
Abstract
Background
Few studies evaluated left ventricular (LV) involvement in arrhythmogenic right ventricular dysplasia/cardiomyopathy (ARVD/C). The aim of this study is to determine the frequency, clinical presentation, and pattern of LV involvement in ARVD/C (LV-ARVD/C).
Methods
We retrospectively evaluated the cardiac magnetic resonance (CMR) in 202 patients referred between 2008 and 2012 to our institution, and we determined the presence or the absence of CMR criteria in the revised task force criteria 2010 for the diagnosis of ARVD/C. A total of 21 patients were diagnosed with ARVD/C according to the revised task force criteria 2010. All included patients had no previous history of myocarditis, acute coronary syndrome, or any other cardiac disease that could interfere with the interpretations of structural abnormalities. The LV involvement in ARVD/C was defined by the presence of one or more of the following criteria: LV end-diastolic volume (LVEDV; >95 mL/m2), LV ejection fraction (LVEF; <55%), LV late enhancement of gadolinium (LVLE) in a non-ischemic pattern, and LV wall motion abnormalities (WMAs). In the follow-up for the occurrence of cardiac death, ventricular tachycardia (VT) was obtained at a mean of 31 ± 20.6 months.
Results
A total of 21 patients had ARVD/C. The median age was 48 (33-63) years. In all, 11 patients (52.4%) had LV-ARVD/C. The demographic characteristics of patients with or without LV were similar. There was a higher frequency of left bundle-branch block (LBBB) VT morphology in ARVD/C (P = 0.04). In CMR, regional WMAs of right ventricle (RV) and RV ejection fraction (RVEF; <45%) were strongly correlated with LV-WMAs (r = 0.72, P = 0.02, r = 0.75, P = 0.02, respectively). RV late enhancement of gadolinium (RVLE) was associated with LV-WMs and LVLE (r = 0.7, P = 0.03; r = 0.8, P = 0.006). LVLE was associated with LV-WMAs, LVEF, and LVEDV (r = 0.9, P = 0.001; r = 0.8, P = 0.001; r = 0.8, P = 0.01).
Conclusion
LV involvement in ARVD/C is common and frequently associated with moderate to severe right ventricular (RV) abnormalities. The impact of LV involvement in ARVD/C on the prognosis needs further investigations.
Keywords
Introduction
Arrhythmogenic right ventricular dysplasia/cardiomyopathy (ARVD/C) is a rare disease. The estimated prevalence of the disease in the general population ranges from 1 in 1000 to 1 in 5000. 1 ARVD/C has been originally described as an inherited cardiomyopathy characterized by structural and functional abnormalities because of a progressive replacement of right ventricular (RV) myocardium by fibro-fatty tissues. 2 ARVD/C predisposes patients to sudden death and ventricular arrhythmia, typically among young subjects and athletes, 3 and leads to progressive heart failure.1,2,4
Molecular genetic studies provide evidence that fibro-fatty replacement is caused by mutation-related desmosomal changes.1,5,6 The diagnosis of ARVD/C is still challenging and is currently based on a multi-disciplinary evaluation of the patient, as defined by the task force of 1994 7 and, more recently, the proposed modification of task force of 2010 to improve the diagnosis and management of ARVD/C 8 with increased sensitivity and without loss of specificity.8,9
A few studies reported left ventricular (LV) involvement in ARVD/C (LV-ARVD/C). In those studies, the diagnosis of LV-ARVD/C was based on echocardiography, myocardial scintigraphy, magnetic resonance imaging (MRI), and autopsy studies.10–13 The place of the LV involvement in the natural history of the disease remains to be established.
There are very few cardiac magnetic resonance (CMR) studies evaluating the LV involvement in ARVD/C.12,14,15 The aim of the present study was to report the frequency, the severity, and the prognosis of LV involvement using CMR in patients diagnosed with ARVD/C.
