
Abstract

Hemoglobinopathies are the most common genetically inherited single-gene disorders in the world. 1 Their associated negative economic impact affects mainly poorer countries. 2 According to the World Health Organization, about 5.2% of the world population and over 7% of pregnant women carry a significant variant, and 1.1% of couples worldwide are at risk for having children with a hemoglobin disorder. 3 Sickle cell trait or the hemoglobin S variant, which is the heterozygous state for the sickle hemoglobin beta globin gene, is carried by as many as 100 million individuals worldwide. 4
Hemoglobinopathies are frequently linked to artifactually altered hemoglobin A1c (HbA1c) concentrations. 5 In blacks with prediabetes, the presence of the hemoglobin S variant is associated with a higher HbA1c concentration and this elevation is not an artifact. 6 Blacks compared to non-Hispanic whites (nHws) tend to have a higher HbA1c concentration for the same degree of glycemia as measured by glycated serum proteins (known as fructosamine) or blood glucose. 7 This discordance is known as the glycation gap. 8 The glycation gap is a measure of disagreement between the magnitude of integrated glycation of (1) hemoglobin within red blood cells (RBC) and (2) circulating proteins within plasma. This discordance can result from alterations in glycation occurring either in the RBC/hemoglobin compartment or the plasma protein compartment. 9 Racial discordances between HbA1c concentrations and other measures of glycemic control are unexplained. 10 Identifying genes underlying racial differences in hemoglobin glycation would add credence that the differences are real and that genetic strategies may be useful for determining proper treatment based on the level of mean glycemia suggested by HbA1c values. 11 The hemoglobin S variant hemoglobinopathy occurs more frequently in blacks then in nHws. 12 It is the thesis of this editorial article that the higher prevalence of the hemoglobin S hemoglobinopathy variant in the black population than in the nHw population is associated with or contributes to the glycation gap in blacks.
Hemoglobin A1c
HbA1c is the most widely used analyte for measuring mean glycemic control. HbA1c is a measure of the percentage of hemoglobin molecules attached with glucose. The higher the glucose concentrations over the previous 2-3 months, the higher HbA1c will be. 13 An HbA1c test is used to monitor the average glucose concentrations of patients diagnosed with diabetes and when elevated, to diagnose diabetes. 14
Hemoglobinopathies
The term “hemoglobinopathy” includes all genetic hemoglobin disorders. There are two main types of hemoglobinopathies: (1) thalassemia syndromes and (2) structural hemoglobin variants (abnormal hemoglobins). Both are caused by mutations and/or deletions in the α- or β-globin genes. When a gene defect causes a disorder in hemoglobin synthesis with normal hemoglobin structure, this leads to thalassemia. When a gene defect causes a change in hemoglobin structure, this leads to an abnormal hemoglobin variant.15,16 Some hemoglobin variants are associated with clinical diseases such as sickle cell anemia and related sickling disorders, 17 hemolysis due to unstable hemoglobins, 18 and hemoglobins with increased or decreased oxygen affinity. 19 However, most structural variants of hemoglobin are clinically silent and are only discovered incidentally, often during the measurement of HbA1c in patients with diabetes. 16 According to a CDC survey published in 2014, in the United States the incidence of sickle cell trait per 1000 newborns is 15.5 overall, 73.1 among blacks, and 3.0 among nHws. 12 According to Washington State Health Care Provider Hemoglobinopathy Fact Sheet, about one in ten people of African descent have the sickle cell trait. 20 Prevalences of the hemoglobin S variant as high as 20% to 40% have been described in certain African tribes. 21 Hemoglobin variants including hemoglobin C, hemoglobin S, hemoglobin E, and hemoglobin D traits, as well as elevated fetal hemoglobin are the most common hemoglobin variants that may interfere with HbA1c measurements. 22
Laboratories use many different methods for measuring HbA1c based on charge or structure and some of these methods can give inaccurate results if patients have certain hemoglobinopathies because by using methods that separate by migration based on molecular charge, a hemoglobin variant molecule can migrate similarly to HbA1c and create a falsely elevated or depressed reading. 23 A clinician should be suspicious that an A1c result is inaccurate due to the presence of a hemoglobinopathy interfering with the HbA1c assay if (1) the HbA1c value is much higher or much lower than expected; (2) the HbA1c value is over 15%; (3) the HbA1c value does not correlate with self-monitored blood glucose results; or (4) a patient’s HbA1c result is radically different from a previous HbA1c result following a change in laboratory HbA1c methods. 24 When such suspicion is present, then the patient’s sample should be tested for HbA1c with a method that is known not to have interference from the most common hemoglobin variants. 25 A falsely high or low HbA1c reading can lead to overtreatment or undertreatment of diabetes. 11
