
Abstract
Background
Elevated aminotransferase levels are commonly associated with compromised hepatic integrity from various insults. In sickle cell disease, aspartate transaminase (AST) is also released via intravascular hemolysis. This study was done to determine the pattern of changes in AST and alanine transaminase (ALT), in particular the AST:ALT ratio, and to relate these to the hemolytic state, which we consider to be more important than hepatic and cardiac dysfunction in some individuals with sickle cell disease.
Methods
Serum aminotransferase levels were measured in 330 subjects with sickle cell disease, as well as hemoglobin, reticulocytes, and lactate dehydrogenase. The AST:ALT ratio was designated as a hemolytic marker, and simple and multivariate regression analyses were carried out between this ratio and other hemolytic markers.
Results
Mean AST and ALT levels were 48.24 % 27.78 and 26.48 % 22.73 U/L, respectively. However, for 49 subjects without sickle cell disease, mean AST and ALT levels were the same, ie, 23.0 U/L. In the subjects with sickle cell disease, the increases in AST levels were far higher than for ALT, supporting its release via intravascular hemolysis. In 95.8% of the subjects with sickle cell disease, the AST:ALT ratio was > 1, but our results did not suggest overt malfunctioning of the liver and heart in the majority of subjects.
Conclusion
Regression analyses support the use of the AST:ALT ratio as a hemolytic marker, because it has an inverse association with the hemoglobin level. Whether in steady state or in crisis, provided hepatic and cardiac integrity has not been compromised, subjects with sickle cell disease would have higher AST levels due to the hemolytic nature of the condition. This is the first report highlighting the AST:ALT ratio in sickle cell disease.
Introduction
Liver function tests are carried out to investigate hepatic integrity, and the synthetic, storage, transport, secretory, and other functions of this important organ. Measurement of aspartate transaminase (AST) and alanine transaminase (ALT) are two of the common tests. Standard laboratory tests for liver function are often requested by doctors for patients with nonspecific symptoms, such as tiredness, abdominal pain, dyspepsia, and weight loss. 1 These tests enable the diagnosis of viral, metabolic, and autoimmune hepatic disorders, and are also used as a basis to select patients for transplantation and to support patients after liver allografts. 2
The release of cytoplasmic proteins from damaged hepatocytes into the vascular system precedes tissue necrosis caused by, eg, drug intoxication, ischemia and reperfusion injury, or rejection after liver transplantation. 4 Limdi and Hyde 5 assert that it is hepatocellular injury, and not necessarily cell death, which is the trigger for release of small proteins into the circulation. The serum activity presumably increases as a result of cellular membrane damage and leakage. 6
AST and ALT are widely distributed throughout the body, and participate in gluconeogenesis by catalyzing the transfer of amino groups from aspartate and alanine to α-ketoglutaric acid to form oxaloacetate and pyruvate, respectively, as well as glutamate. AST is found primarily in the heart, liver, skeletal muscle, red cells, and kidney, whereas ALT is found mainly in the liver and kidney, with lesser amounts in the heart and skeletal muscles.7,8
The liver of a patient with sickle cell disease shows congestion, siderosis, and hepatomegaly. 9 Liver pathology is also commonly related to viral hepatitis or hepatic iron deposition due to repeated transfusions.10,11 Hepatic crisis related to severe intrahepatic cholestasis and ischemic necrosis may also occur. 10 Worsening hemolysis related to increased sickling of red cells intrahepatically leads to sinusoidal dilatation, and probably causes abnormal liver chemistry.11,12
There is also substantial evidence that vaso-occlusive crisis is associated with intensification of hemolysis.23,24 This is further supported by an association of elevated serum lactate dehydrogenase with low levels of hemoglobin and high levels of reticulocytes and bilirubin.8,24,25 Castro et al 26 has also identified total hemoglobin concentration, bilirubin level, lactate dehydrogenase, and the arginine:ornithine ratio to be markers of hemolysis. The disproportionate correlation with AST, and not ALT, is consistent with higher concentrations of AST than ALT in red blood cells released during intravascular hemolysis. 27
The literature is replete with evidence that an AST:ALT ratio >1 signifies hepatic damage.13–15 The ratio can also be >1 in patients with myocardial infarction. 16 However, with red cells being a good source of AST, and given the hemolytic tendency in individuals with sickle cell disease, we hypothesized that such persons would have a high AST:ALT ratio independent of hepatic and cardiac damage.
