
Abstract
Hydatid disease is an indolent parasitic infection caused by Echinococcus. The disease is transmitted through the ingestion of uncooked, contaminated vegetables and can infect almost any human organ, commonly the liver, followed by the lung, and rarely the heart. A computed tomography scan is the modality of choice for identifying hydatid cysts, and magnetic resonance imaging is for identifying complications. The definitive treatment includes surgery, with the possible use of antihelmintics in inoperable cases. To avoid fatal complications, hydatid disease must be treated as soon as it is diagnosed. This case highlights a peasant farmer rearing livestock who presented with chest pain and was incidentally found to have a mass in the left ventricle by transthoracic echocardiography. Further imaging found a large hydatid cyst in the left ventricular wall that was causing chest pain, possibly from the mass effect or compression of the left anterior descending artery.
Keywords
Introduction
Hydatid disease is a zoonotic parasitic infection caused by the tapeworm species of the genus Echinococcus (E. granulosus, E. multilocularis, E. vogeli, or E. oligarthrus), which is transmitted to humans from animals. 1 Transmission occurs when humans swallow the parasite eggs from unwashed or uncooked vegetables contaminated by dog feces. Any organ can be affected by the parasite embryo that enters the bloodstream through the intestine. Up to 75% of people typically have liver involvement through the portal vein. If the liver is bypassed, the infection can reach the lungs (up to 15%) via the inferior vena cava, as other organs are infected in less than 5% of cases. 2
Hydatid disease is endemic in the Mediterranean region, the Middle East, the Baltic region, South America, India, China, and other sheep-raising areas. 2 According to the World Health Organization, there are more than 50 cases of human infection for every 100,000 person-years, with the prevalence being up to 10% in echinococcosis-endemic areas. 3
This case report demonstrates a middle-aged man with chest pain who, upon initial evaluation, was diagnosed to have a hydatid cyst in the left ventricle (LV). This report highlights the incidental findings of an LV hydatid cyst and the possible management options.
Case Report
A 40-year-old male presented with chest pain, worsening on exertion and relieved with rest, for three months prior to his visit to the hospital. He did not complain of difficulty breathing or of any constitutional symptoms of fever, night sweating, or weight loss. Apart from occasional smoking, there were no other comorbidities identified. He was a peasant farmer, rearing livestock, specifically cattle, sheep, and poultry, and kept dogs for security. He reported no relief from multiple visits to the nearby health clinics. On examination, he was comfortable at rest, with no obvious clinical findings.
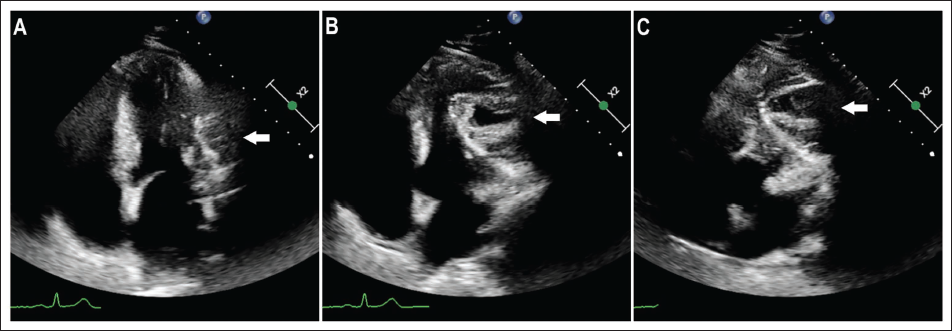