Materials and Methods
Patients and Study Design
We retrospectively evaluated the CMR in 202 patients referred between 2008 and 2012 to our institution, and we determined the presence or the absence of CMR criteria in the revised task force criteria 2010 for the diagnosis of ARVD/C. The keywords used in order to sort the request of all CMR referred to our institution were ARVD/C, RV dysplasia, RV akinesia, RV dyskinesia, RV hypokinesia, RV dilatation, sudden death, cardiac arrest, ventricular tachycardia (VT), and premature ventricular contractions (PVCs). Twenty one patients were diagnosed with ARVD/C according to the revised task force criteria 2010. The clinical history and previous personal and family history were recorded for the 21 ARVD/C patients. All included patients had no previous history of myocarditis, acute coronary syndrome, or any other cardiac disease that could interfere with the interpretations of structural abnormalities. This research was exempt from the requirement of obtaining ethics committee approval, because of the retrospective nature of the research. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Electrocardiogram (ECG) analysis
ECGs were analyzed according to the revised task force criteria 2010 8 , looking for epsilon waves and inverted T waves in right precordial leads (V1, V2, and V3) or beyond in individuals >14 years of age in the absence of complete right bundle-branch block (RBBB) QRS ≥120 milliseconds, in leads V1 and V2 in individuals >14 years of age in the absence of complete RBBB, in leads V4, V5, or V6, or in leads V1, V2, V3, and V4 in individuals >14 years of age in the presence of complete RBBB. 7 Ventricular arrhythmia was recorded. Non-sustained ventricular tachycardia (NSVT) (≥3 consecutive beats at ≥120 bpm with a duration <30 seconds) sustained VT (>30 seconds duration). 12 PVCs of RBBB and left bundle-branch block (LBBB) morphologies were presumed of LV and RV origins, respectively. Biventricular arrhythmia was defined by the presence of PVCs of both RBBB and LBBB morphologies.
CMR acquisitions
Images were performed on a 1.5 Tesla MR system (Aera XQ Siemens) using a cardiac phased-array coil and ECG gating. Steady-state free precession (SSFP) sequences were used for the evaluation of left and right ventricles (RVs).
RV parameters
Cine images were acquired in stacked axial datasets. The workstation calculated end-systolic and end-diastolic RV volumes using the method of summation of discs. The RV ejection fraction (RVEF) was calculated. The RV was divided into three levels in the short-axis plane: basal, mid, and apical. The infundibulum, anterior, inferior, and lateral walls were assessed.
Left ventricle (LV) parameters
Cine images were acquired in the short axis. The workstation calculated end-systolic and end-diastolic LV volumes using the method of summation of discs. The LV ejection fraction (LVEF) was calculated.
The LV late enhancement of gadolinium (LVLE) and RV late enhancement of gadolinium (RVLE) were assessed using phase-sensitive inversion recuperation (PSIR) CMR sequences for 10 minutes following injection of gadolinium chelates DOTA-Gd (15-20 mL).
RV involvement
The study of the RV involvement is based on the revised task force criteria 2010 in CMR and echocardiography.8,9 CMR criteria of RV involvements were regional RV akinesia or dyskinesia or dyssynchronous RV contraction and one of the following: ratio of RV end-diastolic volume to body size area (BSA) ≥100 mL/m2 (male) or ≥90 mL/m2 (female) or RVEF ≤45%.
LV involvement
In this study, LV involvement was considered present if one or more of the following CMR criteria were present, as determined by the first CMR study evaluating LV involvement in ARVD/C 13 : LVEF <55%, LVLE in a non-ischemic pattern, LV dilatation with LV end-diastolic volume (LVEDV) >95 mL/m2 for male and 90 mL/m2 for women, and/or LV wall motion abnormalities (WMAs).
Clinical Endpoints
Cardiac death was defined as any death with demonstrable cardiac cause or any death that was not clearly attributable to a non-cardiac cause: the occurrence of syncope, VT, ventricular fibrillation (VF), implantable cardiovertor defibrillator (ICD), hospitalization for heart failure, or cardiac transplantation. The follow-up was obtained at a mean of 31 ± 20.6 months.
