
Abstract
The objective was to investigate the effects of CT-guided lumbar sympathicolysis on somatic regional oxygen saturation, arterial flow velocity, and skin temperature of the lower limbs in patients with advanced peripheral artery disease (PAD). CT-guided lumbar sympathicolysis was additionally performed after successful revascularization therapy in 61 patients with PAD in categories 5 and 6 according to Rutherford. Somatic regional oxygen saturation in the distal lower limbs was determined semiquantitatively with a near-infrared spectroscopy (NIRS) system. Before and after intervention, peak flow and end-diastolic flow velocity in the dorsalis pedis artery were determined by means of color-coded duplex sonography, and the skin temperature of the feet was measured with an infrared thermometer. After CT-guided lumbar sympathicolysis, somatic regional oxygen saturation, peak flow, end-diastolic flow velocity, and skin temperature in the lower limbs increased significantly.
Keywords
Introduction
Peripheral artery disease (PAD) is characterized by an impairment of circulation of the limbs as a result of stenoses or occlusions of the supplying arteries. The severity of symptomatic PAOD ranges from intermittent claudication to critical limb ischemia (CLI). If left untreated, critical ischemia of the limbs can lead to non-healing wounds, gangrene, and ultimately, amputation. PAD is classified on the basis of clinical symptoms according to Rutherford or Fontaine et al.1,2 In grade III, the Rutherford classification distinguishes between patients with small distal ulcerations of the toes (category 5) and more proximally located necrosis (category 6).
Besides the major arteries, the smaller arterial vessels of the terminal vascular bed are often involved in PAD. The tone of the smooth vascular muscles, and thus the vascular cross-section, is subject to autonomic regulation via vasoconstrictor fibers of the sympathetic nervous system. The vessel-dilating effect of sympathetic denervation has been known for many years.3–5 In CT-guided lumbar sympathicolysis, the image-guided chemical neurolysis of the sympathetic chain is performed at the level of the third lumbar vertebral body. 6 Sympathetic denervation leads to a relaxation of the vascular muscles to vasodilation and to an increase in blood flow.
The objective of this observational prospective cohort study was to examine whether, in patients with advanced peripheral artery disease, computed tomography (CT)-guided lumbar sympathicolysis performed in addition to endovascular or surgical therapy leads to a measurable change in regional oxygen saturation, arterial flow velocity, or skin temperature of the distal lower limbs as a measure of peripheral circulation.
Material and Methods
Patients
Sixty-one patients with PAD categories 5 and 6, according to Rutherford in whom, after percutaneous transluminal angioplasty (PTA) or vascular surgery, a continuous arterial vascular supply from the pelvic axis to the foot via at least one lower leg artery, without higher grade stenoses, could be demonstrated by angiography were included in the analysis. Patients who received lumbar sympathicolysis for improvement of collateralization because of proximal stenoses or vascular occlusions and who lacked reconstructive therapeutic options were excluded. The presented method of treatment is a routinely used method in our clinic. Also because of the observational nature of this research and the minimal risk of NIRS, color coded duplex sonography and temperature measurement, ethical approval was not required. The research was conducted in accordance with the principles of the Declaration of Helsinki, and patients gave their written, informed consent to participate.
Sympathicolysis
CT-guided lumbar sympathicolysis was generally performed bilaterally, although this was done in two sessions one to two days apart, starting on the clinically dominant side. The interventions were performed in local anesthesia under sedation with 2-5 mg midazolam i.v. and insufflation of 3 L of oxygen per minute via a nasal tube. Planning of the intervention was done with the patient in the prone position on a craniocaudal spiral-CT of the central lumbar spinal region (LV 2-4). After specification of the approach at the level of the pedicle of LV 3, prior skin disinfection, and local anesthesia, dorsolateral puncture was performed with a 22G Chiba biopsy needle (length 10-20 cm), which was advanced lateroventrally of the third lumbar vertebral body (Fig. 1). If the needle position was correct, an average of 10 mL (5-15 mL) of a medication mixture consisting of 8 mL of 96% ethanol, 2 mL of 0.5% bupivacaine (Carbostesin®), and a little contrast medium was administered portionwise under repeated CT control scans (three to five scans/intervention), in which the distribution of the medication mixture was checked (Fig. 2).

Right dorsolateral puncture with a 22G Chiba biopsy needle in the right-sided CT-guided lumbar sympathicolysis.

