
Abstract
Background
Thyroid gland dysfunction and echocardiographic cardiac abnormalities are well-documented in patients with transfusion dependent beta-thalassemia major (β-TM).
Aim
This cross-sectional analytic study was conducted to investigate left ventricle (LV) diastolic and systolic function using pulsed Doppler (PD) and tissue Doppler (TD) echocardiography and correlate that with serum level thyroid stimulating hormone in patients with β-TM.
Methods
The study was conducted on patients with β-TM (n = 110, age 15.9 ± 8.9 years) and compared with a control group (n = 109, age 15.8 ± 8.9 years). In all participants, echocardiographic indices of PD and TD were performed and blood samples were withdrawn for measuring the serum level of TSH, free T4, and ferritin. A linear regression analysis was performed on TSH level as the dependent variable and serum ferritin as independent. Stepwise multiple regression analysis was used to determine the odds ratio of different biochemical and echo variables on the risk of developing hypothyroidism.
Results
Patients with β-TM compared with controls had thicker LV septal wall index (0.65 ± 0.26 vs. 0.44 ± 0.21 cm/M2, P < 0.001), posterior wall index (0.65 ± 0.23 vs. 0.43 ± 0.21 cm/m2, P < 0.01) and larger LVEDD index (4.35 ± 0.69 vs.3.88 ± 0.153 mm/m2, P < 0.001). In addition, β-TM patients had higher transmitral E wave velocity (E) (70.81 ± 10.13 vs. 57.53 ± 10.13 cm/s, P = 0.02) and E/A ratio (1.54 ± 0.18 vs. 1.23 ± 0.17, P < 0.01) and shorter deceleration time (DT) (170.53 ± 13.3 vs. 210.50 ± 19.20 m sec, P < 0.01). Furthermore, the ratio of transmitral E wave velocity to the tissue Doppler E wave at the basal septal mitral annulus (E/Em) was significantly higher in the β-TM group (19.68 ± 2.81 vs. 13.86 ± 1.41, P < 0.05). The tissue Doppler systolic wave (Sm) velocity and the early diastolic wave (Em) were significantly lower in the β-TM group compared with controls with Sm, 4.82 ± 1.2 vs. 6.22 ± 2.1 mm/sec, P < 0.05 and (Em), 3.51 ± 2.7 vs. 4.12 ± 2.5 mm/sec. P < 0.05, respectively). The tricuspid valve velocity was significantly higher in β-TM patients compared with controls 2.85 ± 0.56 vs. 1.743 ± 0.47 m sec, respectively, P < 0.01). The prevalence of subclinical hypothyroidism in patients with β-TM was 15.4%, with significantly higher mean serum TSH compared with controls (6.78 ± 1.5 vs. 3.10 ± 1.02 μIU/mL, P < 0.01) and positively correlated with the serum ferritin level (r = 0.34, P = 0.014). On multiple regression analysis, the LV mass, LVEF%, and E/A ratio were not positive predictors of hypothyroidism in patients with β-TM.
Conclusion
We conclude that patients with β-TM had a high prevalence of subclinical hypothyroidism of 15.4%. Thyroid stimulating hormone was significantly high and positively correlated with the serum ferritin level. Echo cardiographic pulsed Doppler showed a restrictive LV diastolic pattern suggestive of severe diastolic dysfunction with preserved left ventricle systolic function.
