
Abstract
Diabetes mellitus (DM) increases the risk of adverse outcomes after coronary revascularization. Controversy persists regarding the optimal revascularization strategy for diabetic patients with multivessel coronary artery disease (MVD).
Aim
The aim of this study was to assess the outcomes of drug-eluting stent (DES) insertion in DM and non-DM patients with complex coronary artery disease (CAD) after risk stratification by the percutaneous coronary intervention with taxus and cardiac surgery (SYNTAX) score.
Methods and Results
We performed multivessel percutaneous coronary intervention (PCI) for 601 lesions in 243 DM patients and 1,029 lesions in 401 non-DM patients. All included patients had MVD and one or more lesions of type B2/C. The two-year outcomes and event rates were estimated in the DM and non-DM patients using Kaplan–Meier analyses. The baseline SYNTAX score was ≤22 in 84.8% vs. 84%, P = 0.804, and 23-32 in 15.2% vs. 16%, P = 0.804, of the DM and non-DM patients, respectively. The number of diseased segments treated (2.57 ± 0.75 vs. 2.47 ± 0.72; P = 0.066) and stents implanted per patient (2.41 ± 0.63 vs. 2.32 ± 0.54; P = 0.134) were similar in both groups. After a mean follow-up of 642 ± 175 days, there were no differences in the major adverse cardiac and cerebrovascular events (MACCE; 26.7% vs. 20.9%; P = 0.091), composite end point of all-cause death/myocardial infarction (MI)/stroke (12.3% vs. 9%; P = 0.172), individual MACCE components of death (3.7% vs. 3.2%; P = 0.754), MI (6.6% vs. 4%; P = 0.142), and absence of stroke in the DM and non-DM patients. An increased need for repeat revascularization was observed in DM patients (18.5% vs. 10.2%; P = 0.003). In the multivariate analysis, DM was an independent predictor of repeat revascularization (hazard ratio: 1.818; 95% confidence interval: 1.162-2.843; P = 0.009).
Conclusions
DES implantation provides favorable early and mid-term results in both DM and non-DM patients undergoing PCI for complex lesions. After a mean follow-up of two years, DM and non-DM patients with complex CAD treated by PCI using new-generation DES showed no differences with regard to MACCE and other secondary end points. However, higher rates of ischemia-driven repeat revascularization were observed in DM patients.
Introduction
In the last several decades, the global prevalence of diabetes mellitus (DM) has continuously increased.1,2 Coronary artery disease (CAD) is a major cause of morbidity and mortality in diabetic patients, and more than 80% of DM deaths occur in low- and middle-income countries.3,4 Compared to nondiabetic patients, patients with DM have a greater extent of coronary atherosclerosis, higher plaque burden, 5 and are more prone to develop multivessel CAD.6,7
Coronary artery revascularization in patients with DM poses a challenge because diabetes has been found to increase the risk of adverse outcomes after coronary artery bypass grafting (CABG) or percutaneous coronary intervention (PCI).8–10 The current guidelines recommend CABG over PCI in patients with DM and multivessel coronary artery disease (MVD) CAD.11,12 The FREEDOM trial demonstrated that CABG was superior to multivessel PCI with the use of first-generation drug-eluting stents (DESs) in patients with DM and MVD. CABG significantly reduced the rates of death and myocardial infarction (MI) but was associated with a higher rate of nonfatal stroke. 13 Although CABG remains superior to PCI among patients with DM and MVD, particularly for patients with higher angiographic disease complexity, the gap between CABG and PCI has narrowed over time. 14 Future trial should be performed to compare CABG and the new PCI technologies based on the currently available newer generation stents specifically in diabetic patients to define the optimal management strategy.
The percutaneous coronary intervention with taxus and cardiac surgery (SYNTAX) score is an angiographic scoring tool used for systematically quantifying the severity and assessing the characteristics of individual coronary lesions. 15 This score is used worldwide to predict the long-term outcomes in patients with CAD undergoing elective PCI or CABG surgery. The SYNTAX score (SS) was shown to be an independent predictor of long-term adverse outcomes in patients with multivessel disease undergoing PCI. 16
Aim
The aim of this study was to assess the outcomes of DES implantation in DM and non-DM patients with complex CAD after risk stratification by the SS.