Racial Differences in Hemoglobin A1c
The HbA1c concentration might fail to reflect mean glycemia in two circumstances related to genetics. The first is a genetically determined hemoglobinopathy, as described above. This situation produces an artifact whereby the hemoglobin variant is being measured instead of or in addition to HbA1c. 5 The second situation is a racial effect that can result in the HbA1c concentration being truly higher in people of some races than other races. 26 Blacks and populations of Middle-East ancestry, compared to nHws have been shown on average to have higher HbA1c values, even after adjustment for factors likely to affect glycemia, although there are much wider differences within races than between races.9,27,28 In a study of 3189 individuals with impaired glucose tolerance, from five racial and ethnic groups who were eligible for the Diabetes Prevention Program (DPP), but who did not have type 2 diabetes, 29 after adjustment for factors that differed among groups or might affect glycemia (ie, age, gender, education, marital status, blood pressure, adiposity, hematocrit, fasting and postglucose load glucose concentrations, glucose area under the curve, beta-cell function, and insulin resistance) racial differences in HbA1c persisted. Postadjustment mean HbA1c values were 5.78% for nHws, 5.93% for Hispanics, 6.00% for Asians, 6.12% for American Indians, and 6.18% for blacks (P < .001). The authors concluded that among patients with impaired glucose tolerance, “HbA1c may not be valid for assessing and comparing glycemic control across racial and ethnic groups or as an indicator of health care disparities.” 30
A similar conclusion about the lack of validity of HbA1c as a sole determining factor of mean glycemia when comparing racial/ethnic groups was supported by a study that used continuous glucose monitoring data. In 2017, using continuous glucose monitoring to assess mean glycemia, Bergenstal and colleagues found blacks with type 1 diabetes to have HbA1c values that were on average, 0.4% HbA1c units higher than those of whites at any given average glucose concentration. 9 This reason for this difference between the two groups has not been elucidated. 30 A difference in glycation or in RBC lifespan between the races has been suggested.11,31
Genetic Differences and Hemoglobinopathies in HBA1C
One of the largest studies to understand genetic factors in responsible for a difference in HbA1c values between races was published in February 2019 by Hivert and colleagues. This study assessed three types of genetic markers to explain racial differences in HbA1c values between blacks and nHws. The genetic markers included (1) genetic variants causing hemoglobinopathies and erythrocyte disorders; (2) genetic variants associated with HbA1c discovered in a recent genome wide association study of loci affecting HbA1c or erythrocyte biology; 32 and (3) principal component analysis of factors intended to determine whether individuals in a dataset are descended from a homogenous population or from a population containing genetically distinct subgroups. These types of genetic studies were performed on 2658 participants in the Diabetes Prevention Program (DPP) all of whom had prediabetes but not type 2 diabetes.28,33
The group of self-identified black participants in this study (n = 537), compared to the group of self-identified nHws (n = 1476) had a higher mean HbA1c value by 0.4% HbA1c units, despite comparable fasting and 2-hour postprandial glucose concentrations. The first principal component explained 60% of the difference in these HbA1c values, which confirmed an association of higher HbA1c with African descent, but the study was not able to determine a cause for the association, such as genetic, environmental, behavioral, or socioeconomic factors.
The genetic risk score based on the genome wide association meta-analysis explained 14% of the difference. The investigators cautioned, however, that the set of 60 loci from their genome risk score might be incomplete because the genome wide association study from which they were derived identified only two loci specific for people of African descent.
The presence of a hemoglobinopathy, as long as it was the sickle cell variant hemoglobinopathy (having one normal gene and one sickle gene), explained 16% of the difference in HbA1c between blacks and nHws. The investigators studied seven genes associated with hemoglobinopathies and found that in blacks the sickle cell variant was associated with a higher HbA1c value by 0.44% HbA1c units. The association was essentially the same after adjustment for fasting glucose, BMI, and waist circumference. Five variants of hemoglobin F were associated with lower HbA1c values in blacks of a magnitude of less than 0.1% HbA1c units. Six genetic variants for enzymes associated with RBC biology were studied and one of them, the G6PD variant, was associated with lower HbA1c by 0.6% HbA1c units, but the other variants had a minimal effect on a difference in HbA1c values between the two racial groups.
