
Abstract
Randomized clinical trials (RCTs) with first- and second-generation drug-eluting stents (DESs) confirmed the superiority of coronary artery bypass surgery (CABG) in patients with multiple vessel disease. In spite of different DES designs, investigators in these trials used similar percutaneous coronary intervention (PCI) strategies hoping to achieve complete revascularization, meaning that all intermediate lesions would be stented. One of these studies also included small vessels in the revascularization policy. On this revision, authors searched for a potential explanation of these intriguing findings and also for solutions to this problem, not seen years ago when other RCTs compared CABG with PCI in the previous DES era. After they revised old and new scientific data, they concluded that improved DES design is not itself enough to narrow the gap between PCI and CABG and that in the future RCTs we should institute more conservative strategies avoiding unnecessary multiple DES implantation.
Keywords
It has almost been 25 years since the first randomized clinical trials (RCTs) comparing coronary artery bypass surgery (CABG) with coronary balloon angioplasty (POBA) in multiple vessel disease were published.1–5
During those years, several RCTs between percutaneous coronary intervention (PCI) – with either POBA or bare metal stents (BMS) – versus CABG in patients with a clinical indication for myocardial revascularization were conducted, and they consistently showed a similar comparative long-term incidence of death and myocardial infarction (MI), in spite of a greater number of repeat revascularization procedures with PCI. In these trials, the extent of coronary artery disease (CAD) was not associated with a better survival with CABG, and only diabetic patients had an inferior survival after percutaneous procedures.3,5–10 In addition, results from merged data of RCTs between BMS versus CABG in multiple vessel disease population (ARTS, 11 ERACI II, 12 MASS, 13 and SoS 9 ), published in 2008 by the investigators of these trials, 14 did not show any differences between both revascularization strategies in either death (91.8% and 91.5%, respectively, P = 0.78) or death/MI/stroke (83.3% and 83.1%, respectively, P = 0.64).
Furthermore, with the composite end point of death/MI/stroke, there was no interaction between diabetics and nondiabetics with either of the revascularization strategies (P 0.65).
With the introduction of drug-eluting stents (DESs) in clinical practice, the superiority of effectiveness of DESs over BMS has been largely demonstrated in head-to-head comparison in several RCTs as well as in observational studies and meta-analysis.15–19 Therefore, we would expect a substantial improvement in PCI results over CABG, narrowing the gap of recurrences in favor of CABG.
However, that was not the case and, on the contrary, all RCTs and observational studies between DESs and CABG showed that the gap in the rate of recurrences remained and there is an unexpected increased rate of cardiac death and MI in patients treated with DESs in both diabetic and nondiabetic patients.20–23
One of the explanations for this phenomenon was that, with no doubt, first-generation DESs were associated with an unacceptable high rate of stent thrombosis (SET); overall SET incidence was 15.4% at five years in the SYNTAX trial, which was related to an increased incidence of cardiac death and MI. 24 In recent years, however, new-generation DESs significantly improved safety compared to the original ones, in terms of stent malapposition and stent strut coverage, which was reflected in a significant lower incidence of late and very late SET as well as the requirement for long-term dual antiplatelet therapy,25–27 although neoatherosclerosis was present. 28
New randomized trials with these new-generation DESs29,30 were conducted, and one of them recently published the long-term outcome.
The BEST trial randomized patients with two- and three-vessel disease to either PCI with everolimus-eluting stents (EESs) or CABG. 30 In spite of better DES design compared to the previous ones, PCI patients had again a significant greater incidence of spontaneous MI (P = 0.004) and new revascularization procedures (P < 0.001) than CABG patients. In addition, although death rate was not significantly different, it was indeed greater with PCI. In this trial, completeness of revascularization required all intermediate lesions to be stented; therefore, stent length was 85.3 mm. Stent length in this study suggested that they used a similar PCI strategy that the SYNTAX trial did (86.1 mm), although, in SYNTAX, 33.3% of patients had more than 100 mm of stent deployed; 20 contrary to SYNTAX, the BEST trial included patients with two-vessel disease and excluded patients with left main stenosis.