Methods
Study Population
From June 2012 to June 2013, a total of 644 consecutive patients (243 DM patients with 601 treated lesions and 401 non-DM patients with 1,029 treated lesions) were included. All patients underwent early PCI during their admission at Alexandria Main University Hospital and the International Cardiac Center (ICC) at Alexandria.
Inclusion Criteria
All included patients had MVD and ≥1 lesion with an American College of Cardiology (ACC) and American Heart Association (AHA) classification type B2/C 17 with clinical indications for revascularization who had not previously undergone angioplasty or coronary surgery. Multivessel PCI was systematically offered to the patients as an alternative to surgery whenever complete revascularization with a finite number of stents was judged to be feasible.
Exclusion Criteria
Patients were excluded based on the following criteria:
Patients with multivessel disease who were candidates for CABG (SS ≥ 33),
Patients with left main disease,
Patients with previous PCI,
Patients with previous CABG, and
Patients with a life-threatening noncardiac illness.
Procedural Data
All patients who underwent PCI received at least 300 mg of aspirin and a 600-mg loading dose of clopidogrel. Heparin was administered throughout the procedure to maintain an activated clotting time of ≥250 seconds. The DES selection and use of glycoprotein IIb/IIIa inhibitors were left to the discretion of the surgeon. After the procedure, all patients received 100 mg/day of aspirin indefinitely, as well as 150 mg of clopidogrel for seven days, followed by 75 mg/day of clopidogrel for at least 12 months. The use of standard postintervention care was recommended.
Angiographic Analysis
Angiographic imaging was performed in two orthogonal views after the intracoronary injection of nitrates. Each lesion was measured before and after stenting on nonoptically magnified cineangiographic frames showing the lesion in its highest grade, using the guiding catheter as a reference. Measurements of the diameter of the guiding catheter, the minimal vessel lumen diameter, and the percent stenosis before and after stenting were performed by automatic contour edge detection; intravascular ultrasound imaging was not routinely used. The patients' angiographic images were reviewed, and the SS was calculated using a web-based calculator (www.syntaxscore.com) by the same trained physician, who was blinded to the clinical outcomes of the patients.
Patient follow-up
Clinical follow-up was performed for all patients at 1, 3, 6, 9, and 12 months and every 3 months thereafter either during outpatient department visits or by direct telephone calls to patients. All the patients were contacted for follow-up regarding the presence of angina, adverse events (death, nonfatal MI, and need for repeat percutaneous intervention in the target lesion), and CABG. For all patients who reported cardiac symptoms, a clinical evaluation was performed. Noninvasive testing for myocardial ischemia was performed for all patients unless contraindicated. Follow-up coronary angiography was performed for all patients with a recurrence of angina or positive findings detected by noninvasive testing. All data collected were stored in a regularly updated computer database.
Study outcomes and Definitions
The primary outcome of this study was the major adverse cardiac and cerebrovascular events (MACCE) [a composite of the cardiac death, MI, or iischemia driven target lesion revascularization (ID-TLR)], death (cardiac and noncardiac), nonfatal MI, ID-TLR, stent thrombosis, and stroke. Periprocedural MI was defined as an increase of biomarkers (creatine kinase isoenzyme MB [CK-MB] or troponin) greater than three times the upper limit of normal. 18 Q-wave MI was defined as an elevation of CK-MB ≥2 times the upper normal value in the presence of new pathologic Q-waves (>0.4 seconds) in ≥2 contiguous leads of the electrocardiogram. Non-Q-wave MI was defined as typical ischemic chest pain and/or ST-segment and/or T-wave abnormalities with a CK-MB increase ≥2 times the reference values without any new pathologic Q-waves. TLR was defined as clinically driven revascularization of the index lesion. Stent thrombosis was defined as definite or probable stent thrombosis according to the Academic Research Consortium definitions. 19 DM was defined as either a previous diagnosis of diabetes treated with diet, oral agents, peptide analogs, and insulin or a new diagnosis during index hospitalization.
