
Abstract
Objective:
Some structural abnormalities have been reported on sonography of pancreas in patients with beta-thalassemia which can indicate that the patient is developing diabetes. In this study, the aim was to investigate the findings of pancreatic sonography in patients, with beta-thalassemia major.
Methods:
This cross-sectional study included information extracted from the medical record and entered into an information form. A cohort of 190 people were split into case and control groups, retrospectively. The required data were extracted from patient’s documents. Data were analyzed with SPSS software, version 22; with the chi-square statistical tests. A P value of < .05 was considered statistically significant.
Results:
This study consisted of 33 males and 61 females in the case group and 32 males and 64 females in the control group. The most common echogenicity observed during pancreatic sonography, in the control group, was an isoechoic feature (72.3%), followed by hyper and hypoechogenicity (18.1% and 9.6%, respectively). The prevalence of an isoechoic texture in the patient case group was 58.3%, while hyper and hypoechogenicity were seen in 26% and 2.1%, respectively (P = .070). There was a poor negative correlation between diabetes and pancreatic echogenicity (P = .002 and r = −.226). Also, there was a poor positive correlation between fasting serum glucose levels and pancreatic echogenicity (P = .034, n = 96 and r = .217).
Conclusion:
This study demonstrates, in this patient group, that there was a poor relationship between pancreatic head size with serum ferritin levels and pancreatic echogenicity with diabetes. These results may suggest using sonography to diagnose early stages of diabetes in patients with thalassemia.
Beta-thalassemia is a type of hemoglobinopathy, which is characterized by chronic anemia and is associated with absent or reduced beta globin chains within the hemoglobin tetramer. 1 Beta-thalassemia major (BTM) if left untreated can cause severe anemia leading to toxic and organic alterations, serious health implications, and possible death. It has been reported that in the Mediterranean, approximately 108 000 people may be suffering from this disease. 2 Beta-thalassemia major has been reported in 17 000 patients in European countries, as well. 2 It has been estimated that more than about 30 000 babies with BTM are born every year. 3 Regular blood transfusions have improved the life expectancy of these patients. However, this method is associated with specific complications such as iron accumulation in various organs (endocrine glands, myocardium, and liver) which can cause organ dysfunction. 4 Patients with BTM would require life-long chelation transfusion to prevent mortality caused by hemosiderosis and organ failure. The most common cause of death in these patients is heart failure; however, a great number of them struggle with endocrine disorders including diabetes mellitus, hypogonadism, pituitary failure hypoparathyroidism, and hypothyroidism. 5 Until a few years ago, patients with thalassemia used to die in the second decade of life. However, with medical advances, especially after iron chelation, there has been a great change in the treatment of these patients. Currently, proper treatment can guarantee a relatively long-life expectancy for patients with thalassemia. 6 Endocrine and exocrine disorders are of the major complications of BTM. The toxic effect of iron accumulation in beta and acinar cells of pancreas in addition to peripheral resistance to insulin can be the main mechanism through which patients with BTM develop diabetes. 7 However, most of the alterations that occurred in the pancreas are caused by an iron overload which has not been accentuated using chelators. The prevalence of diabetes mellitus in patients with BTM varies from 9.7% to 29%.8-10 Magnetic resonance imaging (MRI) has been introduced as a noninvasive method for evaluating myocardial and hepatic overload. In addition, some structural abnormalities have been reported during pancreatic sonography in these patients.11,12 Sonography has not been recommended for the use of early assessment of the pancreas and tailoring chelation based on those findings, as it could prevent organ damage. However, studies have confirmed that sonographic hyperechogenicity, of the pancreas, can be indicative of acute disorders that could lead to early management of the physical and psychological health of patients. 12 In this study, the aim was to investigate the findings of pancreatic sonography in patients with BTM.
