
Abstract
Background
Doppler echocardiographic studies of left ventricle (LV) systolic and diastolic function in patients with β-Thalassemia Major (β-TM) had shown different patterns of systolic and diastolic dysfunction.
Aim
This cross-sectional study was designed to study the LV systolic and diastolic function in patients with β-TM using Pulsed Doppler (PD) and Tissue Doppler (TD) echocardiography.
Methods
All patients were evaluated clinically and by echocardiography, The study included patients with β-TM (n = 38, age 15.7 ± 8.9 years) compared with an age-matched control group (n = 38, age 15.9 ± 8.9 years). The pulse Doppler indices were normalized for age and heart rate.
Results
Compared with control patients, M-Mode showed that patients with β-TM have thicker LV septal wall index (0.659 ± 0.23 vs. 0.446 ± 0.219 cm, P ≤ 0.001), posterior wall index (0.659 ± 0.235 vs. 0.437 ± 0.214 cm, P ≤ 0.01), and larger LVEDD index is (3.99 ± 0.48 vs. 2.170 ± 0.57 mm. P = 0.035). Pulsed Doppler showed high LV trans-mitral E wave velocity (70.818 ± 10.139 vs. 57.532 ± 10.139, p = 0.027) and E/A ratio (1.54 vs. 1.23, P ≤ 0.01). The duration of Deceleration time (DT) and isovolumic relaxation time (IVRT) were significantly shorter in patients with β-TM (150.234 ± 20.0.23 vs. 167.123 ± 19.143 msec, P ≤ 0.01) and (60.647 ± 6.77 vs. 75.474 ± 5.83 msec, P ≤ 0.001), respectively. The ratio of transmitral E wave velocity to the tissue Doppler E wave at the basal septal mitral annulus E/Em– was significantly higher in β-TM group (14.024 ± 2.29 vs. 12.132 ± 1.82, P ≤ 0.01). The Tissue Doppler systolic velocity (Sm) and the early diastolic velocity (Em) were significantly lower in β-TM group compared to control (4.31 ± 1.2 cm/s vs. 6.95 ± 2.1, P ≤ 0.01 and 4.31 ± 2.7 cm/s vs. 5.82 ± 2.5, P ≤ 0.01) respectively. The tricuspid valve velocity was significantly higher than controls (2.993 ± 0.569 vs. 1.93 ± 0.471 m/sec, respectively, P ≤ 0.01). However, the LVEF% and fractional shortening were normal with no significant difference in both groups.
Conclusion
In this study, patients with β-thalassemia major compared with controls, have significantly thicker LV wall, and larger LV cavity and LV diastolic filling indices suggestive of restrictive pattern with a higher tricuspid valve velocity. These data showed that left ventricle diastolic indices are compromised initially in patients with β-thalassemia major.
Introduction
Beta-Thalassemia Major (β-TM) is a genetic blood disorder caused by reduced synthesis of β-globin chain. The consequences of chronic anemia include growth retardation, bone marrow expansion, extra-medullary hematopoiesis, splenomegaly, greater intestinal iron absorption, hypercoagulability and higher susceptibility to infection.1,2 Patients are usually maintained on continuous blood transfusion regimens to keep hemoglobin levels close to normal and allow adequate tissue oxygenation. Because of the hemolysis and repeated blood transfusion, β-TM is associated with iron overload. 3 The iron deposition could adversely affect both the structure and function of the heart. Previous studies indicated that patients with β-TM develop ventricular systolic dysfunction leading to congestive heart failure. 4
LV Diastolic filling pattern has been classified into normal, restrictive and abnormal relaxation pattern on the basis of early filling E wave and late filling A wave on LV trans-mitral diastolic filling. 5 The filling pattern depends on the degree of predominance of the abnormal active relaxation or altered wall stiffness. The restrictive pattern is characterized by high E wave velocity, decreased A wave and shortened Deceleration Time (DT) with high E/A ratio ≥1.29.6,7 In one report, the DT of E wave velocity of ≤180 msec predicted LA pressure ≥20 mmHg. 8