Even more recently, authors of the SYNTAX and BEST trials published a pooled data from an individual patient level of these two RCTs comparing CABG versus DESs in patients with multiple vessel disease in the subgroup of nondiabetic patients. 31 The BEST trial, which excluded diabetics, provided all patients for the analysis, whereas in SYNTAX only patients with three-vessel disease and no diabetics were included. Needless to say, nondiabetic patients have been largely considered the most favorable patients to be treated with PCI. 10
The pooled data advantages of CABG over PCI went across major subgroups including DES design and, most important and surprising, showed no trial interaction (P 0.913) for the primary outcome of death and death/MI/stroke all in favor of CABG (P 0.037 and P = 0.011, respectively). Furthermore, a remarkable lower rate of MI in CABG was seen (P < 0.001) mostly driven by the occurrence of spontaneous MI after 30 days in the PCI group (P < 0.004).
Many interventional cardiologists, including us, are deeply concerned and disappointed with these intriguing findings. So what would then be the potential message for the cardiology community? Maybe, even in the new DES era, the superiority of CABG over PCI in multiple vessel disease is still undisputable across all subgroups of patients.
Is that the True and Simple Answer?
What was different in PCI between the two merged analysis described above?14,31 We may argue that patients treated with DESs had more three-vessel disease (87.3% vs. 36.1% with BMS) and perhaps a higher SYNTAX score than those treated with BMS (in fact, we will never know which was the SYNTAX score for them). However, on the other hand, BMS pooled data also included diabetic population (18.1% vs. 0% with DESs) and more frequently compromise of proximal LAD stenosis (90% vs. 59% with DESs).14,31
The fact that first-generation DESs were used in SYNTAX trial could be one of the most attractive explanations; in fact, SYNTAX patients with definitive SET (6.8%) had 35.4% occurrences of cardiac death. 24 However, that was not the case with EES used in the BEST trial, which significantly improved safety compared to the first designs. Therefore, perhaps, stent design itself is not solely the reason for the poorer long-term outcome data of these two RCTs.
If we analyze the trial methods,21,30 in spite of different DES designs, both studies share similar PCI strategies, meaning that the goal was to achieve complete anatomic revascularization defined by authors “as not any residual stenosis 50% in any major coronary artery or their large branches” 30 ; consequently, we can assume that many intermediate lesions were stented and that concurs with the similarity of stent length in both studies.
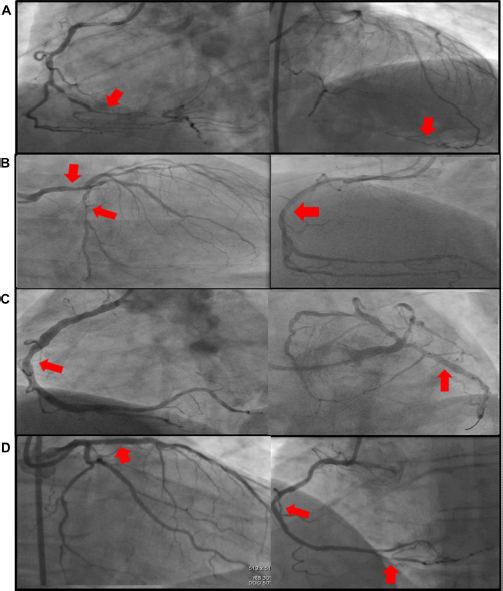
When we analyze completeness of revascularization with PCI, 1 we should take into account several different situations such as the amount of myocardium at risk or stenosis severity of the lesions not included in the revascularization strategy. Prognosis in patients with incomplete revascularization should be different if the not-attempted vessels had a complete chronic closure with collateral circulation (Fig. 1A), high-degree stenosis in a large vessel (Fig. 1B), intermediate stenosis in a large vessel (Fig. 1C), or severe stenosis in a small branch (Fig. 1D). Differences in the amount of completeness of revascularization with both, PCI and CABG, was present in all RCTs since the first study was performed; however, in the past, such differences were not associated with poorer outcome4,14 (53.2% with PCI vs. 82.7% with CABG, P = 0.0003, see Table 1). Furthermore, the fact that only 56.7% and 50.9% of SYNTAX and BEST patients, respectively, in the PCI arm achieved the goal of complete revascularization demonstrated how difficult it is for PCI to achieve such aim. 31
Completeness of revascularization of randomized clinical trials and registries between percutaneous coronary interventions (PCI) and coronary artery bypass surgery (CABG).