Statistical Analysis
Qualitative data were described using numbers and percentages and were compared using chi-squared test. Quantitative data were described using means and standard deviations as measures of central tendencies and dispersion, respectively, for normally distributed data and were compared using Student's t-test, while abnormally distributed data were expressed using medians, minimums, and maximums and were compared using Mann–Whitney test. Cumulative event rates were estimated using time-to-event methods, survival functions were compared using log-rank test, and Kaplan–Meier survival curve was used to illustrate the survival functions. Cox proportional hazards multivariate analysis was performed to adjust for baseline characteristic differences that remained despite the propensity matching. All statistical analyses were performed using the SPSS software (version 20.0; SPSS Inc.). A value of P < 0.05 was considered to be statistically significant.
Sample size and power calculation
Using NCSS 2004 and PASS 2000 software (power analysis and sample size), group sample sizes of 243 and 401 (total, 644) achieve 82% power to detect a difference of 10% of the proportion surviving at two years (not developing any MACE event) between the diabetic and nondiabetic groups (0.6 and 0.7, respectively) using log-rank test and using a significance level of 0.05.
Ethics Statement
This study was reviewed and approved by the review board of the Faculty of Medicine, Alexandria University. The research complied with the principles of the Declaration of Helsinki. All participants were requested to provide written informed consent regarding the procedure according to the study protocol.
Results
We performed multivessel PCI in 243 DM patients with 601 treated lesions and 401 non-DM patients with 1,029 treated lesions using second-generation DES (everolimus-eluting stents [EES] or zotarolimus-eluting stents). All included patients had MVD and ≥1 lesion of type B2/C. Baseline clinical characteristics of the study groups are shown in (Table 1). The two-year outcomes and event rates were estimated in both groups of patients using Kaplan–Meier analyses.
Baseline clinical characteristics.
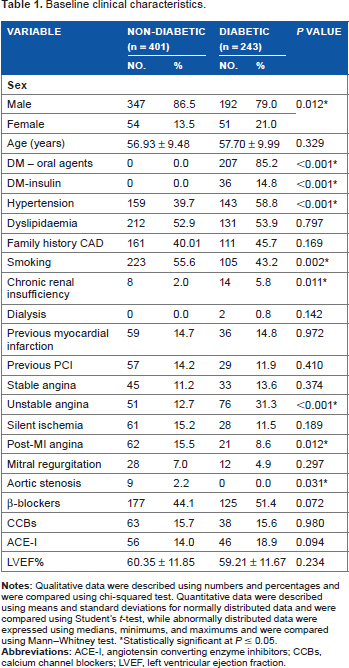
Statistically significant at P ≤ 0.05.
There was no statistically significant difference between two groups as regards the angiographic characteristics, the baseline SS (Table 2), the number of diseased segments treated (2.57 ± 0.75 vs. 2.47 ± 0.72; P = 0.066), and stents implanted per patient (2.41 ± 0.63 vs. 2.32 ± 0.54; P = 0.134).
Baseline angiographic characteristics.

Statistically significant at P ≤ 0.05.
Inhospital Outcome
There was no significant difference in the inhospital MACCE between the two groups (2% vs. 2.1%; P = 1.000), as shown in Table 3.
Inhospital and mid-term outcomes according to the diabetic status.

Statistically significant at P ≤ 0.05.
Mid-term outcome
After a mean follow-up of 642 ± 175 days, there were no differences in the MACCE (26.7% vs. 20.9%; P = 0.091), composite end point of all-cause death/MI/stroke (12.3% vs. 9%; P = 0.172), individual MACCE components of death (3.7% vs. 3.2%; P = 0.754), MI (6.6% vs. 4%; P = 0.142), and absence of stroke in the DM and non-DM patients. A greater need for repeat revascularization was observed in DM patients (18.5% vs. 10.2%; P = 0.003), as shown in Table 3. The Kaplan–Meier survival curves based on the MACCE rates, death/MI/stroke and repeat revascularization in diabetic and nondiabetic patients are shown in Figures 1–3.

The Kaplan-Meier survival curves based on the MACCE rates in diabetic and nondiabetic patients.

The Kaplan–Meier survival curves for the death/stroke/MI rates in diabetic and nondiabetic patients.

The Kaplan–Meier survival curves for the repeat revascularization rates in diabetic and nondiabetic patients.
In the multivariate analysis, DM was identified as the only independent predictor of repeat revascularization even after adjustment of baseline characteristic differences, which was significantly different between the two groups by univariate analysis (hazard ratio: 1.818; 95% confidence interval: 1.162-2.843; P = 0.009), as shown in Table 4.