A CT scan in the case of right-sided lumbar sympathicolysis: intercavovertebral positioning of the puncture needle and distribution of the sympatholytic agent.
Near-infrared spectroscopy
Near-infrared spectroscopy (NIRS) is a non-invasive optical method for measuring tissue oxygenation. Detection is conducted in the near-infrared range at a wavelength of 700-1300 nm. The change in the absorption spectrum of hemoglobin (Hb) in relation to the level of oxygenation is used to measure regional oxygen saturation. If there is an increase in focal blood flow in relation to focal oxygen consumption, a decrease in deoxygenated Hb and an increase in oxygenated Hb occurs. The modified Lambert–Beer law describes the connection between light absorption and a change in the concentration of dissolved chromophores. 7 By conducting spectroscopic measurements at different defined wavelengths, changes in the ratio of oxygenated and deoxygenated Hb can be measured continuously and non-invasively. This enables conclusions to be drawn about tissue oxygenation and blood circulation. 8
During the CT-guided lumbar sympathicolysis, somatic regional oxygen saturation in the distal lower limbs was measured using the commercially available NIRS system INVOS 5100C (Covidien) (Fig. 3). The INVOS 5100C utilizes an emitter (LED) with wavelengths of 730 and 810 nm as well as two detectors at a distance of 30 and 40 mm from the emitter. The absorption measurement of the chromophores (oxyhemoglobin and deoxyhemoglobin) with two detectors and a proprietary subtraction algorithm makes it possible to express the ratio of oxyhemoglobin to deoxyhemoglobin as regional oxygen saturation (rSO2).9,10
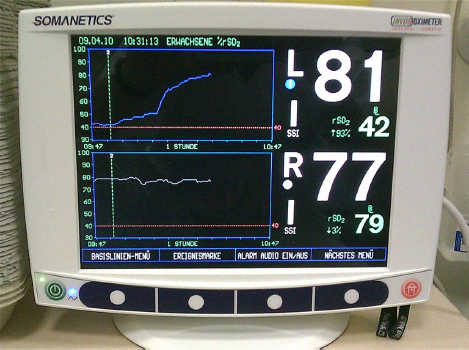
Monitor unit of the INVOS 5100C.
The sensor pads were placed on the lateral dorsum of the foot (Fig. 4). After acclimatization of 10-15 minutes, the baseline was specified. During sympathicolysis, the deviation from the baseline was recorded continuously up to the onset of a plateau phase.

Placement of the sensor pads of the INVOS 5100C on the feet.
Color-coded duplex sonography
Before and after sympathicolysis, the peak flows and the end-diastolic flows in the dorsalis pedis artery were determined by means of duplex sonography (LOGIQ 5 Expert, GE Healthcare).
Skin Temperature Measurement
For skin temperature measurement on the feet, an infrared ear thermometer was used (Braun ThermoScan 6021). After positioning of the patient on the CT table and an acclimatization phase of 10-15 minutes, pre-interventional temperature measurement was performed on the lateral dorsum of the foot. The measuring points were marked with a skin marker pen (Fig. 5). The post-interventional temperature measurement was done immediately before transferring the patient from CT table to bed.

Measurement of skin temperature with an infrared thermometer.
Statistical Analysis
Calculation of statistics was done with the aid of the program package IBM SPSS Statistics Version 20 (SPSS Inc.).
For description of the data, the mean ± standard deviation (SD) was stated.
The measurement values collected were tested with the Kolmogorov–Smirnov adaptation test and the Shapiro—Wilk test for normal distribution.
The potential differences before and after sympathicolysis with regard to the normally distributed measurement values were tested with the t-test for independent samples. The differences in the non-normally distributed measurement values were tested with the Wilcoxon test.
The Mann–Whitney U-test was used for subgroup comparison.
The level of significance (two-tailed) was set at P = 0.05.
Results
A total of 61 patients with advanced PAD in stages 5 and 6 according to Rutherford were investigated. In all, 39 patients (63.9%) were male and 22 patients (36.1%) were female. Their age was between 41 and 97 years, on the average 69.0 years. Overall, 30 patients (49.2%) had diabetes mellitus (Table 1). A total of 39 patients (63.9%) received bilateral sympathicolysis. In 9 patients (14.8%), an exclusively left-sided sympathicolysis was performed. In 13 patients (21.3%), sympathicolysis was only performed on the right. A total of 104 interventions were performed on 61 patients. Of these, 53 (51.0%) were right-sided sympathicolysis and 49 (49.0%) were left-sided sympathicolysis.
Diabetes – Rutherford stage* crosstab.