The tissue Doppler echocardiography (TD) is a non-invasive technique that can detect regional myo-cardial diastolic dysfunction even in early phases of cardiac injury. 9 The tissue velocity at the basal septum of mitral annulus has been evaluated as a marker of myocardial stiffness, and in one report it was suggested that the ratio of early diastolic filling wave (E) to mitral annulus tissue Doppler (TD) velocity (E/Em) correlates positively with the LV end-diastolic pressure (LVEDP), as the E/Em ≥15 predicts high LVEDP ≥ 15mmHg. 10 In one study, the TD early dia-stolic velocity Em and the systolic wave Sm were reduced in hypertensive patients. 11
The National Student Screening Project in Bahrain indicated that the prevalence of β-TM in high school students is 0.09%, with β-thalassemia trait representing 2.9% of the sample population. 12 Similar findings were observed in a study targeting subjects seeking premarital screening in Bahrain. 13 The echocardio-graphic changes in patients with β-TM had not been previously studied in Bahrain. Evaluation of cardiac function by echo Doppler can assist in staging the disease progression and may help to prevent further cardiac damage by applying intense chelating regimens and combination therapy. 14
Thus, the aim of this study is to use pulsed Doppler echo (PD) and TD in assessing myocardial systolic and diastolic functions in young patients with β-TM in Bahrain.
Subjects and Methods
This study included 38 patients with transfusion-dependent β-TM and 38 patients with no thalassemia were used as a control group. The study was conducted during the interval from January 2009 to June 2009. A constitutional ethical approval was obtained for the study.
Inclusion and Exclusion Criteria
Selection was consecutive from patients who are on regular follow-up in Pediatric Hematology clinic at Salmaniya Medical Complex (SMC) in Bahrain. Patients were included if they had a follow-up for more than 3 years at SMC, with a confirmed diagnosis of β-TM based on electrophoresis. Selected patients have been receiving blood transfusions every three weeks to maintain hemoglobin levels above 9 g/dl since infancy. All patients had also been receiving desferrioxamine as a chelating therapy (25-50 mg/kg body weight by subcutaneous infusion with an infusion pump for 8-12 h) regularly for at least one year. In the control group, patients were healthy with no renal or hepatic disease, no valve disease, normal LV function on echo and negative blood tests for thalas-semia. They were selected from the pool of healthy patients who are referred for evaluation of systolic murmur and turned to have normal echo. The time frame for the echo Doppler and the blood test is one week. The control patients’ age was counted to match the study patients. The blood samples in the control group and echo test were carried out in the week prior the blood transfusion. Patients were excluded if they have end stage renal disease with creatinine clearance of ≤30% of normal, severe liver disease, diabetes mellitus, hypoparathyroidism, advanced heart failure, hypertrophic cardiomyopathy or if the patient is taking active cardiac medications. Each patient in the study had a clinical and haematological data file including duration of disease, cardiovascular assessment for pulse rate, jugular venous pressure wave, apex beat, blood pressure, heart sounds and presence or absence of murmur, ankle edema and body weight. Data of the blood hemoglobin, serum Ferritin and creatinine concentrations were all recorded.
Doppler Echocardiography
Each patient in the study and control group had the echo examination by 2.5-5 MHz transducer, using HP E33 echo machine. The echocardiography test and the values measured were performed by an echo technologist who was blinded for the clinical condition of the patient. Data were reported as an average of at least five cardiac cycles. Another echo technician analyzed the data blindly and the data were taken as an average of the two readings. The acquisition sector were according to the criteria of the American Society of Echocardiography. 15 Each patient enrolled in the study had echocardiographic measurements including M Mode, 2D echo, color flow, systolic and LV diastolic transmitral indices and tissue Doppler evaluation of the septal mitral annulus.