Sickle Cell Trait Hemoglobinopathy and Differences in HbA1c
It has not been settled as to whether the presence of sickle trait hemoglobinopathy affects mean HbA1c values. This relationship has been assessed in six studies. (1) The aforementioned Hivert study found higher mean HbA1c values in prediabetic subjects with sickle cell trait compared to without the sickle cell trait (delta 0.44%, P = 2.1 x 10−8), 33 and so did the (2) Senegal study (delta 0.51%, with no P value presented) which assessed a group of 203 subjects, over half of whom did not have diabetes. 34 Both studies were published in February 2019. (3) In 2017 the combined Coronary Artery Risk Development in Young Adults study and the Jackson Heart Study demonstrated lower mean HbA1c values in subjects with the sickle cell trait (delta −0.38%, P < .001). Diabetes was not an entry criterion in this analysis and mean HbA1c concentrations in subjects in this study were 5.7-6.0%. 35 (4) The Africans in America Study in 2015, where a history of diabetes was an exclusion factor, did not report a significant mean difference between subjects with and without the sickle trait, but the HbA1c values in subjects with sickle cell trait, compared to the HbA1c values in subjects without this trait, were about 10% less sensitive and 10% more specific in making a diagnosis, suggesting that the values were approximately 10% higher in the hemoglobinopathy subjects. 36 In two older retrospective studies HbA1c results were compared between blacks with and without the sickle cell trait and the studies found less of an association of higher HbA1c in the presence of sickle cell trait compared to the absence of sickle cell trait, compared to the two studies reported this year. (5) In 2010 the HbA1c value was higher in the presence of the trait (delta 0.2%, P = .06) in a community population where diabetes was neither an inclusion nor an exclusion factor. 37 (6) In 2012 the mean HbA1c was lower in a type 2 diabetes cohort among subjects with compared to without the sickle cell variant (delta −0.4%, 95% CI = 1.18-0.93). 38 In this study, HbA1c was measured by ion exchange chromatography, a method that is known for generating falsely decreased levels for glycated hemoglobins in patients with the hemoglobin S variant. 39 The combination of findings in these six studies suggests that in type 2 diabetes elevated HbA1c concentrations out of proportion to mean glycemia, in blacks compared to nHws, could be associated with the presence of the sickle cell hemoglobinopathy variant.
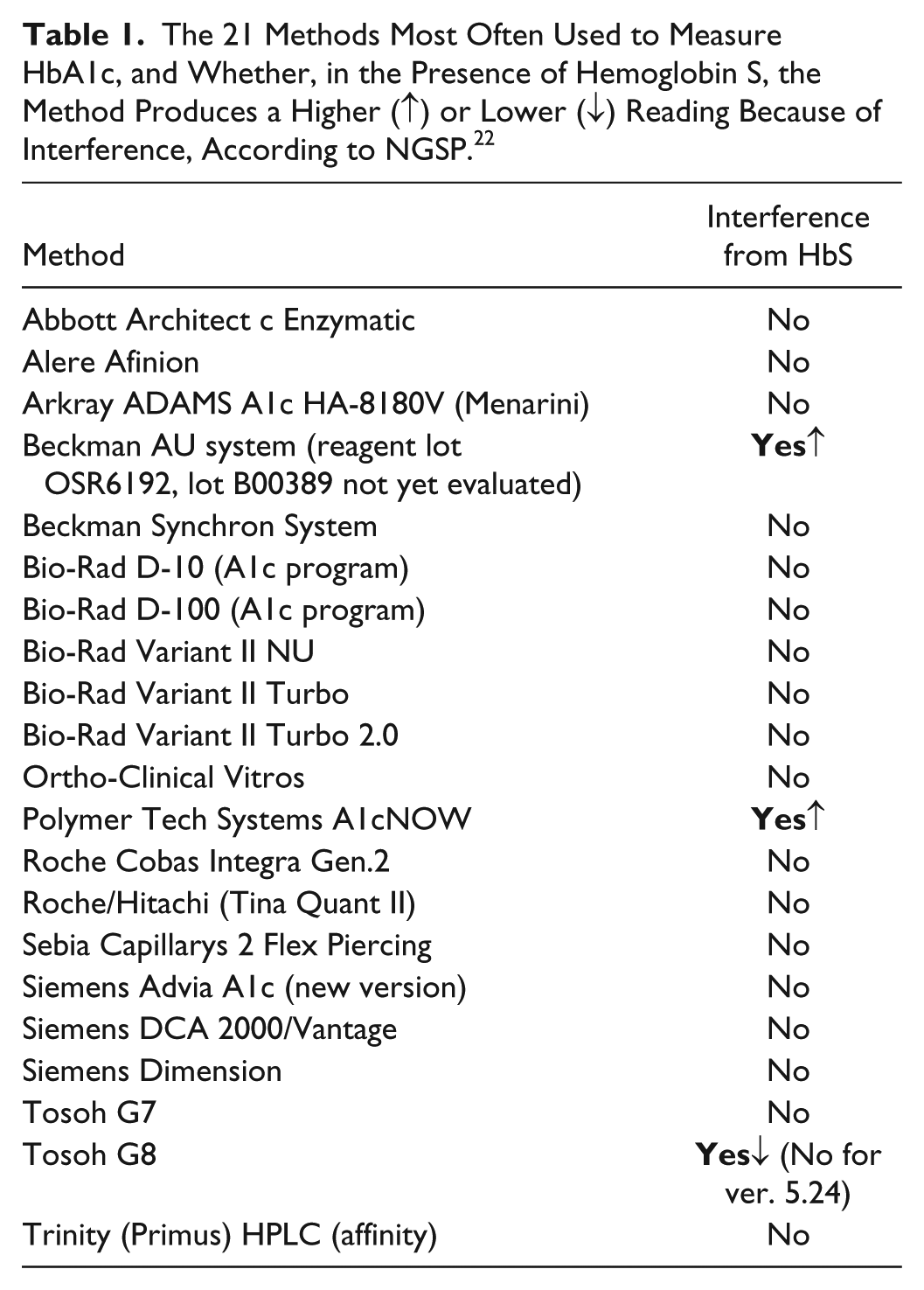
There has been debate as to whether the HbA1c differences in these sickle trait studies were due to interference with the measuring assays.33,40,41 NGSP is an organization that standardizes HbA1c test results to those of the Diabetes Control and Complications Trial (DCCT) and United Kingdom Prospective Diabetes Study (UKPDS), which established the direct relationships between HbA1c value and outcome risks in patients with diabetes. 42 NGSP sets accuracy requirements. A list of the 21 most widely used HbA1c assays and whether they are susceptible to interference from hemoglobin S, which is present with sickle cell trait, is found in Table 1. 22
The 21 Methods Most Often Used to Measure HbA1c, and Whether, in the Presence of Hemoglobin S, the Method Produces a Higher (↑) or Lower (↓) Reading Because of Interference, According to NGSP. 22
Future Hemoglobinopathy Research