Statistical Analysis
Continuous variables were analyzed for normal distribution with the Shapiro–Wilk test. Continuous variables were expressed as median (25 and 75 interquartile ranges), and categorical variables were expressed as frequencies and percentages. Patients were classified into two groups: patients without LV involvement (ARVD/C) and patients with LV involvement (LV-ARVD/C). Continuous variables were compared between the two subgroups by non-parametric Mann–Whitney U test as the distribution was not normal. Fisher's exact tests have been used for comparison of categorical variables. Relationship between two continuous variables was assessed with Pearson's correlation coefficient; Spearman's rank correlation was used when either or both variables were ordinal. A P value <0.05 was considered statistically significant. Statistical analysis was performed with SPSS version 19.0 software.
Results
Demographics, ECG, and arrhythmic findings
A total of 21 patients had ARVD/C. Major and minor criteria, modified task force criteria 2010, met by each patient are summarized in Table 1. The median age of patients was 48 (33-63) years. In all, 11 patients (52%) had LV involvement (LV-ARVD/C) (Table 2). In ARVD/C, it was more common, but there was no difference in male/female ratio between ARVD/C and LV-ARVD/C. In all, 12 of the 21 patients (57%) were symptomatic; the most frequent symptom was palpitation. A total of 11 patients (52%) had ECG abnormalities with inverted T waves and 10 (48%) fulfilled the major revised task force criteria for repolarization abnormalities. In all, 12 (57%) patients presented NSVT or VT. The most frequent VT morphology was LBBB morphology (58.3%) originating from the RV. There was significant difference in demographic characteristics (age <40 years, sex, personal previous history, clinical presentation, sport and family history) between ARVD/C and LV-ARVD/C. Baseline characteristics are summarized in Table 3. Three ARVD/C patients had lateral repolarization abnormalities. Only two LV-ARVD/C patients had such repolarization troubles, one in inferior leads and the other in apicolateral leads. LBBB-VT morphology was more frequent in ARVD/C compared to LV-ARVD/C (6 vs 1, P = 0.04). LV-ARVD/C was negatively correlated with the LBBB-VT morphology (r = −0.539, P = 0.012).
ARVD/C modified task force criteria 2010 met by the population study.

ARVD/C modified task force criteria 2010 met by LV-ARVD/C population.

Baseline clinical characteristics.

Disease Patterns
RV abnormalities
A total of 15 patients (71%) had severe RV dilatation and 2 (10%) had mild RV dilatation. In all, 13 patients (62%) had RVEF alteration ≤45%, 11 patients (52%) had severe RVEF alteration ≤40%, and 2 patients (10%) had mild RVEF alteration between 40 and 45%. One patient (5%) had an infundibulum aneurysm. A total of 10 patients (48%) had RV late gadolinium enhancement. The distribution of RV-WMAs was quite homogeneous in ARVD/C and LV-ARVD/C, except for the RV infundibulum. There was higher RV infundibulum motion abnormalities in ARVD/C group compared to LV-ARCD/C group (P = 0.007).