The M mode measurement study of the left ventricle was performed under 2D echo controls. The septal and posterior wall thickness in cm, LV cavity diameter in diastole and systole were measured in long parasternal view with M-Mode beam just distal to the tips of mitral leaflet and at the papillary muscle level in short axis (mid cavity). The left ventricle mass was calculated as previously reported. 16 Pulsed Doppler acquired in the apical view, while patients in the partial left lateral decubitus position during end of expiration, with sample volume situated between the mitral leaflet tips. The peak velocity of early rapid filling (E velocity) and the peak velocity of the atrial filling (A velocity) were recorded and the E/A ratio was calculated. The time of E wave deceleration was measured as the interval between the peak E velocity and the point at which the descending segment crosses the zero line. The isovolumic relaxation time is measured in the apical four chambers as the time in ms from the aortic valve closure and the onset of the mitral flow. The tissue Doppler velocity is taken at the septal mitral annulus in the apical view. The early diastolic velocity (Em), the systolic velocity (Sm), and the ratio of E/Em were all measured. The velocity tracing was read as a mean of five measurements.
The intra-observer variability between the pulsed Doppler measures was assessed in 20 thalassemia patients who were examined twice, with one week apart. The mean differences ± SD were -0.002 ± 0.035-1 m/s for peak E velocity, -0.004 ± 0.061 m/s-1 for A velocity and 0.017 ± 0.164 for the E/A velocity ratio.
The M mode echo parameters including the left ventricle (LV) septal wall thickness, posterior LV wall thickness, mid and basal LV cavity dimension in systole and diastole as well as the LV end diastolic volume. LV fractional shortening (FS) and LV ejection fraction percentage (LVEF %) were measured using Teicholz formula: V = {7.0/(2.4 + D)*D 3 }.
The left ventricle diastolic filling indices included early diastolic wave (E wave), late diastolic wave (A wave), deceleration time of E wave (DT), isovolu-mic relaxation time (IVRT) and E wave to A wave (E/ A) ratio were all measured with the sample volume at the tip of the mitral leaflets in the apical view. The IVRT, DT and all Pulsed Doppler velocities and ratios were corrected for age and heart rate of each patient in the study. The tricuspid valve velocity in systole in cm/s was measured in apical view. The tissue Doppler velocity of the septal mitral annulus, early filling E wave velocity (Em), the calculated E/Em ratio and the systolic wave (Sm) were all were recorded as a mean of five readings and corrected for age and heart rate. The septal mitral annulus ring was chosen to measure the tissue Doppler rather than the lateral because the changes in left ventricular hypertrophy and hypertension are more pronounced and marked in the mitral annulus rather than in the other wall.17,18
Statistical Analysis
All data were entered and analyzed using the Statistical Package of Social Sciences (SPSS) version 17.0. Data are presented as mean ± SD. Unpaired student t-test was used to analyze the differences between the variables in the control group and patients with β-TM. The M-mode dimensions of the LV were adjusted and indexed for Body Surface Area (BSA) of each patient in both groups. Linear regression analysis was used to assess the linear relationship between the serum ferritin as the independent variable and ratio of the transmitral early velocity of pulsed Doppler (E) to the tissue Doppler velocity (Em) of septal mitral annulus. Regression lines of (heart rate and age) for each variable in the study were analyzed and the slope of each variable was calculated. The pulsed and Tissue Doppler indices were calculated for E/Em ratio normalization using the following equation:

Each parameter was adjusted for age and heart rate and the mean value in each group was measured and compared with the control group. All other pulsed Doppler and tissue Doppler for systolic and diastolic functions were corrected or normalized for age and heart rate such as: E wave velocity, A wave velocity, DT, IVRT, Em, E/Em, and Sm. Differences between groups were considered statistically significant at a probability value of ≤0.05.
Results
The demographic data of β-TM patients and the healthy controls are summarized in Table 1. The β-TM patients had a significant lower body surface area compared with control patients, (1.15 ± 0.2 vs.1.01 ± 0.2, P ≤ 0.05). The mean age for β-TM was 15.7 ± 8.94 year (range; 7-25), while the mean age of the control group was 15.9 ± 8.30 year (range; 6-24. The gender distribution between the two groups was comparable. The systolic and diastolic pressures values were comparable in both groups. In β-TM the heart rate was significantly higher of 27% in β-TM (92 ± 6.99 vs. 67.58 ± 7.26, P ≤ 0.001) compared with control group. The serum ferritin was significantly higher in the β-TM group compared with the control group (P ≤ 0.001). No significant differences in serum creatinine and hemoglobin level were found between both groups.