The data comparing HbA1c values in blacks with and without the hemoglobin S variant has been collected mainly in prediabetic and type 1 populations, but no study has looked at this phenomenon in patients with type 2 diabetes subjects with an NGSP-approved accurate method for measuring HbA1c in the presence of this variant. This editorial article has presented evidence supporting the hypothesis that the hemoglobin S hemoglobinopathy variant is associated with or contributes to the presence of a glycation gap between glycated hemoglobin in RBCs and glycated serum proteins in blacks (compared to nHws) with type 2 diabetes.
This hypothesis can be tested by performing a well-controlled prospective trial in blacks with type 2 diabetes and nHws with type 2 diabetes comparing results of (1) mean glucose concentrations and time in range using continuous glucose monitoring; 43 (2) accurate HbA1c measurements not affected by sickle cell trait by averaging HbA1c results from two different NGSP–approved instruments for measuring Hb A1c that are not affected by artifactual interference from hemoglobin S; 22 and (3) both hemoglobin electrophoresis and high performance liquid chromatography to check for the presence of hemoglobin S. 44 This study will establish (1) to what extent blacks have a glycation gap relative to nHws in type 2 diabetes, that is, whether the black and nHw populations with type 2 diabetes have similar or dissimilar glycemic control for a given mean glucose concentration and time in range, and glycosylated serum protein concentration; and (2) whether the level of mean glycemic control in the black cohort, as measured by either continuous glucose monitoring or HbA1c, is associated with the presence of hemoglobin S. In the black population, if the presence of the hemoglobin S variant is associated with a gap between predicted mean glycemia (as measured by continuous glucose monitoring) and HbA1c concentrations, then this difference will represent a glycation gap linked to the presence of the hemoglobin S variant hemoglobinopathy. In that case, it will be demonstrated that the presence of the hemoglobin S variant is associated with HbA1c concentrations in type 2 diabetes not only potentially as an artifact, but actually as a physiologic phenomenon.
The use of continuous glucose monitoring to assess glycemia in a study of the glycation gap in patients with type 2 diabetes has not been reported in the medical literature. Likewise there are no reports in the medical literature of a study correlating the presence of the hemoglobin S variant with double-checked accurate (in the presence of the hemoglobin S variant) measures of HbA1c concentrations and double-checked assays for the presence of this variant. It is now time to test the hypothesis linking the presence of a hemoglobinopathy with heretofore-unexplained elevations of HbA1c concentrations out of proportion to continuously measured glucose and other metrics of mean glycemia in patients with type 2 diabetes.
Footnotes
Acknowledgements
The author thanks Robert Cohen, MD, and Sultan Meo, MBBS, MPhil, PhD, for helpful advice and Annamarie Sucher for her expert editorial assistance.
Abbreviations
DCCT, Diabetes Control and Complications Trial; DPP, Diabetes Prevention Program; HbA1c, hemoglobin A1c; nHws, non-Hispanic whites; UKPDS, United Kingdom Prospective Diabetes Study.
Declaration of Conflicting Interests
The author declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DCK is a consultant for Abbott, Ascensia, EOFlow, Lifecare, Merck, Novo, Roche Diagnostics, and Voluntis.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.