Methods
Subjects and Setting
The subjects were outpatients with sickle cell disease attending the Sickle Cell Clinic at the Komfo Anokye Teaching Hospital in Kumasi. Patients who reported characteristic bony pain were deemed to be in crisis. On the other hand, those who had no complaints of pain, were asymptomatic in the preceding four weeks, and had not had a blood transfusion in the previous three months were deemed to be in a steady state. The subjects were aged 5-20 years.
Patients who were too sick and weak to be subjected to blood sampling were excluded. Those who had received emergency drug therapy were also excluded.
Given that sickling hemoglobinopathy is not genotypically homogenous, our subjects were grouped into three categories, ie, SS, SC, and unspecified. The last group could have been a heterozygous combination of S and the thalassemias (α or β), or some other genotype, but we were unable to determine the exact type. An apparently healthy group of 49 people without sickle cell disease (31 males and 18 females) were included as controls specifically for determination of AST and ALT activity, were aged 5-55 years, and had attended the Clinical Analyses Laboratory for medical diagnostic tests. They were not patients who had been referred from hospitals, but had reported voluntarily for a health check.
Collection of Blood Samples
About 5 mL of blood was taken from the antecubital vein and put into two sample tubes; one anticoagulated tube containing ethylenediamine tetra-acetic acid for plasma and a nonanticoagulated tube for serum. The study was cross-sectional for the majority of the subjects, thus the blood sampling was done once. However, for a small subset of subjects with sickle cell disease (n = 16), blood samples were taken twice over 1-6 months. This was to show if the trend of the changes being investigated followed the same pattern longitudinally.
Assay Methodology
ALT, AST, liquicolor, and lactate dehydrogenase test kits were supplied by Human Gesellschaft fur Biochemica und Diagnostica GmbH, Wiesbaden, Germany. The Humalyzer Junior spectrophotometer with a digital readout was used for the enzyme assays. Hemoglobin was assayed using the methemoglobin method, and reticulocytes were assayed using the brilliant cresyl blue manual method.
Statistical Analysis
The values of the various measured parameters were subjected to statistical analysis using Statgraphics 2006 (StatPoint Inc, Warrenton, VA). Means and standard deviations were calculated. The Spearman's nonparametric correlation test was used to determine possible associations between the parameters.
Ethical Approval and Informed Consent
The committee for human research, publication, and ethics for the School of Medical Sciences, KNUST, and the Komfo Anokye Teaching Hospital, Kumasi, granted ethical approval for us to perform this study. Informed consent was sought from parents/ caregivers of subjects younger than 18 years, and from participants who were 18 years and older.
Results
Changes in Transaminases of Patients with Sickle Cell Disease versus Controls
Mean AST and ALT levels in the overall population of 330 subjects were 48.2 % 27.78 U/L and 26.5 % 22.73 U/L, respectively. The highest AST measurement was 262 U, and the highest for ALT was 275 U. However, for 49 nonsickling subjects (31 males and 18 females), the mean AST and ALT levels were the same at 23.0 U/L.
In the smaller longitudinal study of 16 subjects, mean ALT and AST levels for the first determination were 22.8 and 50.0 U/L, respectively, while values obtained for the second determination were 22.9 and 41.8 U/L. The AST:ALT ratios for the two time points were 2.16 and 1.93.
