
Abstract
We assessed the effect of the topical application of epsilon-aminocaproic antifibrinolytic acid (EACA) on the pericardium of patients submitted to coronary artery bypass graft (CABG) without the use of cardiopulmonary bypass (CPB). This is a prospective, randomized, and double-blind study. We evaluated 26 patients with chronic coronary heart disease indicated for CABG without CPB (EACA and placebo groups). The analysis of the postoperative hematological results showed no difference between groups in hemoglobin and hematocrit. There was no difference between the groups regarding the postoperative bleeding through the drains in the first 24 hours, 48 hours, and accumulated loss until removal of drains. The use of EACA in patients undergoing CABG without CPB presented no difference in the reduction of the amount of bleeding and the need for blood transfusions.
Introduction
Bleeding remains a common complication in the postoperative period of coronary artery bypass graft (CABG), 1,2 mainly when associated with the use of cardiopulmonary bypass (CPB) with increased fibrinolytic activity, thrombocytopenia, and platelet dysfunction. Some strategies to control postoperative bleeding demonstrated, when effective, to reduce perioperative morbidity and mortality, decreased the need for surgical interventions and hospitalization time. 3 –7
Aprotinin was the most widely used agent, with significant reduction of postoperative bleeding. 8 –12 However, recent reports showed uncertainty in the safety of parenteral use due to increased risk of acute graft thrombosis, acute and chronic renal failure, cerebrovascular events, and death, indicating the withdrawal of aprotinin from the market. The use of these agents topically in the pericardial cavity presented minimal plasma measurements 2 hours after administration, possibly representing an acceptable alternative. 8,10,13 –22
In an attempt to decrease the fibrinolytic activity, thrombocytopenia, and platelet dysfunction, CABG without CPB has been adopted more frequently around the world, according to the meta-analysis by Omar and Taggart published in 2009. 26 Despite the small amount of fibrinolysis caused by CABG without CPB, the effect of antifibrinolytic agents has not been extensively tested in those patients. Therefore, we aimed to evaluate the effect of the topical application of epsilon-aminocaproic antifibrinolytic acid (EACA) in the pericardium of patients undergoing CABG without CPB on the reduction of postoperative bleeding.
Method
Between October 2008 and February 2010, 26 patients with chronic coronary heart disease indicated for CABG without CPB were enrolled in a prospective, randomized, and double-blind study. They were divided into 2 groups, EACA versus placebo, assessing the volume of postoperative bleeding by thoracic and mediastinal drains and the need for blood transfusion and blood products. The randomization method adopted was a lottery. No member of the surgical team who had access to the patient knew the randomization group drawn.
We considered the following exclusion criteria: previous diagnosis of coagulation disorder with a history of bleeding and/or changes in laboratory tests, associated operations (other than CABG), minimally invasive CABG, reoperations, intensive care or emergency procedures.
The study protocol was approved by the ethics and research committee at the ABC faculty of medicine (protocol number: 376/2007), and the patients agreed to participate in the study by signing an consent letter.
All patients were followed during their hospital stay by the same member of the surgical team, who filled out a protocol for pre- and postoperative data comparison.
Surgical Technique
The procedures began with hemodynamic monitoring with measurement of mean arterial pressure, central venous pressure, urine output, and pulse oximetry. The surgical procedure was performed in the usual manner, with a median sternotomy in all cases, with 200 IU/kg of heparin administered and complete anticoagulation reversal at the end of operation using protamine sulfate (1:1). In all cases, the anastomosis was performed with individual sutures and with the aid of a mechanical stabilizer (Octopus, Medtronic Inc, Mineapollis). The proximal anastomoses were all performed in the aorta and side branches of the internal thoracic artery were ligated with cotton suture in all patients, and the heparinization reversal was confirmed by measuring the activated clotting time (80-120 seconds). At the end of the procedure, the patients were referred to the postoperative care unit.
In all the cases, the anesthetic technique used was balanced general anesthesia with inhaled sevoflurane gas, induction of hypnosis with etomidate and fentanyl, and intravenous muscle relaxant rocuronium.