Materials and Methods
A cohort of 190 people were split in a case and control group, retrospectively. Within the case group, there were 94 patients diagnosed with beta-thalassemia. The control group included 96 healthy children who were similar to the case group, in all aspects, except having beta-thalassemia and underwent sonography in the hospital, during this same time frame. Informed consent was obtained from the patients or their parents, following approval of the study protocol by the hospital ethics committee. All of the patients were under regular treatment with blood transfusion and iron chelators. The demographic and clinical data were extracted from their medical records which included age, sex, other diseases, treatment, ferritin level, number of blood transfusions, fasting blood sugar (FBS) level, diabetic and nondiabetic status, and imaging data. Given that three patients in the case group were diabetic, the results were analyzed in two diabetic and nondiabetic groups, as well. For those case study patients, a FBS test a day before blood transfusion was done. The ultrasound equipment that was used to evaluate the echo pattern of the pancreas was ATL—Ultra Mark 4p with a 5.0 MHz transducer. All of the sonograms were performed by the same experienced radiologist, who had 10 years of experience in abdominal radiology. All examinations were done after one night fasting. The patients were asked to lay in the Fowler’s position and asked to place their hands behind their back. The radiologist evaluated the echotexture of the pancreas, in reference to the liver echogenicity, which matches the technique used in previous studies. The sonographic results were assigned three grades for echogenicity: less echogenicity than liver, similar echogenicity to the liver, and more echogenicity than liver. The size of pancreas was measured on transverse/oblique images, using the maximum antero-posterior diameter of head and the body. Data were analyzed with SPSS software, version 22, with the chi-square statistical tests. A priori, a P value of <.05 was considered statistically significant.
Results
There were 190 patients who participated, and the gender consisted of 33 males and 61 females in the case group. Likewise, there were 32 males and 64 females in the control group. The mean patient ages were 17.92 ± 8.93 and 17.84 ± 7.40 years in the control and case groups, respectively. The average ferritin level in the patients with thalassemia was 2957 ± 1792.
The most common echogenicity status observed during pancreatic sonography in the control group was isoechoic (72.3%) followed by hyper and hypoechoic (18.1% and 9.6%, respectively). The prevalence of an isoechoic texture, in the case group, was 58.3%, while hyper, and hypoechoic textures were seen in 26% and 2.1%, respectively (P = .070) (see Table 1, Figure 1).
Description of Statistical Sample in Terms of Pancreatic Echogenicity and Pancreatic Dimensions.

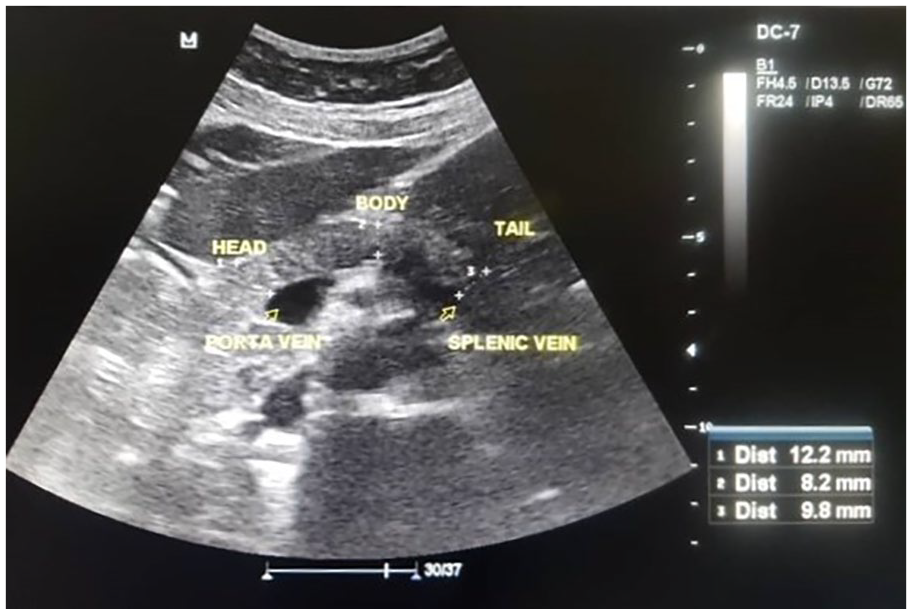
An example of a hyperechoic texture of the pancreas, in a patient with beta-thalassemia major.
Out of all 190 cases, three were diabetic, who all belonged to the case group, and the rest were nondiabetic. The mean FBS level in the case group was FBS 96.7 ± 48.71 mg/dL. The most prevalent echogenicity status in nondiabetic cases was isoechoic, while this type of echogenicity was not observed in any of nondiabetic patients. Based on the result of the Pearson correlation, there was a poor negative correlation between diabetes and pancreatic echogenicity (P = .002 and r = −.226). Also, there was a poor positive correlation between fasting serum glucose levels and pancreatic echogenicity (P = .034, n = 96, and r = .217).
