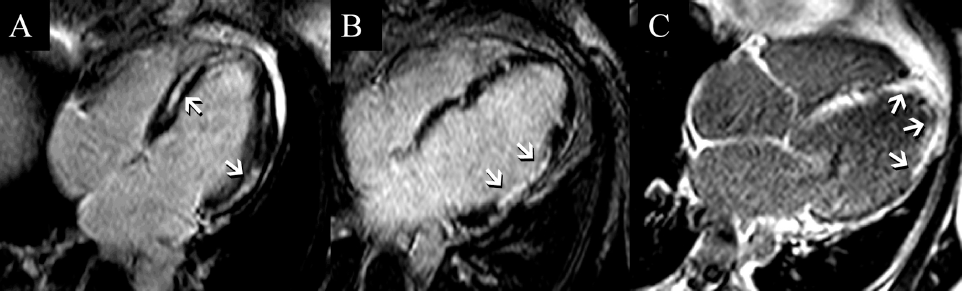
Representative CE-CMR four chamber images of three patients with DCM and no coronary artery disease demonstrating (
The mean duration of follow-up was 660 ± 346 days. There were 9 deaths and LGE was present in 2. There was no significant difference in all-cause mortality between patients with and without LGE (P = 0.58). There was a trend towards a greater occurrence of MACE (Hazard ratio 0.77; 95%CI 0.29-1.97, P > 0.05) in patients with LGE (Fig. 2). Notably there was a higher incidence of ventricular arrhythmias in patients with LGE, although this did not reach statistical significance. The worst outcomes were found in patients with transmural LGE, despite the proven absence of coronary artery disease in this group (Fig. 3). Despite the large ventricular volumes and greater incidence of LGE, outcomes were similar for both Maori and non-Maori (25% vs. 23% MACE during follow-up, P = ns). (Fig. 4)

Kaplan-Meier analysis demonstrating event free survival in patients with or without myocardial LGE detected by CE-CMR.

Kaplan-Meier analysis demonstrating event free survival in patients with LGE, stratified by LGE location.

Kaplan Meier analysis demonstrating no significant difference in event free survival between Maori and non-Maori.
Discussion
This study demonstrates that CE-CMR imaged LGE consistent with myocardial fibrosis is found in nearly one third of DCM, and that both the presence and pattern of LGE are associated with medium-term prognosis. The study also highlights potentially important differences in the morphology of DCM between Maori and non-Maori patients.
The overall occurrence of LGE (30%) was similar to that noted in previous studies of Assomull et al 4 and McCrohon et al, 3 but less than reported by Wu et al (42%). 5 The pattern of LGE was also similar to that previously described, with the majority of fibrosis being located in the mid-wall but a significant minority being transmural (23% of patient with LGE). The potential mechanisms for mid-wall fibrosis have been considered to include: exposure to pathogens and toxins, microvascular ischaemia, abnormal immune and metabolic responses such as renin-aldosterone system overactivity, and genetic factors.6–10 In particular CE-CMR imaging in patients with acute myocarditis may show mid-wall and epicardial LGE that persists in convalescent imaging. 11 Subclinical myocarditis has been implicated as the aetiology of DCM in a significant proportion of patients, 12 and the similarity in LGE findings on CE-CMR would support this. The finding of transmural or subendocardial fibrosis in the absence of obstructive coronary disease has also been described.3,13 It is postulated that this may result from thrombosis and subsequent recanalisation associated with coronary atheroma, or coronary embolus.
The finding of an association between adverse prognosis and the presence of LGE on CE-CMR confirms the results of studies by both Assomull et al 4 and Wu et al. 5 Our results do not meet a threshold of statistical significance, but the reasons for this are unclear. Our population may be a lower risk cohort to that in both prior studies. The majority of our patients were asymptomatic (NYHA Class I 75%, as compared with 15% in Wu et al 5 and 23% in Assomull et al 4 ), and ventricular function was better (Wu et al: ejection fraction 22% in LGE positive patients vs. 32% in our group). Overall event rates in follow-up are lower in our cohort (Assomull et al 26% vs. 21% in this study). A lower risk profile for the study population may have attenuated the prognostic impact of LGE. The higher rate of ventricular arrhythmias in our LGE positive patients is consistent with prior data from CE-CMR studies, but should also be interpreted with caution given the low numbers in this study. Partial thickness LGE on CE-CMR has been shown to correlate with inducible VT in patients with DCM, 14 as has infarct tissue heterogeneity. 15 An increase in scar-related re-entrant ventricular tachyarrhythmias in LGE positive patients has also be shown in other forms of myocardial disease, including hypertrophic cardiomyopathy. 16 Our data also raise the possibility that the pattern of LGE has an impact on prognosis, a finding not previously noted in this context. However the small numbers of events limit interpretation of this result.
Our study includes the largest reported cohort of New Zealand Maori patients with DCM studied by CE-CMR. The imaging findings in this group suggest more severe disease, although the prognosis was similar for Maori and non-Maori. The reasons for the higher prevalence of LGE and worse ventricular volumetric results in Maori are not clear. Potentially these findings may reflect a more advanced stage of disease, suggesting that Maori patients are coming to clinical attention later. However if this were the case we would have expected to observe a worse outcome for Maori—even in the intermediate term. Other possibilities include an alternative aetiology of DCM in Maori, such as a greater prevalence of subclinical myocarditis, or a differing genetic predisposition, but this study unfortunately provides no evidence to support or refute those hypotheses. Further studies should be considered in this population.
Limitations
This is a small retrospective study, and suffers from the potential biases inherent in such a review. MACE have been determined from chart review and may be inaccurate. Lack of consistently recorded measurements of height and weight limits the calculation of indexed ventricular volumes on CE-CMR, and makes direct comparison between Maori and non-Maori difficult.
Conclusions
Patients with DCM frequently have myocardial fibrosis detected on CE-CMR, and the occurrence and pattern of this fibrosis is associated with worse outcome in the medium term. Maori patients have a higher prevalence of fibrosis but similar prognosis to non-Maori. The information obtained using CE-CMR may be of incremental clinical benefit in patients with DCM.
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.
Footnotes
Acknowledgements
There was no financial support for this project.