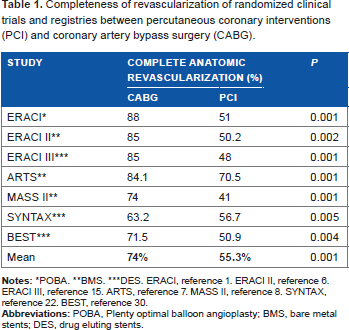
POBA.
BMs.
DES. ERACI, reference 1. ERACI II, reference 6. ERACI III, reference 15. ARTS, reference 7. MASS II, reference 8. SYNTAX, reference 22. BEST, reference 30.
Therefore, improved DES design is only one face of the problem, while changing PCI strategies using a more conservative policy during DES implantation would be the other.
If We Combined Both, We May Improve the Long-Term PCI Outcome
The ERACI IV study,32,33 with a patient population of multiple vessel disease and left main stenosis, used a second-generation DES and a conservative PCI strategy, defined as stenting only severe lesions (visually ≥70%) in large vessels. Intermediate (>50 to <70) lesions in small or large vessels or severe lesions in small vessels (<2.0 mm) were not included. The results coincide with the stent length of the study: 41.7 mm. This PCI strategy of not scoring lesions not included in the revascularization strategy allowed to build a new scoring system where low SYNTAX score was found in 54% of patients and only 17.2% of patients persisted with high SYNTAX score. 34
Investigators of ERACI IV, at more than two years of follow-up, reported remarkable low rates of adverse events including death/MI/stroke of 3.9%, unplanned new revascularization of only 4%, and death/MI/stroke/target vessel revascularization (TVR) of 6.7%. It is important to note that there was no major penalty for this conservative policy as it was reflected by the low TVR rate in the not-stented intermediate lesions (1.3%).
We do not know whether these results will remain at a five-year follow-up, although at the present time, the low rate of events in the not-stented lesions supports the PCI strategy of this study. In agreement, FAME investigators largely demonstrated that nonischemic lesions had better outcome when they were not treated with DESs.35,36
We have to take into account that, even in the era of safer DESs, neoatherosclerosis as a consequence of DES implantation has not disappeared. 28
To recap, interventional cardiologists have been doing a lot of work during this 25-year journey trying to close the safety/efficacy gap between PCI and CABG in patients with multiple vessel disease and, looking at long-term results from RCTs with the old and new DESs, we may conclude that improved stent design alone is not enough to narrow the gap between PCI and CABG. 37
New revascularization strategies during PCI and the search for a more functional revascularization avoiding unnecessary DES implantation should be the new goal for future randomized comparisons between PCI and CABG.
The game between PCI and CABG is not over.
Author Contributions
Conceived and designed the experiments: AER. Analyzed the data: AER, HP, JDP. Wrote the first draft of the manuscript: AER. Contributed to the writing of the manuscript: HP, JDP. Agree with manuscript results and conclusions: AER, HP, JDP. Jointly developed the structure and arguments for the paper: AER, HP, JDP. Made critical revisions and approved final version: AER. All authors reviewed and approved of the final manuscript.