In the control group, the average pancreatic head, body, and tail sizes were 12.26 ± 3.48 mm, 9.05 ± 2.23 mm, and 10.06 ± 2.57 mm, respectively, and the corresponding sizes in the case group were 11.82 ± 3.75 mm, 10.66 ± 2.68 mm, and 13.90 ± 3.93 mm, respectively. The difference was only significant between body sizes (P = .04). These differences were not significant between the diabetic and nondiabetic groups, as well (see Table 1).
In the study, the relationship between pancreas size (head, body, and tail) was also evaluated and the number of blood transfusion times in patients with BTM. There were no statistically significant associations found among these variables (P values: .98, .39, and .71, respectively).
Regarding serum ferritin level, there was a statistically significant relationship between serum ferritin level and the pancreas head size in patients with BTM (see Figure 2) (P = .027, R = .2). But the pancreatic body and tail sizes showed no significant relation to serum ferritin level (P values = .34 and .46, respectively). Also, there was no significant correlation between blood transfusions and pancreatic echogenicity (P = .114, n = 96 and r = .162). There was no significant correlation between serum ferritin levels and pancreatic echogenicity (P = .116, n = 96, and r = .161), as well.
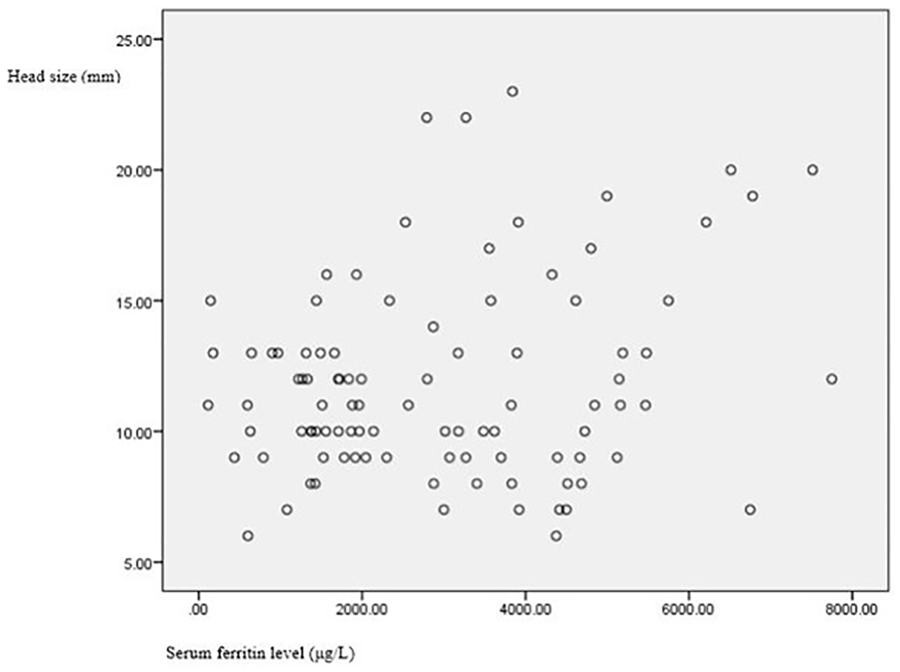
The scatter plot and the relation between pancreas head size and serum ferritin level.
Discussion
In this cohort comparison, the prevalence of diabetes among patients with BTM was 3.1%. The rate of BTM was 9.8% in a study by Pourn et al 13 and 18.3% in Mirzaei et al 14 which differs from the current study. With those patients with BTM evaluated, the incidence of diabetes was lower than compared to previous studies. There is also a difference in the prevalence of diabetes across countries, such as 4.9% in Italy to 19.5% in Taiwan.15-21 This variation may be due to the patient’s treatment, the time of onset, and the amount of deferoxamine taken. Conversely, the difference in the prevalence of diabetes in different studies can be due to the difference in patient ages. For example, in a study of 25 Italian hematology centers, the age of the patients was 2 years. Therefore, in this study, the prevalence of diabetes in this study was lower compared to other studies since it takes more than 10 years to cause glandular complications, due to thalassemia.