Demographic characteristics of thalassemia patients (n = 38, β-TM) and healthy controls (n = 38) in the study. Data are presented as mean ± sD. P value ≤ 0.05 is considered statistically significant.

Echo Doppler Findings
Table 2 summarized the raw (un-indexed) pulsed Doppler data and M-mode values in both control and p-TM groups. The &bT-TM group showed significantly higher LV wall thickness manifested by significantly thicker posterior wall and interventricular septum (P ≤ 0.001 in both). The LV dimensions at the end of systole (LVESD) and diastole (LVEDD) were significantly larger in β-TM compared with control group. The left ventricle mass was significantly higher (172 ± 65.3 vs. 87 ± 14.8, P ≤ 0.001) in β-TM group compared with the control. The Doppler indices of the LV diastolic filling showed significantly higher E wave, and E/A ratio in the β-TM group compared to control while significantly shorter interval of DT time of E wave and IVRT.
Unindexed Echocardiographic findings in thalassemia patients (n = 38) and the control group (n = 38) in the study. Data are presented as mean ± SD. P value ≤ 0.05 is considered statistically significant.

Table 3 showed the mean of Tissue Doppler indices taken at septal mitral annulus ring of the LV after being corrected for age and heart rate in each patient in the study.
The age- and heart rate-adjusted diastolic Doppler indices for β-thalassemia (β-TM) patients and healthy controls. Data are presented as mean ± SD. P value ≤ 0.05 is considered statistically significant.

The ratio of transmitral E wave velocity to TD (Em) of the septal mitral annulus (E/Em) was significantly higher in the β-TM group compared to the control group (P ≤ 0.01), the early diastolic velocity (Em) was significantly lower in β-TM group. Likewise, the systolic wave velocity (Sm) was significantly lower in the β-TM group compared to the control. However, no significant differences in fractional shortening at the base and at mid-cavity sector or in LV ejection fraction (EF%) were observed between the two groups. The normalized tricuspid valve velocity for age and heart rate was significantly higher in β-TM group. (P ≤ 0.01).
The E/Em ratio of tissue Doppler had a significant positive correlation with serum ferritin level (r = +0.74, P ≤ 0.001).
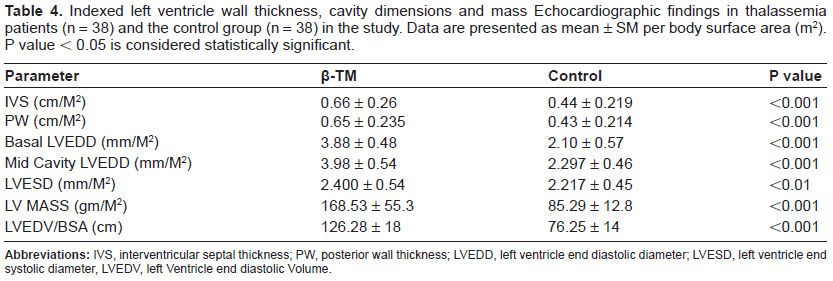
Table 4 showed the indexed data of the M-mode values for the LV wall thickness for septum and posterior wall, LV cavity dimension in systole and diastole as well as the calculated LV mass. The LV end diastolic volume was significantly high in β-TM (126.28 ± 18 ml vs. 76.25 ± 14 ml ≤ 0.001) compared with control. Both the un-indexed and the indexed data were significantly higher in the β-TM patients compared with controls. The color flow and continuous flow of the LV and RV in the β-TM group showed mild mitral regurgitation in nine patients and three patients had mild aortic regurgitation.