Rutherford stage 5: minor tissue loss, ischemic ulceration not exceeding ulcer of the digits of the foot. Rutherford stage 6: major tissue loss, severe ischemic ulcers, or frank gangrene.
During injection of the sympatholytic agent, a marked increase in regional oxygen saturation occurred in the foot on the treated side. The contralateral side was only affected to a minimal degree (Fig. 6A). After intervention on the contralateral side, an increase in regional oxygen saturation also occurred there and there was an adaptation to the other side (Fig. 6B).
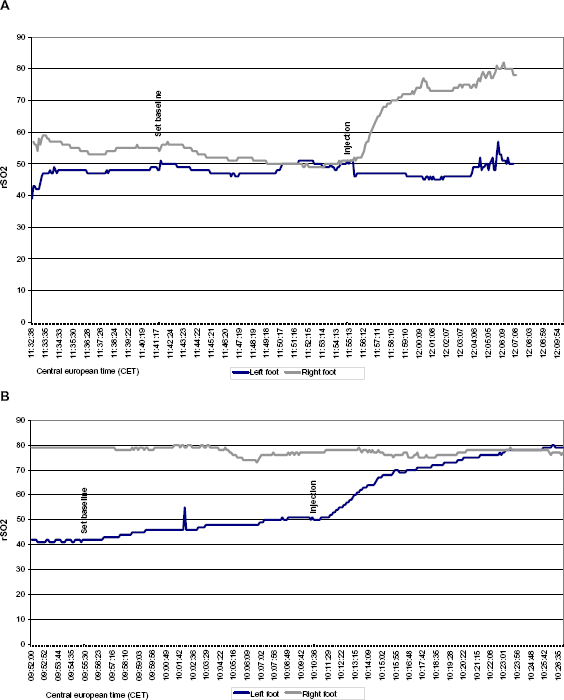
Regional somatic oxygen saturation in the feet during (
The mean values of the regional somatic oxygen saturation in the foot of the treated side increased significantly (baseline 62.99 ± 12.92% vs. follow-up 71.33 ± 12.59%, P < 0.001).
The peak flows in the dorsalis pedis artery increased (baseline 51.51 ± 27.30 cm/second vs. follow-up 63.09 ± 30.33 cm/second, P < 0.001).
After sympathicolysis, an increase in end-diastolic flow velocity occurred (baseline 7.43 ± 7.66 cm/second vs. follow-up 18.86 ± 12.03 cm/second, P < 0.001).
In addition, there was a significant increase in skin temperature in the foot of the treated side (baseline 32.2 ± 2.10 °C vs. follow-up 33.7 ± 1.90 °C, P < 0.001).
The peak flow increased by 16.01 cm/second in patients without diabetes mellitus vs. 3.87 cm/second in patients with diabetes mellitus (P = 0.039). No significant differences were seen with regard to oxygen saturation (P = 0.318), skin temperature (P = 0.757), and end-diastolic flow (P = 0.064) between the groups with and without diabetes mellitus (Table 2).
Descriptive statistics – diabetes.

In category 5, according to Rutherford, the end-diastolic flow increased by 15.2 vs. 8.4 cm/second in stage 6 according to Rutherford (P = 0.031). No significant differences were seen between categories 5 and 6 according to Rutherford with regard to oxygen saturation (P = 0.140), skin temperature (P = 0.328), and peak flow (P = 0.251) (Table 3).
Descriptive statistics – Rutherford stage.