Pharmacological Protocol
After randomization, a paramedic not directly involved in the study prepared the medication to be used in a proper location outside the operating room. In accordance with doses in previous published work 14,23 , a saline solution containing 24 g of EACA (total volume 250 mL, dose of 0.096 g/mL) or only saline solution (also 250 mL) was prepared in a flask without the knowledge of the surgeon.
The container containing the solution was then sent to the operating room with only an ID number, maintaining the characteristic of colorless solution. None of the members of the surgical team or postoperative unit were aware of the contents of the solution.
After the reversal of the systemic heparinization and before closing the sternum, the colorless solution was poured directly into the pericardial sac and aspirated by the mediastinal drain tube after the complete closure of the incision, affecting a total drug exposure time of 10 minutes in all patients.
In all patients, anticoagulant therapy of 100 mg of aspirin daily was stopped 5 days before the operation and resumed 24 hours after the procedure. No patient was taking any other platelet anticoagulant.
Statistical Analysis
In order to verify the probability that a statistical analysis will be able to catch false null hypotheses, that is, to determine how big a sample size should be selected for the study, we applied the power test, which provided a minimal number of 21 patients. The choice of measures of central tendency and dispersion of the values that make up the samples, as well as statistical tests for comparison between them, were based on the type of distribution using the Kolmogorov-Smirnov normality test. SPSS version 13.0 (SPSS Inc, Illinois) was used for all data analysis. The values obtained by study of each quantitative variable were organized and described by the mean and standard deviation. For the qualitative variables, absolute and relative frequencies were used.
Comparisons of frequency of events between groups of qualitative variables were performed by applying the Fisher exact test and chi-square test. To compare the means of 2 sample populations, the Student t test and Mann-Whitney U test for parametric and nonparametric variables were used, respectively. Differences were considered significant for values of P < .05.
Results
The clinical and demographic profiles of the 2 groups (EACA and placebo) are described in Table 1, and there was no statistically significant difference between the groups, confirming the homogeneity of the sample.
Clinical and Demographic Characteristics of the Patients.
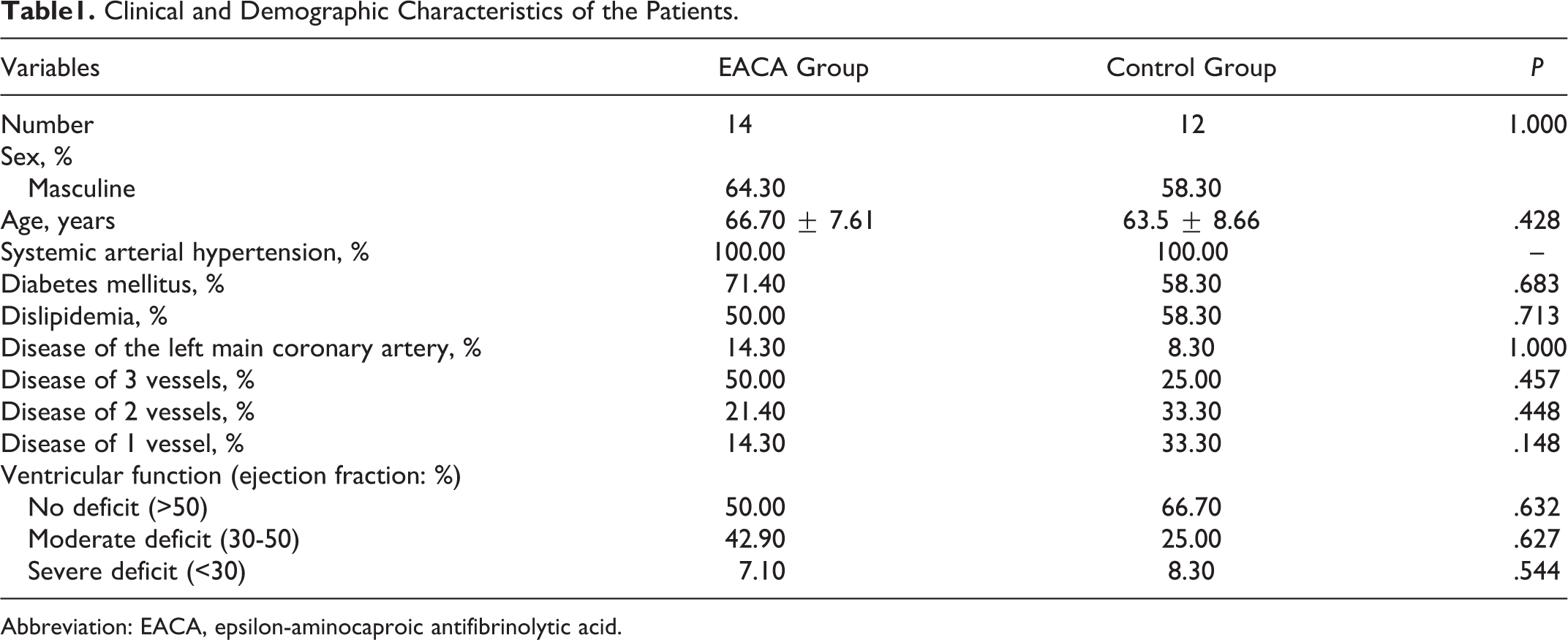
Abbreviation: EACA, epsilon-aminocaproic antifibrinolytic acid.
