
Abstract
There are no studies regarding analysis of clinical and haematological features of chronic myelogenous leukemia (CML) from Pakistan. This study analyzes the data of patients suffering from CML, reporting to a major referral Institute in Northern Pakistan in the past 6 years and 3 months. CML constitutes approximately 80% of all myeloproliferative disorders, with a peak incidence between 21-50 years of age, and a male:female ratio of 2:1. Anaemia and massive splenomegaly were the main clinical features found in 92% and 47% patients respectively. There was significant correlation between anaemia and WBC counts with degree of splenomegaly. Three percent of all CML patients presented as de novo accelerated phase, and another 3% presented as blast crises without any previous history of chronic phase. The ratio of myeloid and lymphoid blast crisis was 2:1. Median duration of chronic phase in patients on hydroxyurea treatment was 6 years. Thirty six percent of patients in chronic phase of CML belonged to intermediate and high risk according to Sokal and Hasford scoring systems. In contrast to the Caucasian populations where the peak incidence of the disease is in 6th to 7th decade, CML occurs in Pakistan in a much younger population, with a broad peak between 21-50 years of age. Patients present in fairly advanced disease because of poor access to health care facilities, due to non-affordability and lack of health insurance coverage.
Keywords
Introduction
Chronic myelogenous leukemia (CML) is a myeloproliferative disorder, characterized by clonal expansion of abnormal pluripotent haemopoietic stem cell, arising from reciprocal translocation of genetic material between long arms of chromosome 9 and 22. 1 The resulting BCR-ABL fusion gene is derived from translocation of abl gene on chromosome 9, which becomes juxtaposed to bcr gene 2 on chromosome 22. The BCR-ABL oncogene results in constitutive expression of an oncoprotein (p210) with tyrosine kinase activity, 3 which causes activation of anti-apoptotic pathways and unregulated proliferation of stem cells resulting in expansion of myeloid cell mass. The disease undergoes clonal evolution from relatively stable chronic phase to an accelerated phase lasting for 4-6 months, and finally culminating into myeloid or lymphoid blast crisis. 4
The age adjusted incidence rate of CML for both sexes in United States 5 is 1.6 per 100,000. Before the advent of tyrosine kinase inhibitors, the chronic phase of the disease lasted from 3-8 years 6 in patients who were treated with hydroxyurea or busulphan. Different aspects of CML, including presentation at diagnosis, biology, clinical and laboratory features, risk stratification and, course of, the disease have been studied in various populations.7,8 This has resulted in fair emergence of accurate and well-defined picture of disease in those communities facilitating optimum therapeutic decisions. There is, however, a lack of comprehensive analysis of any such data pertaining to this haematological malignancy in Pakistan. In this paper retrospective analysis is done on epidemiological, clinical, and laboratory data of Pakistani patients suffering from chronic myelogenous leukemia, who had reported to a single centre for initial diagnosis and workup of disease during the past 6 years and 3 months.
Materials and Methods
The study was carried out in Armed Forces Institute of Pathology, Rawalpindi, Pakistan, which is the major referral centre for diagnosis of patients suffering from haematological disorders in Northern Pakistan. Patients who were diagnosed to be suffering from CML between 1st January, 2006 and 31st March, 2012 were selected for data analysis. The diagnosis of CML was confirmed either by cytogenetic analysis for Philadelphia chromosome or RT-PCR based BCR-ABL analysis (Applied Biosystems 7500 Real time PCR system). 9 Diagnosis of accelerated phase of CML was based on one or more of the following criteria:10,11 (1) rising white cell count and/or splenomegaly despite chemotherapy, (2) thrombocytosis > 1000 x 109/L despite treatment, (3) persistent thrombocytopenia not related to chemotherapy, (4) > 20% basophils in peripheral blood, (5) 10%-19% blasts in blood or bone marrow, and (6) bone marrow fibrosis with presence of megakaryocyte clusters. Blast crisis was diagnosed when there were >20% blasts in the bone marrow. Myeloid and lymphoid blast crises were distinguished from each other by morphology of blast cells, staining by Sudan Black-B and immunophenotyping (BD FACS-Calibur). The relative risk of patients in chronic phase of CML was determined by using both Sokal and Hasford prognostic scoring systems, using European LeukemiaNet calculator. 12 Patients in this study were stratified into age groups with 10 years increments. The ratio of the sum of accelerated phase and blast crises (advanced disease) with the chronic phase was calculated in each age category as follows: Number of patients in accelerated phase + Blast crises/Number of patients in chronic phase. All patients diagnosed from this Institute were later managed in the referral centers, which had sent them in for diagnosis. Ethics and Scientific committees of the Institute approved the study.
Statistical Analysis
Statistical analysis of the data was done using IBM SPSS Statistics Version 20. Continuous variables haemoglobin, WBC counts, and platelet counts were presented as range and median values. Frequencies were calculated using Microsoft excel sheet. Pearson's correlation was calculated for testing the correlation between spleen size and WBC counts, haemoglobin, and platelet counts. Chi-square test was applied to test the association of haemoglobin level and platelet counts with different phases of CML. Chi-square test was also applied to test the association of ratio of number of patients in accelerated phase and blast crises with those in chronic phase of CML in different age categories. Unpaired t-test was applied to compare the mean basophil counts between myeloid and lymphoid blast crises of CML. The P value < 0.05 was considered as statistically significant result.