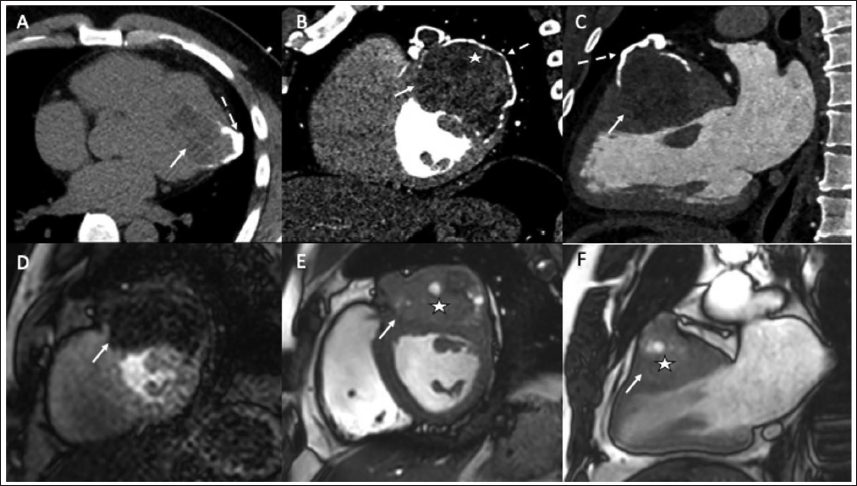
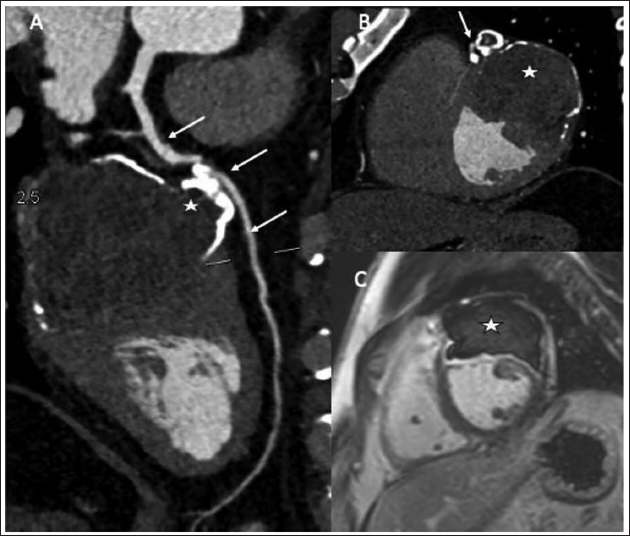
Initial hemoglobin was 13.3 g/dL with normal biochemical parameters. A chest radiograph did not show any significant abnormalities. An echocardiogram revealed an extracardiac mass compressing the anterior wall of the LV, whereby it could be visualized but not delineated (Figure 1), initially suspecting a complex cyst. A multidetector computed tomography (MDCT) of the heart demonstrated a lobulated hypodense lesion in the anterior wall of the LV, measuring 7 × 6 cm in maximum dimensions, with internal cystic areas and peripheral capsular calcification (Figure 2). The location of the lesion was very atypical, but the appearance was highly suggestive of a hydatid cyst. The left anterior descending (LAD) artery was abutting the lesion in the proximal aspect with unclear fat planes (Figure 3). Cardiac magnetic resonance (CMR) imaging was performed for better characterization of the mass lesion. The anterior wall of the LV was involved by this multiseptated mass lesion with a few cysts within (Figure 2). This showed poor perfusion and patchy peripheral areas of enhancement on late gadolinium enhancement imaging as compared to the normal myocardium (Figure 3). Cross-sectional image features were consistent with those of a myocardial hydatid cyst. A differential diagnosis would have included a complex cyst with prior infection, though quite rare in the heart. Other remote possibilities of pericardial cysts and primary cardiac tumors were not considered due to the location and morphology of the lesion. Additionally, hydatid cysts were not visualized in the liver or lung.
Echocardiogram Showing (A) a Four-chamber View in Diastole; (B) a Four-chamber View in Systole; and (C) a Modified View to Visualize a Mass (Arrow) in the Anterior Wall of the Left Ventricle.
Multiple Images from Multidetector Computed Tomography (A, B, and C) and Cardiac Magnetic Resonance Imaging (D, E, and F) Clearly Showing the Lesion in the Anterior Wall of the Left Ventricle (White Arrow). The Plain Computed Tomography Study (A) Showing the Calcification (Broken Arrow) Along the Periphery of the Lesion, Similarly Seen in Images B and C. Perfusion Images of the Cardiac Magnetic Resonance Imaging (D) Showing no Perfusion of the Lesion Compared to the Myocardium. Cardiac Magnetic Resonance Imaging (and, to an extent, image B) Clearly Demonstrating Daughter Cysts Within the Lesion (stars in B, E, and F). Notice the Near-Complete Involvement of the Myocardium with no Clear Dissection Planes.
The Multidetector Computed Tomography (A and B) and Cardiac Magnetic Resonance Imaging (C) Showing the Hydatid Cyst (Star) and Its Close Proximity to the Left Anterior Descending Artery (arrow). Notice the Lack of Clear Fat Planes Between the Lesion and the Left Anterior Descending Artery. Late Gadolinium Enhancement (C) Image Showing a Central Nonenhancing Lesion with Mild Peripheral Enhancement.