Regarding the laboratory comparison of preoperative hematological characteristics, no statistically significant difference was observed in hemoglobin, hematocrit, and coagulation values. The only variable with a statistically significant difference was the previous platelet dose greater in the EACA group when compared to the placebo (Table 2). We also found no difference between preoperative and postoperative conditions (P >.05).
Preoperative Hematological Characteristics.
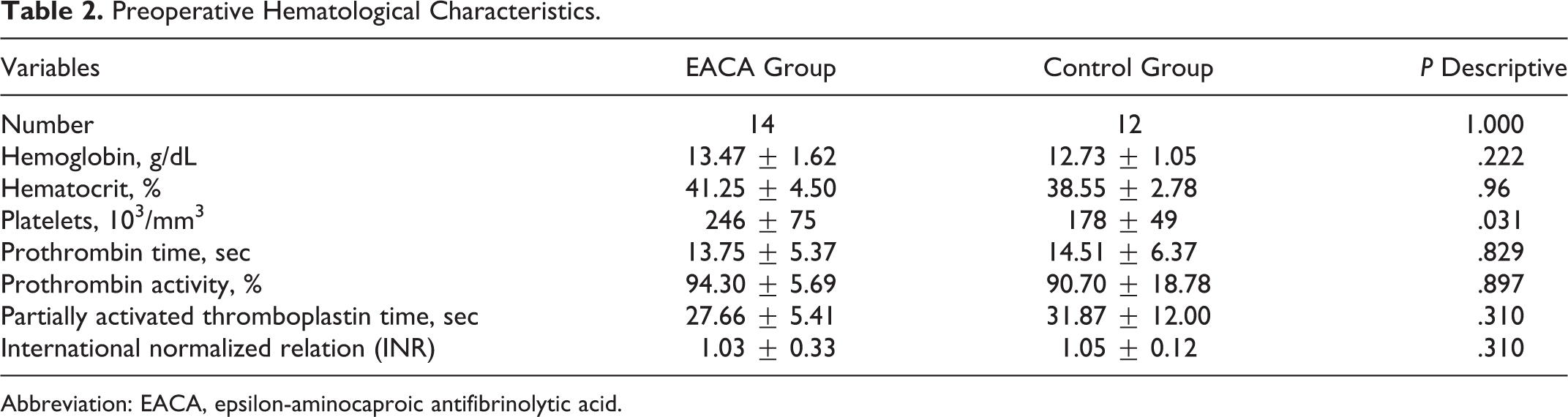
Abbreviation: EACA, epsilon-aminocaproic antifibrinolytic acid.
The analysis of the postoperative hematological results showed no statistically significant difference between the EACA and the placebo groups in hemoglobin and hematocrit values. No patient had reoperation for hemostasis repair. The postoperative bleeding through the drains in the first 24 to 48 hours and accumulated loss until removal of the drains showed no statistically significant difference when comparing the groups (Table 3).
Postoperative Hematological Characteristics and Flow Through the Drains.