Cox proportional hazard multivariate analysis for repeat revascularization.

Discussion
DM is becoming one of the most important health problems worldwide. Approximately 60% of all patients who undergo coronary artery revascularization via CABG or PCI have MVD that is amenable to treatment by one of these procedures. The long-term success of multivessel PCI in diabetic patients is principally limited by the need for repeat revascularizations, which are performed not only for restenosis but also for disease progression. This study examined the outcomes of DES implantation in DM and non-DM patients with complex CAD after risk stratification by the SS. The baseline SS was ≤22 in 84.8% DM patients vs. 84% in non-DM patients, while 15.2% vs. 16% of the DM and non-DM patients, respectively, had an intermediate SS (23-32). After two years of follow-up, there were no differences in the rates of MACCE (26.7% vs. 20.9%), composite end point of all-cause death/MI/stroke (12.3% vs. 9%), individual MACCE components of death (3.7% vs. 3.2%), MI (6.6% vs. 4%), and absence of stroke in the DM and non-DM patients. The present study, representing a patient population with a broad spectrum of clinical presentations varying from stable angina pectoris to ST-segment elevation MI, demonstrates that DM was associated with a higher need for repeat revascularization in DM patients (18.5% vs. 10.2%; P = 0.003), even with the use of DES.
The selection of an appropriate revascularization strategy for an individual patient with MVD is complex. The current guidelines recommend that CABG should be preferred to PCI in patients with MVD and DM.11,12 The FREEDOM trial demonstrated that in diabetic patients with MVD, CABG was superior to PCI when the first-generation DESs were used. CABG significantly reduced the rates of death and MI but was associated with a higher rate of stroke. Subgroup analyses of DM patients included in the FREEDOM trial stratified by insulin treatment have been reported by Dangas et al. The overall five-year event rate of death/stroke/MI was significantly higher in patients treated with insulin than in those not treated with insulin (28.7% vs. 19.5%; P < 0.001). 20 Before the results of the FREEDOM trial are applied to all DM patients in real-world practice, it should be considered that only 10% of the screened patients met the inclusion criteria, with only two-thirds of these finally providing informed consent for participation. In addition, the PCI group comprised a high-risk population: 82% had three-vessel disease, the mean number of lesions/patient was 5.6 ± 2.2, and 34% of the patients were insulin-treated DM patients. In addition, 65% of the PCI patients had an intermediate or high SS. First-generation DESs were used in 94% of the included patients.
Data based on the conclusions from the CARDia trial 21 and the five-year results of the SYNTAX trial indicated significantly higher rates of MACCE and repeat revascularization in patients with DM treated with PCI compared with those treated with CABG. 16 The SYNTAX trial concluded that PCI is a potential treatment option for patients with less complex lesions, but that CABG should be the revascularization option of choice for patients with more complex anatomical disease, especially in DM patients. Extrapolating the findings of the previous trials to current clinical practice is not really possible because the use of the newer generation DES now available may lead to a better outcome in DM patients. The combination of thin struts and the advanced polymer technology of the newer generation DES has been shown to contribute to improved early endothelialization, lower inflammation, and lower stent thrombosis rates.22,23 A recent study conducted by Pendyala et al showed better safety and efficacy of EES compared with the first-generation DES when used in diabetic patients undergoing multivessel PCI. In DM patients undergoing native multivessel PCI, the use of EES was associated with superior one-year safety compared with the use of first-generation DES. This benefit was mainly driven by decreased rates of all-cause mortality and cardiac mortality in the EES group. 24
In the present study, multivessel PCI was performed in 243 DM patients with 601 treated lesions and 401 non-DM patients with 1,029 treated lesions. The differences between the study protocol and the previous trials were: (1) all included patients had MVD and ≥1 lesion of type B2/C treated with ≥2 stents in ≥2 different coronary territories (excluding the left main), (2) the majority of the study population (≈84%) had a low SS (≤22) and the maximum SS was ≤27, (3) a small number of the study participants were insulin-treated diabetic patients (14.8%), (4) the reference vessel diameter of all treated lesions was ≥2.75 mm, and (5) the treatments involved the use of new-generation DESs. The two-year outcomes showed a higher need for repeat revascularization in DM patients, but no significant differences with regard to the MACCE, composite end point of all-cause death/MI/stroke, individual MACCE components of death, MI, and absence of stroke. These results with relatively better clinical outcomes in diabetic patients could be explained by the differences in the inclusion criteria, patient selection, and use of newer generation DES.