Mean AST and ALT levels for the females with sickle cell disease were higher than in their male counterparts, while the mean AST:ALT ratio in males was higher (Table 2A), but these differences were not significant (
Classifying by genotype (Tables 1 and 2A), mean levels showed some differences. From Table 1, amongst the different genotypes of subjects with sickle cell disease, the SS genotype (n = 187) had the highest mean levels of AST and ALT (50.8 and 27.3 U/L, respectively), while the SC (n = 104) had the lowest mean AST level of 43.5 U/L. Sickle cell disease of unspecified genotype (n = 39) had the lowest mean ALT level at 23.5 U.
AST and ALT levels (U/L) in patients with sickle cell disease compared with those in normal subjects.

Comparison of AST, ALT and AST/ALT values of SS and SC
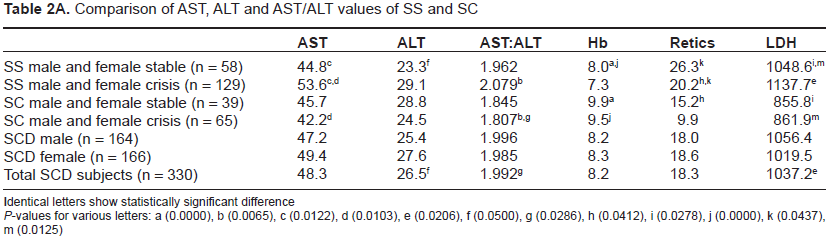
Identical letters show statistically significant difference
Between the genotypes, only the difference between the mean AST level for SC (43.5 U) and for SS (50.8) was statistically significant (
ALT and AST levels (U/L) and AST:ALT ratio at two different time points for 16 subjects with sickle cell disease.

The Figure 1 and Table 4 demonstrate that the lowest range of ALT (< 40 U/L) predominates for the SS and SC genotypes, whereas for AST, the 40-80 U/L range of activity is the most predominant for these genotypes. Up to 312 (94.5%) of the 330 subjects had ALT levels within the normal range (≤ 40 U/L). On the other hand, 137 (41.5%) had AST levels within the normal range, while the remaining 171 (51.8%) had AST levels of 40-80 U/L. In fact, 22 (6.7%) of the subjects had AST levels above 80 U/L.

Categorical AST and ALT levels of SS and SC genotypes.
Categorical ALT and AST levels (U/L) according to genotype.

Various ranges of ALT and AST according to genotypes and clinical states.

Overall, of the 330 subjects, only 14 (4.2%) had ALT levels higher than their AST levels, and in more than 95% of cases, AST levels were higher than for ALT. Mean AST and ALT levels in subjects without sickle cell disease were the same at 23.00 U/L, as shown in Table 1. AST was higher in 28 of the 49 controls, and ALT levels higher in 43.9% of cases. The magnitude of the increases in aminotransferase levels in the control group was lower than in the subjects with sickle cell disease. The highest AST level seen was 55 U, and the highest ALT level was 52 U. Three of the controls had AST levels above 40 U, while four had ALT levels above this cutoff value.
Ast:Alt Ratio
Generally, the AST:ALT ratio in patients with sickle cell disease tends to be higher than 1.0. The minimum level (0.17) was recorded in the male SC patient in crisis, and the highest (4.67) was in a SS female patient in crisis. From Table 2A, the SC male and SC female in crisis had the lowest AST:ALT ratio (1.807), and the highest (2.079) was in an SS male and an SS female in crisis. In contrast, the controls showed a mean AST:ALT ratio of 1.070 for males and 1.112 for females.
All the 330 subjects with sickle cell disease had a significantly higher AST:ALT ratio than the SC male and SC female in crisis (Table 2A). The highest ratio seen in the SS male and SS female in crisis was significantly different from that in the SC male and SC female in crisis. The longitudinal study involving 16 subjects gave ratios of 2.16 and 1.93 for the first and second determinations, respectively. These values are similar to those obtained in the cross-sectional study.