Echogenicity
In this study, the pancreas sonographic findings were 58.3% isoechoic, 26% hyperechoic, and 9.4% hypoechoic, in the patients with thalassemia. The highest echogenicity pattern found in patients without diabetes was isoechoic; however, this echotexture was not found in any of the diabetic patients. Moreover, 33.3% of diabetic patients had a hyperechoic pattern, a rate of 28.6% was also noted by Hashemipour et al, which compares favorably with the present cohort. However, a recent study using T2 MRI patient images found no significant difference in patients with BTM compared to nondiabetics.22,30 In the present study, there was no association between pancreatic echogenicity and serum ferritin levels or blood transfusion frequency (P < .05). In the cohort, 53.2% of patients with BTM had ferritin levels higher than 2500 µg/L. In a study conducted by Hashemipour et al, they divided 42 children with thalassemia into two groups: patients with high echogenicity (hyperechoic) and patients with normal echogenicity (isoechoic). The difference between serum ferritin level was significantly higher among the hyperechoic group than in the isoechoic group (P < .05). 22
Ferritin Level
Ferritin is an effective factor associated with insulin resistance. Its serum concentration which is an indicator of liver iron concentration is considered as an independent risk factor for diabetes and impaired glucose tolerance (IGT). Also, in epidemiological studies, ferritin constitutes an important component of the insulin resistance. 23 According to a study by Cavallo-Perin et al, insulin sensitivity, which is closely related to increased iron depletion, is reduced by 40% in patients with thalassemia. 24 In one study, a lower ferritin level of 2500 µg/L reduced the prevalence of diabetes in these patients, 24 and in another study, a lower ferritin of 1500 µg was effective in reducing the endocrine side effects of patients with thalassemia. 25
Correlations
A Greek study examined the importance and sensitivity of pancreatic sonographic results as a benchmark for pancreatic function in people with beta-thalassemia. The sonogram and oral glucose tolerance test (OGTT) studies were performed on 34 children with thalassemia. Based on the results, 5.76% of patients had increased pancreatic echogenicity, 77% of which had IGT and 5.37% had abnormal serum insulin concentrations. The researchers concluded that in patients with increased pancreatic echogenicity, the average level of glucose was higher during OGTT. So, this simple imaging technique can be seen as an indicator of the increased risk of developing diabetes in patients with thalassemia. 12 There was a significant correlation between diabetes and fasting glucose levels with pancreatic echogenicity, so that with increasing fasting glucose, pancreatic echogenicity increased. Due to the increasing tendency of glucose and insulin in patients with increased pancreatic echogenicity, pancreatic sonography could be used to diagnose the early stages of diabetes in patients with thalassemia.26,27 In a previous study, the authors indicated that 76% of their BTM cases had a decreased pancreatic size on the sonogram. They considered this as a factor showing the functional damage of pancreas. Therefore, in this study, it was decided to measure the pancreatic dimensions on the sonogram, as part of the data collection. In general, the size of the head, body, and tail of the pancreas was higher in patients with thalassemia than in healthy individuals, which was not statistically significant. Also, the average size of the pancreatic head, body, and tail, among diabetic thalassemia patients was higher than those without diabetes. These measurement differences were not statistically significant and there was no association between pancreatic dimensions in diabetic thalassemia patients. However, these results were likely limited by the small number of diabetic patients. Also, in the present study, no relationship was observed between the dimensions of the pancreas (size of the head, body, and tail) with the frequency of receiving blood and serum levels of fasting glucose. In a study by Gullo et al, the sonographic echogenicity of the pancreas and its size were collected with the serum pancreatic enzymes and these patient results were compared to a control group. Most of patients with thalassemia had a significant increase in pancreatic echogenicity and a decrease in pancreatic gland size. Both echogenicity and glandular size reduction were significantly associated with transfusion treatment time.28,29 The findings of the present study demonstrated that in this cohort, there was a weak association between pancreatic head size and serum ferritin levels. This may provide some lower-level evidence that patients with higher serum ferritin levels may have an enlarged pancreatic head. No association was found between the pancreatic size of the body and tail with serum ferritin levels.
Summary
This cohort study indicated that there was a poor relationship between pancreatic head size with serum ferritin levels and pancreatic echogenicity. It was noted that the higher the ferritin levels the smaller the pancreatic head size among this cohort of diabetics, which may suggest that sonography could be used to diagnose early stages of diabetes, in patients with thalassemia. Due to the limitation of the study design, these results need to be replicated in a larger group of patients.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.