Keywords
Introduction
Dysfunction of the thyroid gland is a substantially well-documented endocrine complication in patients with blood transfusion dependent beta-thalassemia major (β-TM). 1 Because of hemolysis of red blood cells and repeated blood transfusion in such patients, they end up with iron overload. 2 The iron deposition adversely affects the structure and function of the myocardium, thyroid gland, and other organs. 3 Treatment with iron chelating therapy in patients with β-TM is considered the standard care of this blood disorder, leading to improvement of morbidity and an increased rate of survival. 4
Studies of left ventricle (LV) function by echocardiogram (echo) provided with pulsed and tissue Doppler in patients with β-TM has shown variable abnormalities depending on the patient's age and the severity of the disease.5,6 The diastolic function of LV has been classified into abnormal relaxation, pseudonormal, and restrictive pattern depending on the ratio of LV early diastolic filling velocity (E wave) to the late filling velocity (A wave). 7
The filling pattern of LV during diastole depends on the degree of predominance of the abnormal active relaxation or altered wall stiffness. The restrictive pattern is characterized by high E wave velocity, decreased A wave velocity, and shortened deceleration time (DT) with a high E/A ratio.7,8
The tissue Doppler echocardiography (TD) can detect regional myocardial diastolic dysfunction even in the early phases of cardiac injury. 9 The tissue velocity at the basal septum of the mitral annulus has been evaluated as a marker of myocardial stiffness, and in one report, it was suggested that the ratio of early diastolic filling wave (E) velocity to mitral annulus velocity (Em) correlates positively with the LV end-diastolic pressure (LVEDP). 10 Furthermore, it was shown that TD velocity of the early diastolic wave (Em) and systolic wave (Sm) velocity were both reduced in stiff hypertensive myocardium. 11
Previous studies in hyper-transfused β-TM patients showed variable prevalence of hypothyroidism ranging from 0% to 35% depending on the age of the study population, duration of blood transfusions, the level of serum ferritin, and the dose of the iron chelating agent.12,13
The aim of this study was to examine the relationship between the serum levels of thyroid stimulating hormone, ferritin, and echocardiographic indices of pulsed and tissue Doppler in patients who had transfusion-dependent β-TM.
Material and Methods
This study included 110 patients with transfusion-dependent β-TM and 109 healthy individuals who were used as a control group. A constitutional ethical approval was obtained for the study.
The study was conducted over a 12-month period from January 2011 to December 2011. Patients' selection was consecutive from those who were on regular follow-up in the Pediatric Hematology Clinic of the Salmaniya Medical Complex (SMC) in Bahrain. In the control group, patients were healthy with no hepatic or renal disease, had normal LV function on echocardiogram, and negative blood tests for thalassemia. They were selected from the pool of age-matched healthy patients who were referred for evaluation of systolic murmur and turned out to have normal echo. The time frame for echo and blood tests was one week. The blood sampling in the β-TM group and the echo test were carried out at the end of the week prior to the blood transfusion.
Patients were excluded if they had an end-stage renal disease with creatinine clearance < 30% of normal, severe liver disease, advanced heart failure, or hypertension cardiomyopathy.
Clinical and biochemical variables
Each patient in the study had a clinical and hematological data file that included duration of disease, cardiovascular assessment for heart rate, jugular venous pressure wave, apex beat, blood pressure, heart sounds and any murmurs, ankle edema, body weight, and signs of hypothyroidism such as delayed ankle reflex, coarse facial features, and rough skin. Blood levels of hemoglobin, serum ferritin, thyroid stimulating hormone, free thyroxin (FT4), and creatinine were recorded.
Doppler echocardiography
Each patient in the study had the echo examination by 2.5-5 MHz transducer, using an HP E33 echo machine. The echocardiography tests were performed by an echo technologist who was blinded about the clinical condition of the patient. Data were reported as an average of at least five cardiac cycles. Another echo technician analyzed the data blindly, and the average of the two readings was recorded. All measurements were conducted according to the recommendations of the American Society of Echocardiography (ASE). 14
Each patient enrolled in the study had echocardiographic measurements including M-mode, 2D echo, color flow, LV systolic and diastolic transmitral indices, and tissue Doppler evaluation of the septal mitral annulus. The M-mode echo parameters included the LV septal wall thickness, posterior LV wall thickness, mid and basal LV cavity dimension in (LVESD) and diastole (LVEDD). LV fractional shortening (FS%) and LV ejection fraction percentage (LVEF%) were measured using Teichholz formula: V = {7.0/(2.4 + D) * D3}. 15 Pulsed Doppler was acquired in the apical view, while patient in the partial left lateral decubitus position during the end of expiration, with sample volume situated between the mitral leaflet tips.