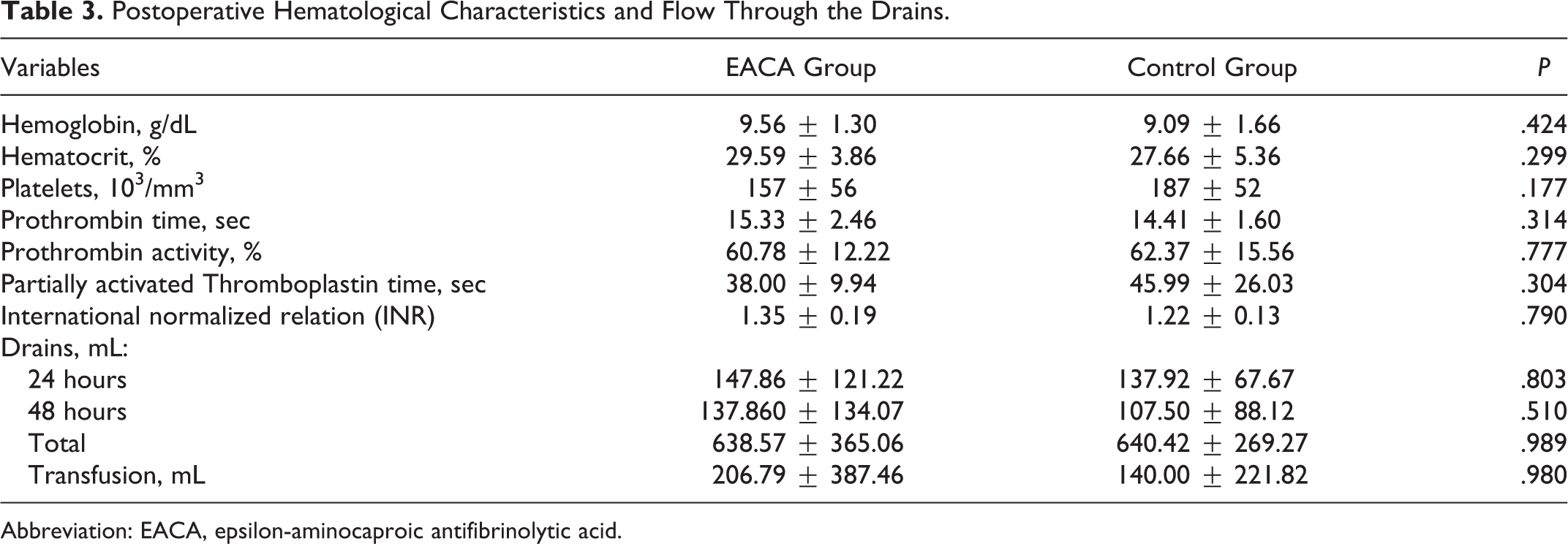
Abbreviation: EACA, epsilon-aminocaproic antifibrinolytic acid.
We applied the Pearson correlation test and found no association between the blood variables and surgical procedure duration, blood glucose levels, and left ventricular dysfunction.
Discussion
This study was undertaken to investigate the effect the topical application of EACA in the pericardium of patients undergoing CABG without CPB. Regarding the preoperative hematological profile, we found difference with respect to platelet dose, which was higher in the placebo group. We found absence of difference between EACA and placebo groups regarding hemoglobin and hematocrit parameters.
According to our data, there was no difference between the CABG without CPB and the EACA groups, indicating the beneficial effects of EACA. The favorable effects of the topical application of antifibrinolytics on patients undergoing CABG with CPB were previously documented in the literature. In 2009, a systematic review of 8 randomized-controlled studies comparing the topical use of aprotinin and tranexamic acid was published, suggesting that both agents are effective in reducing bleeding and decreasing the need for blood transfusions. Moreover, the authors described the absence of studies with EACA topically applied, which, combined with the low cost of the drug, led to its use in our study. 23
Before the surgical procedures, platelet count was higher in the EACA group. This difference is possible due to interpersonal variability of this variable. Moreover, we observed that platelet count was higher in the EACA group compared to the control group. This finding suggests that aprotinin influences platelet count. Conversely, we found no difference regarding bleeding between EACA and control groups. A previous study supports the effect of aprotinin in bleeding. The authors influence using aprotinin demonstrated a benefit on reducing bleeding in 25 patients holding coronary disease. 24 These data were supported in a randomized and double-blind investigation performed in 100 patients submitted to myocardial revascularization surgery. 25
Our findings support a previous study published by our group. 14 In 2009, our group 14 demonstrated a favorable effect of the topical application of EACA on patients undergoing CABG with CPB, reducing bleeding in approximately 30% based on the drainage volume. Furthermore, Hosam et al 26 in 2009, in a randomized study of tranexamic acid applied in the pericardial cavity after CABG with CPB, showed a significant reduction of 37% in bleeding in the first 24 hours after surgery. Nevertheless, both studies included only patients undergoing CABG with CPB.