Regression Analyses between Ast:Alt Ratio and Hemolytic Markers
Regression analyses were carried out to find the association between the AST:ALT ratio and hemoglobin as well as other hemolytic markers, lactate dehydrogenase and reticulocytes. In the simple regression analyses, the AST:ALT ratio was the dependent variable, and hemoglobin, reticulocytes, and lactate dehydrogenase were the independent variables (Table 5).
Correlation coefficients (r) and

Data in brackets include SCD subjects of unspecified genotype.
Generally, there was a negative correlation between the AST:ALT ratio and hemoglobin levels. A striking feature is that it was in the crisis states that the relationship assumed high statistical significance, as seen in the SS and SC subjects in crisis (
In addition to the simple regression analyses, we carried out multivariate analyses, still keeping the AST:ALT ratio as the dependent variable, and hemoglobin, reticulocytes, and lactate dehydrogenase as the independent variables. The

Note:
Statistically significant.
The multiple regression analyses indicated that there were varying levels of association between the AST:ALT ratio and the hemolytic markers, but the association was only statistically significant (
In order to ascertain which of the independent variables weighted most in the association, a multiple regression analysis was performed for the AST:ALT ratio and some two-variable independent factors, to derive
Discussion
Our study has shown that individuals with sickling hemoglobinopathy have significantly elevated AST activity compared with controls without sickle cell disease (see Tables 1 and 2A).
AST is found primarily in the heart, liver, skeletal muscle, red cells, and kidney, whereas ALT is found mainly in the liver and kidney, with lesser amounts in heart and skeletal muscles.7,8 In most types of liver disease, ALT activity is higher than that of AST. Exceptions include alcoholic hepatitis and Reye's syndrome. ALT is regarded as a more specific biomarker of hepatocellular damage. 8
We believe that there could have been some cases of hepatic crisis amongst our patients, indicated by right upper quadrant pain, tender hepatomegaly, jaundice, and low-grade fever. According to a report by Sheehy, 3 acute sickle cell hepatic crisis occurs in 10% of patients.
Our observation that patients with sickle cell disease generally had higher AST than ALT levels supports previous findings of a mean AST of 57.6 U and a mean ALT of 33.5 U by Bayazit and Kilinc, 19 and a mean of 35.9 U for AST and 21.4 U for ALT by Richard and Billett, 20 implicating a hemolytic source for this enzyme. Consequently, we are proposing that in patients with sickle cell disease, in whom hepatic and cardiac integrity has not been compromised, the AST:ALT ratio could denote a hemolytic tendency.
The AST:ALT has also been evaluated by studies13,14 in patients with acute and chronic liver disease of various origins. In these patients, the AST:ALT ratio was reported to provide useful clinical information regarding both the cause and severity of liver disease. Because this variable is readily available, easy to interpret, and inexpensive, it has been used various studies in the past.
In a study by Giannini et al,15,21 it was shown that a progressive increase in the AST:ALT ratio is correlated with a concomitant decrease in liver function, and that an AST:ALT ratio ≥ 1 has good specificity and sensitivity for the diagnosis of cirrhosis. The higher mean AST levels associated with cirrhosis imply that the extent of fibrosis influences AST levels.21,22 It has been shown that plasma clearance of AST is modulated by sinusoidal liver cells, as progressive fibrosis and cirrhosis develops and sinusoidal function becomes progressively impaired, resulting in a relative increase in AST levels. 22 Cirrhosis and fibrosis were unlikely in our subjects because they had no signs and symptoms of liver disease, and had only modest elevations of both ALT and AST. Some few patients showed splenohepatomegaly, but there were no patients showing evidence of fluid accumulation, eg, ascites, edema, or unexplained weight gain.