The LV diastolic filling indices including early diastolic wave (E wave), late diastolic wave (A wave), E wave to A wave (E/A) ratio, and deceleration time of E wave (DT) were all measured with the sample volume at the tip of the mitral leaflets in the apical view. The tricuspid valve velocity in systole (cm/s) was measured in apical view. The tissue Doppler velocity of the septal mitral annulus, early filling E wave velocity (Em), the calculated E/Em ratio, and the systolic wave (Sm) were all recorded as a mean of five readings.
Patients' were subdivided into two groups based on age difference, group 1 with patients' age between 3 and 10 years (n = 41), and group 2 with patients' age between 11 and 28 years. The age subdivision in the two groups was arbitrary and the intention was to evaluate the impact of age difference on the occurrence of hypothyroidism in patients with β-TM.
Statistical analysis
All the data were entered and analyzed using the Statistical Package for the Social Sciences (SPSS) version 17.0. Data are presented as mean ± SD. Unpaired Student t test was used to analyze the differences between the variables in the control and the β-TM groups. The M-mode dimensions of the LV were adjusted and indexed for body surface area (BSA) of each patient. Linear regression analysis was used to assess the correlation between the serum level of TSH as dependent variable and ferritin as the independent variable. The correlation coefficient (r) of the slope was then calculated. The mean of tissue Doppler indices taken at septal mitral annulus ring of the LV were corrected for heart rate.
Stepwise multiple regression analysis was used to determine the odds ratio of different variables on the risk of developing hypothyroidism. The variables were age, sex, serum level of creatinine, LVEF%, E/A ratio, and LV mass.
All other pulsed and tissue Doppler indices for systolic and diastolic functions were corrected for heart rate, such as E wave velocity, A wave velocity, DT, Em, E/Em, and Sm. Differences between groups were considered statistically significant at a probability value of < 0.05.
Results
The demographic data of all β-TM patients and the healthy controls are summarized in Table 1. The β-TM patients had a significantly lower body surface area compared with control patients (1.02 ± 0.2 vs. 1.15 ± 0.2, P < 0.05). There was no significant difference in the mean age between the β-TM group (15.7 ± 8.9 years, range 5-28) and the control group (15.9 ± 8.3 years, range 3-29) with comparable gender distribution between the two groups.
Demographic characteristics of control (n = 109) and thalassemia patients (n = 110) in the study.
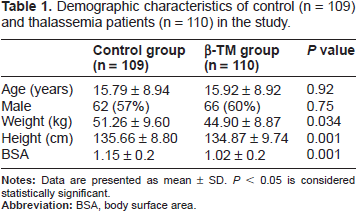
Table 2 shows the hemodynamic and biochemical variables in both groups. The systolic and diastolic pressure values were comparable in both groups. The heart rate was lower in the β-TM compared with the control group (68.16 ± 7.4 vs. 72.92 ± 6.1 BPM respectively, P < 0.05). The serum ferritin level was significantly higher in the β-TM group compared with the control group (5124 ± 1931 μg/L vs. 164 ± 48 μg/L, P < 0.001). There were no significant differences in serum levels of creatinine and hemoglobin between the two groups.
Hemodynamic and biochemical parameters in beta thalassemia (β-TM) patients on deferasirox (20 mg/ kg/day) and the control group.

The significantly low heart rate in β-TM patients could be due to the low state of T4 however other signs of hypothyroid were not detected.
The mean level of serum FT4 concentration was with in the normal range of 14.3 ± 2.4 pmol/L in all patients in the control group with a range of 8 to 27 pmol/L, and it was in the low normal range of 9.5 ± 1.9 pmol/L in patients. The mean serum level of TSH in the control group was 3.10 ± 1.02 μIU/mL and 6.78 ± 1.5 μIU/mL in the β-TM group. The mean difference of high TSH and low FT4 were statistically significant.