Several meta-analysis showed similar results on mortality, stroke, myocardial lesions, atrial fibrillation, and need for transfusion of blood and blood components in comparison with patients undergoing CABG with and without CPB. 27 –30 It is noteworthy that most of these studies compared only low-risk patients, because when more severely affected patients are studied, the benefits of the operation without CPB become more evident. 31,32
A meta-analysis published by Cheng et al suggested that the coagulation disorder, fibrinolysis, and platelet dysfunction are not as intense in patients undergoing CABG without CPB. 1 –3,26 A meta-analysis published in 2009 26 showed that the use of CABG without CPB has increased over the years around the world. However, the number of studies with patients undergoing these procedures is still small, and despite the small amount of fibrinolysis caused in this surgery by the absence of CPB, the effect of the antifibrinolytic agents has not been tested enough in these patients to assume that it is ineffective.
To obtain this information, we evaluated EACA applied topically in patients undergoing CABG without CPB, and we found no significant reduction of postoperative bleeding and also regarding the need for blood transfusion or a difference in hematological values between the groups.
The literature investigated the topical effect of EACA in some situations. A previous study reported that after aprotinin topical application in the pericardium the same substance was not found in the patients’ blood. The authors hypothesized that it may suggest a reduction in the fibrinolytic state of the patients admitted for surgery with CPB. 17 Other study evaluated 300 patients submitted to heart surgery, they were divided into 3 groups placebo, aprotinin, and tranexamic acid groups. It was reported a beneficial effect in the topical application of the both antifibrinolytic agents. Tranexamic acid and aprotinine decreased the cumulative blood loss compared to the placebo group. On the other hand, it was observed no reduction in the blood and hemoderivative transfusion in the treated groups. 18 Taken together, the literature and our results support the positive effects of EACA.
There is still uncertainty with respect to the safety use of parenteral application of antifibrinolytic agents. The topical application of aprotinin in the pericardial cavity is indicated to be a better way, considering the likelihood of decreasing the adverse effects of medications, for instance, renal risk of graft acute thrombosis after myocardial revascularization surgery. In our center, we have used the routine parenteral EACA in cardiac surgery procedures. Nonetheless, based on Baric et al study, 17 we decided to evaluate the efficacy of EACA topically applied in the pericardium. Although the small number of patients investigated, our results support a positive effect of EACA topically applied in the pericardium. It possibly represents an adequate method with decrease in the collateral effects of the systemic use of antifibrinolytic agents. A likely problem of the use would be the rise of pericardial adherence, causing additional complications in future reoperation. Nevertheless, this hypothesis needs further confirmation. This hypothesis was suggested in a previous study that investigated the use of aprotinine. 21
Our study presents some points that are worth to be raised. The limitations of this study include the lack of an antifibrinolytic serum dose after 2 hours of administration and the number of patients, which actually represents the applicability of the operation without CPB in our surgical routine. Also, there was a different course of the platelet count regarding the placebo and experimental groups. In the EACA group, there was a mentionable decrease in the platelet count after the procedure, while the platelet count in the placebo group was significantly lower before surgical procedures. However, this fact was not reported regarding the other variables investigated related to bleeding. We believe that the use of topical EACA may be involved in this mechanism. Further studies are necessary to better investigate this process.
Conclusion
The topical use of EACA in patients undergoing CABG without CPB showed no difference in reducing the amount of bleeding and the need for blood transfusions.
Footnotes
Acknowledgment
This research was supported by Faculdade de Medicina do ABC.
Authors’ Note
The study was not presented orally at a professional meeting.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Faculdade de Medicina do ABC.