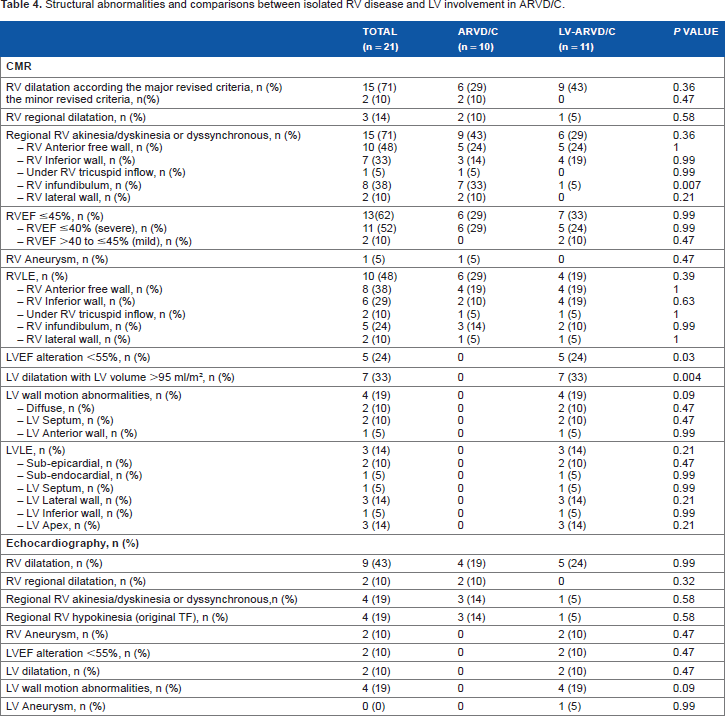
Using echocardiography, RV dilatation was detected in nine patients (43%) and segmental dilatation in two patients (10%). Only two patients (10%) with localized RV aneurysms were found, while regional RV hypokinesia was found in four patients (19%) and regional RV akinesia, dyskinesia, or dyssynchronous RV contraction was recorded in four patients (19%). Structural abnormalities are summarized in Table 4.
Structural abnormalities and comparisons between isolated RV disease and LV involvement in ARVD/C.
LV involvement
Seven patients (33%) presented LV dilatation with LV volume >95 mL/m2. Five patients (24%) had LVEF alteration <55% (the LVEF of those five patients were 37%, 40%, 50%, 53%, and 53%). Four patients (19%) had LV WMAs. Three (14%) patients had LVLE (Table 4). Subepicardial LVLE of the lateral and inferior walls of the LV of two LV-ARVD/C patients is shown in Figures 1 and 2. All LV-ARVD/C patients had no previous history of myocarditis or coronary artery disease.

(
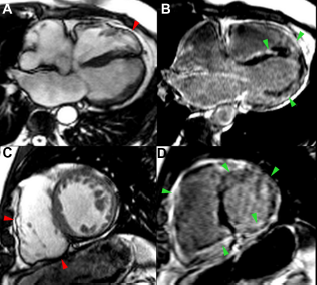
(
Comparison of Disease Patterns
CMR data
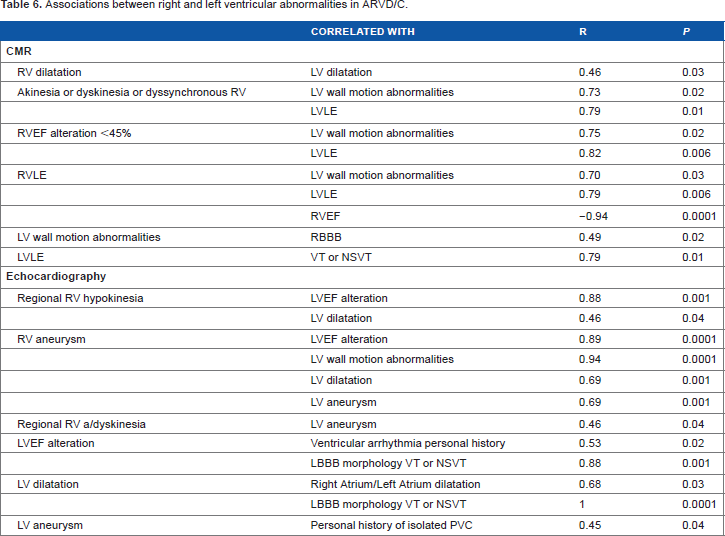
RVEF was similar in ARVD/C and LV-ARVD/C (45% [32-51], 47% [30-54], P = 0.84). Although there was a trend for a larger RV in LV-ARVD/C as compared to ARVD/C, this difference did not reach statistical significance (107 mL/m2 [89-114], 120 mL/m2 [115-130], P = 0.09) (Table 5). The RV-WMAs, RVLE, and RVEF (<45%) were strongly associated with LV-WMAs (r = 0.73, P = 0.02; r = 0.7, P = 0.03; r = 0.75, P = 0.02, respectively) and with LVLE (r = 0.8, P = 0.01; r = 0.8, P = 0.006; r = −0.82, P = 0.006, respectively). LV dilatation was associated with RV dilatation (r = 0.46, P = 0.036). LVLE was strongly associated with LV-WMAs, LVEF alteration, and LVEDV (r = 0.9, P = 0.001; r = 0.8, P = 0.001; r = 0.8, P = 0.01) (Table 6).