There were 17 (15.4%) patients with high TSH and 5 patients with TSH higher than 10 μIU/mL, and 10 had TSH level of 7 to 10 μIU/mL. Lower levels of FT4 were detected at 5.3 pmol/L in 9 patients and the rest were > 8.2 pmol/L.
Linear regression analysis showed a postive correlation between serum levels of TSH as the dependent variable and serum ferritin (r = 34, P = 0.014). Step-wise multiple regression analysis was conducted to determine the odds ratio of different variables on the risk of developing hypothyroidism. The odds ratio for age was 0.991 (95% CI, 0.918-1.071, P = 0.83); sex, 0.423 (95% CI, 0.137-1.306, P = 0.125); creatinine, 1.039 (95% CI, 0.985-1.096, P = 0.162); LV mass index, 1.005 (95% CI, 0.971-1.039, P = 0.761); LVEF%, 0.91 (95% CI, 0.780-1.065, P = 0.243); and E/A ratio, 0.409 (95% CI, 0.56-3.22, P = 0.409).
No patients with high TSH levels had any sign of hypothyroidism. There were 16 (94%) patients in group 2 with age > 10 years, and only one was in group 1 (6%), age < 10 years.
No patient had positive results for antimicrosomal antibody (thyroid peroxidase antibody).
Echocardiographic findings
Table 3 summarizes the indexed pulsed M-mode values in both the control group and the β-TM group. The β-TM group showed significantly higher LV wall thickness manifested by significantly thicker posterior wall and interventricular septum (P < 0.001 in both). The LV dimensions at the end of systole (LVESD) and diastole (LVEDD) were significantly larger in β-TM compared with the control group. The left ventricle mass was significantly higher in the β-TM group compared with the control (152.85 ± 25.3 vs. 87 ± 14.76, respectively, P < 0.001).
Indexed M-mode and 2D echocardiography findings in beta thalassemia (β-TM) patients and the control group.

Compared with the control group, patients with β-TM had slightly lower LVEF% and FS, but these differences did not achieve statistical significance.
Table 4 shows the pulsed and tissue Doppler indices of the LV in both groups. The pulsed Doppler diastolic indices of LV showed significantly higher E wave and E/A ratio in β-TM group compared with control with significantly shorter interval of DT time. The ratio of transmitral E wave velocity to TD (Em) of the septal mitral annulus (E/Em) was significantly higher in the β-TM group compared with the control group (P < 0.05), while the early diastolic velocity (Em) and the systolic wave velocity (Sm) were significantly lower in the β-TM group (P < 0.05).
The heart rate corrected diastolic pulse and tissue Doppler indices for thalassemia (β-TM) patients and the control group.

The LV fractional shortening and LVEF% at the midcavity sector were not significantly different between the two groups.
The tricuspid valve velocity was significantly higher in the β-TM group (P < 0.01). In the group of patients with β-TM, the color flow pattern and continuous wave velocity of the LV inflow and outflow showed mild mitral regurgitation in nine patients, and three patients had mild aortic regurgitation with none in the control group.
Discussion
In this study, patients with β-TM were evaluated for thyroid function clinically and biochemically with pulse and tissue Doppler echocardiogram for systolic function and diastolic indices of the left ventricle compared with age-matched individuals with no β-TM.