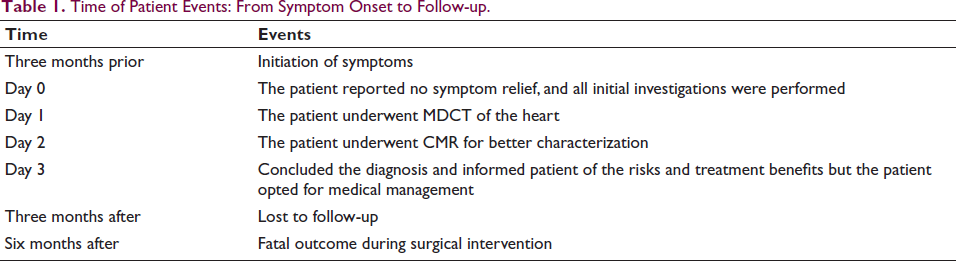
Upon review of the imaging studies, the patient was diagnosed with cardiac hydatid disease and was advised to undergo surgical excision of the mass on the LV. However, the patient was reluctant, and the risks were explained to the patient, but the patient opted for medical management. Oral albendazole 400 mg twice a day was initiated, and the patient was advised to follow up after three months; however, the patient had lost follow-up. After multiple attempts to contact the patient and family, it was informed that the patient had clinically worsened with chest pain and fever and had gone to a nearby hospital. Surgical intervention was attempted, but the outcome was fatal. The timeline of patient events is shown in Table 1.
Time of Patient Events: From Symptom Onset to Follow-up.
Discussion
The heart is a rare site for hydatid cysts, with an incidence of up to 2%.4 The multiple sites of cardiac involvement include the LV (50%–60%), pericardium (10%–15%), right ventricle (5%–15%), atrium and atrial appendage (5%–8%), pulmonary artery (6%), and interventricular septum (4%).4, 5 However, each endemic region might have different rates of cardiac involvement.
The primary hepatic or lung hydatid cyst rupture is the common route by which the larvae enter the heart, either through direct spread or the coronary circulation. The factors that may lead to LV involvement include dominance of the left coronary artery, the bulk of the LV wall, and ventricular high pressure. 5 However, in our case, there was right coronary dominance. The LV offers optimal conditions for the growth and development of the parasite because of its large myocardial mass and varying pressures. After the hydatid cysts rupture, the pulmonary vein is the second possible route for cardiac infection, as other possible routes include superior and inferior vena cava, intestinal lymphatic vessels, and hemorrhoidal veins of large bowel loops. 5
The disease can remain asymptomatic in up to 90% of cases with cardiac involvement. However, complications may occur due to a mass effect or cyst rupture, depending on the location of the hydatid cyst. These include heart failure, mitral regurgitation, coronary artery disease, atrioventricular block, paroxysmal supraventricular tachycardia, pericarditis, pericardial effusion, cardiac tamponade, pulmonary embolism, stroke, anaphylaxis, and death. 6 The hydatid cyst can compress blood vessels, causing coronary constriction, and in our case, the pressure effect of the cyst affected the LAD artery.
Transthoracic echocardiography may be limited in identifying the relationship between the cyst and adjacent structures. When demonstrating fluid-attenuating cystic structures, which may include daughter cysts, internal septations, and calcifications, MDCT and CMR are useful modalities to use. CMR is more useful in assessing the true extent of the lesion and its extension into adjacent structures. On CMR, these lesions have high T2 and low T1 signal intensities, with a characteristic low signal intensity peripheral ring secondary to calcification.4, 5 Therefore, MDCT is best for illustrating calcification, while CMR is best for illustrating complications.
The definite treatment is excision of the hydatid cyst via open-heart surgery, which is crucial to patient survival. Medical treatment with antihelmintics has a role in reducing the size and stopping the development of cysts, which is an option in inoperable cases. However, 400 mg of albendazole or mebendazole twice a day for five years is crucial in a postoperative setting to prevent recurrence. 7
Cardiac hydatid cysts are an uncommon but serious condition that is not associated with a high mortality rate when diagnosed and treated early. Rupture of the cyst during surgery, pulmonary embolism, and multiorgan failure have been noted as the causes of mortality in cardiac hydatid cyst patients. 8
The learning points in this case report are isolated cardiac hydatid cysts are rare (<2% of infected patients); the presentation may vary, as this case presented with angina-like symptoms; and MDCT is best for illustrating calcification, while CMR is best for illustrating complications.
In conclusion, hydatid disease is a parasitic infection that is indolent and can affect any organ. Suspicion should be made, especially in endemic regions with unclear clinical histories. Treatment for cardiac hydatid cysts must begin as soon as a diagnosis is made in order to avoid fatal complications, as the definitive treatment is surgical removal. Clinicians should be aware of such cases to better identify and execute management as early as possible.
Footnotes
Acknowledgements
We thank the patient and family for their co-operation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.