Left and right ventricular functions in ARVD/C.

Associations between right and left ventricular abnormalities in ARVD/C.
Echocardiography Data
Regional RV hypokinesia and aneurysm were strongly associated with LVEF ≤50% (r = 0.88, P = 0.001; r = 0.9, P = 0.0001, respectively) and with LV dilatation (r = 0.5, P = 0.04; r = 0.7, P = 0.001, respectively). RV aneurysm was strongly correlated with LV-WMAs (r = 0.9, P = 0.0001) and LV aneurysm (r = 0.7, P = 0.001). Regional RV dyskinesia was correlated with LV aneurysm (r = 0.5, P = 0.04). The LV and RV dilatation, RV aneurysm, and RV regional dilatation were strongly associated with LBBB-VT morphology or NSVT (r = 1, P = 0.000; r = 1, P = 0.000; r = 1, P = 0.000; r = 0.5, P = 0.04, respectively) (Table 6).
Disease Prognosis
The follow-up was obtained at a mean of 31 ± 20.6 months. Four patients (19%) had ICD: one (5%) in secondary prevention after a sudden death, two (10%) in secondary prevention for symptomatic VT, and 1 (5%) in primary prevention for the purpose of resynchronization. Out of the 12 patients who had ventricular arrhythmia (VT/NSVT), 10 patients (83.3%) were treated with beta-blockers. One patient (5%) had severe VT one month after the diagnosis, and one patient (5%) had VT 10 months after the diagnosis and an electrical storm four years after. No sudden death was recorded. There was no statistical difference between ARVD/C and LV-ARVD/C regarding cardiac events (Table 7).
Cardiac events at follow-up.

Discussion
The present study showed that LV involvement as assessed by CMR is frequent in ARVD/C. Although the LV involvement in ARVD/C was reported, almost all studies focused on the RV and the LV were often misevaluated. Only few studies have been founded in the literature that assessed the LV involvement by CMR.12,14,15 The prevalence of LV involvement in ARVD/C was variable from 16% to 76% according to the technique used for the evaluation of left ventricle.16,17 In line with the literature, our study showed that 52% of ARVD/C patients had LV involvement evaluated by CMR. In contrast to a previous study reporting 30% of LVLE, 18 our study showed 14% of LVLE. Peters and Reil reported a normal LVEF, but 40% of their 60 ARVD/C patients had LV WMAs. 19 In contrast, our study showed that 24% of ARVD/C patients had LVEF <55% but had a lower frequency of LV WMAs. In an autopsy study, the most common location of LV involvement was the posterolateral wall in a subepicardial distribution. 11 In accordance, the present study showed that lateral and apical walls were the most common locations of LV involvement in a subepicardial distribution. These data were in line with previous CMR studies.12,15
In the present study, there was no difference in clinical presentation in patients with and without LV involvement in ARVD/C, which is in line with a previous study. 13 There was no increase in the frequency of VT with RBBB morphology in LV-ARVD/C. Furthermore, the frequency of VT with LBBB morphology was higher in LV-ARVD/C. These data could suggest that the main origin of ventricular arrhythmia remains the RV, which could be related with the thinnest RV wall. The most frequent ECG repolarization abnormalities in ARVD/C with LV involvement were inverted T waves in the inferior and lateral leads. 13 In our study, although there were few ECG lateral and inferior repolarization troubles, 18% of LV-ARVD/C had inferior and lateral repolarization vs 30% in ARVD/C.