In agreement with our study, a large analysis of 18 pooled randomized trials examining DES outcomes according to the presence of DM conducted by Kedhi et al. 25 demonstrated that DM remains an independent predictor of one-year repeat revascularization and adverse events (cardiac death or MI) in the DES era. There were increased rates of TLR and target vessel revasularization (TVR) in patients with DM versus those without DM with complex lesions (ACC/AHA class B2/C), but not in patients with simpler lesions (A/B1). However, there was no significant relationship between the presence of diabetes, lesion type, and cardiac death or MI. The main finding of this study was that diabetic patients had favorable intermediate-term outcomes after the treatment of noncomplex lesions with DES. In addition, the two-year results of the international global RESOLUTE program evaluating the outcomes of zotarolimus-eluting stents in 1,535 patients with DM compared with all 3,595 patients without diabetes showed an equivalent cumulative incidence of target lesion failure in patients with noninsulin-treated DM versus patients without DM. The patients with insulin-treated diabetes demonstrated a significantly higher target lesion failure rate. It should be noted that the high-risk subsets from the RESOLUTE All Comers and the observational RESOLUTE international study were excluded from the primary analysis of that study. 26 Moreover, some of the registry data have shown that the clinical events were similar in diabetic patients undergoing CABG surgery or PCI.27,28 Advances in PCI technology, including newer generation DES and bioabsorbable stents, may further reduce the risk of target lesion failure, the need for repeat revascularization, and the long-term risk of stent thrombosis. 29 Additionally, functional assessment with fractional flow reserve will help identify hemodynamically important and significant lesions that would benefit most from revascularization. Using such a strategy would allow for the identification of ischemia-producing lesions and may have important prognostic utility in reclassifying patients with MVD into functional one- or two-vessel CAD.30,31
The findings of the present study demonstrated favorable mid-term outcomes in selected diabetic patients after treatment of complex lesions with the new-generation DES, although there was a greater need for repeat revascularization in the diabetic patients. The optimal revascularization strategy in diabetic patients with MVD must be determined after considering the different anatomical, clinical, and technical factors for each particular patient. All of these factors should be assessed by the heart team in order to make a decision for an individual patient in real-world practice. Future clinical trials should compare CABG and the new PCI technologies based on the currently available newer generation stents, specifically in diabetic patients, in order to define the optimal management strategy.
Conclusions
The currently used newer generation DESs are associated with favorable early and mid-term results in both DM and non-DM patients undergoing PCI for complex lesions. After a mean follow-up of two years, DM and non-DM patients with complex CAD treated by PCI using the new-generation DES showed no differences with regard to MACCE and other secondary end points. However, higher rates of ischemia-driven repeat revascularization were observed in DM patients. For patients with DM and complex CAD, the decision to proceed to coronary revascularization must carefully consider and incorporate all of the clinical and angiographic characteristics and the circumstances of each individual patient, and such a decision should be made only after discussion in a multidisciplinary heart team.
Study Limitations
This study was a prospective single-center study and therefore lacks randomization and intention to treat data. As an observational study, it is subject to selection bias. The reason for choosing multivessel PCI in preference to CABG was not evaluated in the present study. The study sample was relatively small, and the short duration of follow-up in this study should be considered a limitation of the present analysis. Therefore, our results did not provide data on the outcome of multivessel PCI in DM versus non-DM patients in the longer perspective. Despite these limitations, this study provides insight into a large series of consecutive diabetic patients treated with native multivessel PCI and their midterm outcomes.
Author Contributions
Conceived and designed the experiments: ML. Analyzed the data: ML. Wrote the first draft of the manuscript: ML, MAS. Contributed to the writing of the manuscript: ML. Agree with manuscript results and conclusions: ML, MAS, MS. Jointly developed the structure and arguments for the paper: ML, MAS, MS. Made critical revisions and approved final version: ML, MAS, MS. All authors reviewed and approved of the final manuscript.