Systemic side effects were not recorded. A total of 2 of 61 patients reported regional inguinal dysesthesia after sympathicolysis. After four weeks, the symptoms had completely regressed.
Discussion
The aim of therapy in advanced PAD is to salvage the limb. Besides reconstructive measures such as PTA or vascular surgery, CT-guided lumbar sympathicolysis can contribute to an improvement in peripheral circulation in advanced peripheral artery disease. 11 Dilation of the peripheral vessels achieved by sympathicolysis improves the healing of necroses and contributes to longer term patency of the reconstructed vessels by increasing flow.12,13
For objectification of the vessel-dilating effect of sympathicolysis in the limbs, previous investigations successfully used the ankle brachial index, 14 thermographic measurements, 14 sweating tests, 6 plethysmographic circulation measurements, 15 MR spectroscopy, 16 nuclear medical perfusion tests, 13 color-coded duplex sonography, 12 as well as skin resistance measurements.17,18 However, these methods are in part very time consuming and require considerable expenditure for equipment.
In the present study, CT-guided lumbar sympathicolysis led to a significant increase in regional somatic oxygen saturation in the foot of the treated side. No significant differences were found between diabetics and non-diabetics. The contralateral side was only affected to a minimal degree. This supports the concept of bilateral sympathicolysis. NIRS was first described by Jobsis in 1977. 8 The first clinical applications of NIRS were focused on cerebral circulation.19–22 In more recent investigations, NIRS has been used to investigate oxygen consumption and circulation of the skeletal muscles.23–25 Initial near-infrared spectroscopic investigations on muscular oxygen deficiency in the limbs used inflatable cuffs and excessive muscular exertion to simulate ischemia.26–29 Several investigations on PAD followed.30–42 Kooijman et al showed a significant connection between reoxygenation and ankle brachial index after walking exercises. 30 Fadel et al found a significant reduction in tissue oxygenation and blood flow after sympathetic nerve stimulation. 27 NIRS can detect changes in tissue oxygenation in the distal lower limb semiquantitatively in real time during CT-guided lumbar sympathicolysis. Changes in regional somatic oxygen saturation can already be measured during injection of the sympatholytic agent, which makes the method particularly suitable for the peri-interventional monitoring of peripheral circulation.
After sympathicolysis, vascular denervation and the decreasing tone of the smooth vascular muscles lead to dilation of the vessels and a decrease in peripheral resistance. As a result of this, peak flow and end-diastolic flow in the color coded duplex sonography increase significantly. In addition, there is a qualitative change in the Doppler flow profile, with an increase in end-diastolic flow. The increase in peak flow was less pronounced in patients with diabetes than in patients without diabetes. Patients with large-area necroses (Rutherford category 6) showed less of an influence on end-diastolic flow than patients with small-area necroses (Rutherford category 5). Clearly, the sympathetically mediated tone of the smooth vascular muscles is still maintained at least in part even in the case of advanced arteriosclerotic changes. The lesser influence on end-diastolic flow in the case of larger necroses can be explained by the preexistent vascular dilation caused by local inflammatory processes. Color-coded duplex sonography enables a qualitative and quantitative assessment of peripheral circulation. The qualitative change in the flow profile with increased end-diastolic flow is comparatively insensitive to environmental influences and can still be demonstrated even months after the intervention. The results of CCDS are consistent with those of other authors. 12 As a result of low sensitivity toward environmental influences, Doppler sonography is the method of choice for course controls and follow-up.
After lumbar sympathicolysis, the skin temperature of the foot on the treated side increases significantly. Temperature measurement is a known method for monitoring the effect of sympathicolysis. Using thermographic measurement after lumbar sympathectomy, McCollum et al found a temperature increase of more than 1.5 °C in 81% of the patients. 14 In Nickel et al, 86% of the patients reported a sustained improvement in the feeling of warmth and a reduction in pain symptoms in relation to forced claudication distance after lumbar sympathicolysis. 12 Apart from thermography, various thermometers are available for measuring temperature. Besides infrared thermometers specifically designed for measuring skin temperature, thermometers developed in particular for measuring body temperature in the auditory canal are now widely used. Both forms can be used equally with high precision for measurement of skin temperature in the limbs. Skin temperature shows a good correlation with intramuscular temperature in the limbs. 43 Measurement of skin temperature with an infrared ear thermometer before and after sympathicolysis is easy and inexpensive to perform. However, the temperature measurement is affected by external factors such as the ambient temperature and is predominantly suitable for peri-interventional monitoring of peripheral circulation.
Near-infrared spectroscopic measurement of regional somatic oxygen saturation, color-coded duplex sonography, and skin temperature measurement are suitable, non-invasive, and inexpensive methods for assessing the effect of CT-guided lumbar sympathicolysis on the distal lower limbs and for multimodally verifying the positive effect of lumbar sympathicolysis on circulation.
Limitations
No comparison with a control group was carried out. The study is not randomized. The semiquantitative measuring of regional oxygen saturation with the commercial INVOS system using a proprietary measurement algorithm also has limitations and is restricted reproducible. After recanalization of the lower leg arteries, the measurement region was not adapted to the angiosome of the recanalized vessel. The positioning of the NIRS sensors and ultrasound measurements were performed in a standardized manner in the coverage area of the dorsalis pedis artery.
In conclusion, the study shows an increase in blood flow in the feet through lumbar sympathicolysis beyond the effect of revascularization. Whether this also influences the course of disease was not included in the present study. Only if future, prospective, randomized, controlled studies clarify whether lumbar sympathicolysis prolongs amputation-free survival, sympathicolysis may become a part of the medical guidelines. Until then, sympathicolysis is usually reserved for patients with severe PAD threatened by amputation.
Author Contributions
Conceived and designed the experiments: IB, RA. Analyzed the data: IB. Wrote the first draft of the manuscript: IB. Contributed to the writing of the manuscript: IB, CW, RA. Agree with manuscript results and conclusions: IB, CW, RA. Jointly developed the structure and arguments for the paper: IB, CW, RA. Made critical revisions and approved final version: IB, CW, RA. All authors reviewed and approved of the final manuscript.