Thyroid dysfunction in β-TM patients has been reported with variable prevalence, with a low range of 0% to 12%.16–18 or a high of 16% to 35%.19–21
The variation of prevalence in the past may be related to different methods used for thyroid function studies, different ages in the study population, or different medications. In one study by Masala et al, 22 the prevalence of hypothyroidism diagnosed by concentration of T4 and TSH was only 5%, whereas hypothyroidism diagnosed by TRH stimulation test increased the dysfunction rate up to 35%. However, since TRH is rarely used, concentrations of T4 and TSH have been commonly used and accepted for the evaluation of thyroid function. In this study, the prevalence of abnormal thyroid function was 15.4%, which is in the higher range. The high prevalence in our patients may be a reflection of the poor compliance with the iron chelating therapy and the low dose of oral deferasirox, as evidenced by the very high serum ferritin levels.
The significantly low heart rate in β-TM patients in the absence of coarse facial features and normal ankle reflex may be the single most clinical manifestation of hypothyroidism in this population.
In one study by Grundy et al, 16 a lower prevalence of hypothyroidism was observed among those with serum ferritin levels < 2500 μg/L.
In our patients, there was a positive linear relationship between thyroid dysfunction with high TSH levels and ferritin levels. When multiple logistic regression analysis was used to predict the hazard of developing hypothyroidism, there was no positive predictor of hypothyroidism found among the different demographic and biochemical variables included, including creatinine, LVEF%, LV mass, and E/A ratio; however, the positive linear relation between serum TSH and ferritin has not been reported in previous studies.20,21
The diastolic indices of LV in β-TM patients showed higher early diastolic filling of LV and E/A ratio, suggesting a restrictive diastolic pattern and stiff myocardial wall. These findings are in keeping with one study by Yaprak et al 23 who demonstrated that β-TM patients had significantly higher E wave, E/A ratio, and lower A wave velocity, suggesting a restrictive pattern but with no correlation with hemoglobin level. Similar observations were reported by Spirit et al 24 who demonstrated a restrictive pattern in patients with β-TM with no heart failure. This was also in agreement with a previous report that a high E/A ratio is the most common finding in patients with β-TM. 25
The decreased DT of E wave was mostly related to the increased amplitude of the E wave and may be due to the impaired relaxation of LV with a constrictive pattern. The exact mechanism of these findings is not known but may be due to iron overload and increased stiffness of the LV wall.
The tissue Doppler ratio of E/Em was significantly higher in β-TM patients compared with controls. Likewise, the early diastolic velocity (Em) and the systolic velocity wave (Sm) of the basal septum were significantly reduced, suggesting stiff myocardium and possibly high LVEDP. These findings are in agreement with those previously reported in hypertensive patients.26,27
The LVEF% and fractional shortening in the midcavity sector were normal indicating that β-TM patients are having a preserved systolic function. In the current study, the serum ferritin was more than 30 times higher in the β-TM group compared with controls. These findings confirm our previously published studies that iron overload appears to mediate the impaired diastolic function leading to stiffness of the myocardial wall but with well-preserved LV systolic function. 28 It seems in this population, as observed previously, that myocardial disease goes through a stage of impaired relaxation before development of systolic dysfunction.5,6 This finding is in agreement with one report where patients with β-TM with no heart failure had higher E/Em– ratio compared with controls. 25
In the β-TM group, the increase ratio of E/Em ratio compared with the control group is highly suggestive of stiff myocardial wall and increased left ventricular end diastolic pressure. 26
Conclusion
We conclude that patients with β-TM had a high prevalence of subclinical hypothyroidism of 15.4%. The age of onset was mainly between 10 and 28 years. Thyroid stimulating hormone was significantly high and positively correlated with serum ferritin level.
Echocardiographic pulsed Doppler showed a restrictive LV diastolic pattern, suggestive of severe diastolic dysfunction with preserved left ventricle systolic function.
Author Contributions
Conceived and designed the experiments: NAM. Analysed the data: TSG. Wrote the first draft of the Manuscript: ZAH. Contributed to the writing of the manuscript: AMJ. Agree with manuscript results and conclusions: DSN. Jointly developed the structure and arguments for the paper: TSG. Made critical revisions and approved final version: TSG, NAM, AMJ, ZAH, DSN. All authors reviewed and approved of the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.