Our data indicate that the higher elevation of AST relative to ALT is linked to a hemolytic tendency in sickle cell disease. There is substantial evidence that vaso-occlusive crisis is associated with intensification of hemolysis.23,24 This is further supported by an association of elevated serum lactate dehydrogenase with low levels of hemoglobin and high levels of reticulocytes and bilirubin.8,24,25 Castro et al 26 have also found total hemoglobin concentration, bilirubin level, lactate dehydrogenase, and the arginine:ornithine ratio to be markers of hemolysis. The disproportionately stronger correlation with AST than with ALT is consistent with higher concentrations of AST than ALT in red blood cells, which are released during intravascular hemolysis. 27 Billett et al 28 have reported that many of their patients with sickle cell disease had lactate dehydrogenase levels above 500 IU/L, and that the levels correlated with the number of dense cells.
From simple regression, as well as the multivariate analyses, as shown in Tables 4 and 6, it can be deduced that, being a hemolytic marker in people with sickle cell disease, the AST:ALT ratio has a negative correlation with hemoglobin, but a positive correlation with reticulocytes and lactate dehydrogenase. A high AST:ALT ratio implies the release of AST from red cells containing mutant and oxidant-stressed hemoglobin S, leading to lowered hemoglobin levels. The resulting hemolytic state evokes a prompt hemopoietic response (where there is effective erythropoiesis), leading to compensatory release of many young red cells together with nucleated red cells, a condition which is associated with increased activity of lactate dehydrogenase. Immature erythrocytes, including reticulocytes and nucleated red cells, reportedly contain increased levels of lactate dehydrogenase isozymes. 29
From the multivariate analysis of the AST:ALT ratio and other hemolytic markers in Table 6, only values for the SC males in crisis achieved statistical significance. It is possible that levels from the other groups could have been confounded by hepatic crises, causing loss of specificity of the AST:ALT ratio for hemolysis.
Patients with alcoholic liver disease due to alcohol-related vitamin B6 deficiency could have an AST:ALT ratio of ≥ 2, reflecting low serum ALT levels. 30 None of the subjects in this study was deemed to be alcoholic, given their young age profile.
Chronic anemia can impair cardiac function, causing increased cardiac output due to myocardial hypofusion. 31 Cardiac enlargement is a common observation in children with sickle cell disease, 17 and has been found to be related to the severity of anemia and percentage hemoglobin S. 17 Furthermore, children who receive very frequent transfusions are exposed to the cardiac toxicity of iron overload. 31 All such cardiac complications were ruled out in our patients, and thus we concur with the suggestion of McMahon and Mark 18 that chronic heart failure and myocardial infarction are uncommon in sickle cell disease.
To address the shortcoming of one-time determination in a cross-sectional study, we followed up on the determinations in 16 subjects predominantly of the SS genotype. The trend of changes in all the parameters for the two determinations was similar to those obtained for the cross-sectional study.
Conclusion and Recommendations
This study has shown that, in patients with sickle cell disease and a hemolytic tendency attributable to mutant hemoglobin S in red cells, there is generally higher elevation of AST relative to ALT, leading to an AST:ALT ratio >1. This finding is at variance with the generally held view that, in patients with acute and chronic liver disease of various origins, the AST:ALT ratio provides useful clinical information regarding both the cause and severity of liver disease. We therefore propose use of the AST:ALT ratio in sickle cell disease (provided that hepatic and cardiac integrity has not been unduly compromised) as a hemolytic index, and using simple and multiple regression analyses, we have shown the ratio to have an inverse association with hemoglobin, but also a direct association with reticulocytes and lactate dehydrogenase, which are known markers of hemolysis. It is recommended that the correlations between the ratio and total, direct, and indirect bilirubin should be found, while further subjecting the data to receiver-operator curve analysis to determine the specificity and sensitivity of the AST:ALT ratio as a hemolytic index.
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.
Footnotes
Acknowledgments
The authors are grateful to the Research and Conferences Committee of KNUST for financial support for this study. Our appreciation also goes to Mr CK Firempong and the technical team at the Clinical Analyses Laboratory of the Department of Biochemistry and Biotechnology for their assistance in the biochemical analyses. For the hematological analyses, we are thankful to Mr BA Eshun and his coworkers at the Department of Hematology, Komfo Anokye Teaching Hospital, Kumasi.