In the first reports, LV involvement in ARVD/C was frequently considered as a late manifestation of an advanced disease.4,20 Later, after the first CMR study evaluating the pattern of ARVD/C and LV involvement, LV abnormalities were found to be associated with preserved RV function in 40% of ARVD/C. 12 In the present study, the degree of RV impairment was similar in patients with isolated RV and those with LV involvement in ARVD/C. These data suggest that it is not necessary to have a severe RV impairment to imply a LV involvement. The present and previous studies showed various clinical pathological forms with only RV involvement or both RV and LV involvements, and even isolated LV involvement.15,21
The natural course of ARVD/C is still not fully elucidated. There are few data evaluating long-term prognosis of ARVD/C. Aneq et al., followed up ARVD/C patients up to 10 years. They reported that LV involvement might occur early in the disease. 22 Another study with 8.5 years follow-up reported a high rate of recurrent malignant ventricular arrhythmia in initially symptomatic patients. 23 The occurrences of life-threatening ventricular arrhythmia and heart failure are the main components of the prognosis. 24 However, early and clustered recurrence of rapid VT/VF in patients who had ICD was common, whereas late recurrence of rapid VT/VF is very rare. Six years of follow-up studies showed a good survival rate with a cardiac death rate of 8% at long-term follow-up.25,26 In the present study, the population study was small to evaluate the impact of LV in ARVD/C on the long-term prognosis. In the present study, no death and no terminal heart failure were recorded. Two initially symptomatic and high-risk patients (10%) had recurrences of VT. The only one, who had ICD, received appropriate ICD therapy. In those patients, a short delay between the diagnosis and the recurrence of ventricular arrhythmia (1 and 10 months) was reported. Furthermore, we noted CMR structural RV and LV evolutions with worsening RV dilatation, WMAs, and LVLE apparition, in a delay of 2-3 years signing a progressive disease as described in the literature.2,24 Larger studies with longer follow-up are needed to evaluate the impact of LV involvement in ARVD/C on prognosis.
Clinical Implication
The main aim of clinicians is to access the disease at an early stage, in order to propose an appropriate care and a closer follow-up. Indeed, the first diagnostic criteria were proposed by McKenna et al. 7 The revision in the diagnostic criteria of ARVD/C has recently been proposed in 2010 by Marcus et al. 8 ; these revised criteria improved the diagnostic specificity and sensitivity.8,9,27,28 These revised criteria included RV CMR criteria, but no LV involvement criteria were proposed, as LV involvement in ARVD/C is frequent without specific clinical presentation predicting them. Our findings support the emerging evidence in favor of the need for a contemporaneous revision of task force criteria to include LV descriptions.
A previous study showed that LV late gadolinium enhancement was the most sensitive indicator of LV involvement. 12 A localized LVLE occurred even without concomitant WMA or volume expansion. 11 More and larger studies are needed to evaluate the predictive value, sensibility, and specificity of CMR in the diagnosis of LV involvement in ARVD/C.
Study Limitations
Although the data were recorded prospectively, the study was a retrospective monocentric study. Another limitation was the relatively small number of patients explained by the rareness of the disease and many underrecognized patients. No genetic analyses were made. There were no enough data about all family members. The impact of LV involvement in ARVD/C on the prognosis could not be fully evaluated because of the small population study.
Conclusion
LV involvement in ARVD/C is common and not always associated with severe RV abnormalities. It seems to occur earlier in the natural history, and appears rather as a biventricular cardiomyopathy. Larger studies are needed to determine the potential predictive value of LV in the prognosis of the disease.
The LV CMR assessment could be of great value for the diagnosis of LV involvement in ARVD/C. More studies focused on LV assessment by CMR are needed to define specific diagnostic criteria of LV-ARVD/C.
Author Contributions
Conceived and designed the experiments: SE, PG. Analyzed the data: SE. Wrote the first draft of the manuscript: AN, SE. Contributed to the writing of the manuscript: SE, PG. Agree with manuscript results and conclusions: PG, Mi-YJ. Jointly developed the structure and arguments for the paper: SE, AN. Made critical revisions and approved final version: PG, Mi-YJ, AG, CR. All authors reviewed and approved of the final manuscript.