Indexed left ventricle wall thickness, cavity dimensions and mass Echocardiographic findings in thalassemia patients (n = 38) and the control group (n = 38) in the study. Data are presented as mean ± SM per body surface area (m2). P value ≤ 0.05 is considered statistically significant.
Discussion
In this study, patients with β-TM were evaluated with pulse and tissue Doppler echocardiogram for systolic and diastolic functions of left ventricle (LV) compared with age- and sex-matched controls. Compared with controls, the diastolic indices of LV in β-TM patients showed higher early diastolic filling of LV and high E/A ratio suggesting restrictive diastolic pattern and thus stiff myocardial wall. These findings are in keeping with another study by Yaprak et al 21 who demonstrated that β-TM patients (n = 63) had significantly higher E wave, E/A ratio, and lower A wave velocity, suggesting restrictive pattern in 54% in the study population; no correlation was found with hemoglobin level. Similar observations were reported by Spirit P et al 22 who demonstrated that transmitral diastolic filling measured by Doppler in patients with β-TM (n = 32, none of them had heart failure) was described of restrictive pattern. This was also in agreement with a previous report that high E/A ratio is the most common finding in patients with β-TM. 23 The left Ventricle (LV) diastolic filling measured by pulsed wave Doppler echocardiography reflect the diastolic filling characteristics of the LV and depends on various factors including LV ventricle relaxation, compliance, systolic function and loading conditions.24,25
In the current study, the tissue Doppler ratio of E/Em was significantly higher in β-TM patients compared with controls, the TD of early diastolic velocity (Em) and the systolic velocity wave (Sm) were significantly reduced, suggesting stiff myocardium and possibly high LVEDP. 26 These findings are in agreement with previously reported findings in hypertensive patients. 27
The LVEF% and fractional shortening in basal and mid cavity were normal with no difference between patients with β-TM and the control group. The normal LVEF% indicates that β-TM patients are having minimal deleterious effect of iron overload on myo-cardial systolic function and that was evident by the optimal level of serum ferritin in the study population. This may also explain the absence of heart failure or significant valve diseases in the current study population. In one report it was shown that the overall cardiovascular prognosis was good if the serum ferritin is below 2500 ng/dl. Serum ferritin levels ≤1000 ng/dl were associated with normal LVEF% while high levels were associated with low LVEF%. 28 In another study, however, right sided heart failure was reported in 16% of β-TM patients with high serum ferritin of ≥2500 ng/ml. 29 Therefore, the iron overload in the current study appears to mediate the impaired diastolic function leading to stiffness of the myocardial wall with mean pre-transfusion hemoglobin concentration of 9.5 gm/dl in the β-TM group, there is an increased dimension of LV cavity and LV volume in diastole. The increase of the volume load in this population may be a reflection of Frank Starling mechanism or due to increased heart rate in β-TM patients. This was observed by others who related the increment of LV volume to factors mediated by chronic anemia rather than iron overload. 30
In order to avoid the influence of the heart rate in this study, all the Doppler indices were normalized for the heart rate and the age. The echocardiographic measurements were all conducted during the week preceding the blood transfusion in order to eliminate the high volume effect on the pulse wave velocity. 31
The decreased DT time of E wave was mostly related to the increased amplitude of the E wave and may be due to the impaired relaxation of LV of constrictive pattern where the E wave is high with shorter DT and IVRT interval. This is probably due to iron overload and increased stiffness of LV wall. 32
In the β-TM group, the increase ratio of E/Em ratio compared with the control group is highly suggestive of stiff myocardial wall and an increased left ventricle end diastolic pressure.10,26,27 The significant high velocity of the tricuspid valve in β-TM compared to controls may be due to pulmonary diffusion defect, hypoxia or possibly airway obstruction due to iron overload.33,34
Conclusions
We conclude from this study that patients with β-thalassemia have larger left ventricle dimension, abnormal LV relaxation pattern suggestive of restrictive type and higher LV end-diastolic pressure, while the left ventricle ejection fraction is normal. These data suggest that abnormalities of diastolic indices are initial findings in patients with β-thalassemia major.
Disclosures
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors report no conflicts of interest.