Results
During the period of study, out of 425 patients suffering from myeloproliferative disorders, 335 (79%) patients were diagnosed as chronic myelogenous leukemia. Majority of patients with CML were in the chronic phase of the disease (n = 240, 71.6%), with 49 (14.6%) in the accelerated phase, 31 (9.3%) in the myeloid blast crisis, and 15 (4.5%) suffered from lymphoid blast crisis of the disease. Age of the patients ranged from 2-80 years (median: 42 years), with a male to female ratio of 2:1 (225:110). Peak incidence of the disease was seen between 21-50 years (Fig. 1), reflected by a broad plateau. Fourteen patients (5.8%) in chronic phase of CML were asymptomatic and were discovered incidentally after routine blood tests were performed for other reasons. The duration of symptomatic disease ranged from one week to 3 years, with maximum number of patients (n = 225; 67%) reporting within 3 months of the onset of symptoms. The spectrum and frequency of clinical features seen in patients in all phases of CML is given in Table 1. The most common clinical presentations of patients were pallor (63.6%), and signs and symptoms related to splenomegaly (50%). About 18% of patients had symptoms related to hyper-metabolic state, secondary to malignancy.

Frequency of CML patients in different age groups.
Clinical features of CML patients (n: 335).
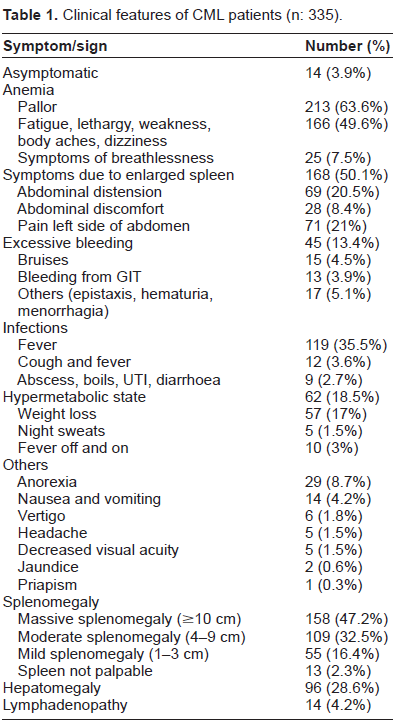
Anaemia was the most frequent finding and was almost universal, as only 27 (8%) patients in all phases of CML had haemoglobin levels > 12 g/dL (Table 2). Consequently, the most common clinical presentation was due to anaemia, including symptoms of fatigue, breathlessness, dizziness, lethargy, and body aches (Table 1). The next frequent clinical feature was massive splenomegaly (spleen palpable > 10 cm below left costal margin), which was observed in 158 (47.2%) patients in this study presenting as abdominal distension, pain in left hypochondrium, and dragging sensation in abdomen. A significant number of patients (>35%) gave history of continuous fever of 5-10 days duration, suggestive of either viral or bacterial infection. Only 14/45 patients who presented with excessive bleeding had thrombocytopenia with platelet count less than 100 x 109/L, suggesting that platelet dysfunction was responsible for impaired haemostasis in the remaining (31/45; 69%) patients. Thrombocytosis was seen in 68 (28%) patients suffering from chronic phase of the disease, at the time of initial diagnosis; and in 88 (26%) patients in all phases of CML. Four patients with thrombocytosis had signs and symptoms of increased bleeding, including bleeding from gut, menorrhagia and haematuria, again indicative of platelet dysfunction.
Distribution of haemoglobin level and platelet counts in different phases of CML.

Note:
P < 0.01.
Patients in chronic phase of CML had WBC count ranging from 21.8-1160 x 109/L (median: 187.3 x 109/L). Out of these, only 10 patients (4.2%) had WBC counts between 21-50 x 109/L, while the majority (63%; n = 151) had WBC counts between 101-300 x 109/L (Fig. 2). The WBC counts in patients suffering from accelerated phase ranged from 1.73 28.7 x 109/L (median: 91.8 x 109/L); between 0.823 64 x 109/L (median: 119 x 109/L) in myeloid blast crisis and 1.4-65 8 x 109/L (median: 91.6 x 109/L) in lymphoid blast crisis. Sixty percent of patients were in the chronic phase of the disease, 81.6% in accelerated phase, 93% in myeloid blast crisis, and 87% in lymphoid blast crisis had hemoglobin ≤ 10 g/dL (Table 2). Patients in myeloid blast crisis had a significantly greater drop of haemoglobin (P < 0.01) between 4-7 g/dL, as compared to those in other phases of the disease. Platelet counts ranged from 65-1744 x 109/L (median: 3 44 x 109/L) in chronic phase of CML, 13-3700 x 109/L (median: 292 x 109/L) in accelerated phase, 5-654 x 109/L (median: 94 x 109/L) in myeloid blast crisis and 4-386 x 109/L (median: 44 x 109/L) in patients with lymphoid blast crisis. A significantly higher number of patients in myeloid and lymphoid blast crisis presented with thrombocytopenia (Table 2) as compared to patients in chronic and accelerated phase of the disease. There was a significant direct correlation between spleen size and WBC count (Pearson correlation: 0.488; P < 0.0001), and inverse correlation between spleen size and hemoglobin levels of patients (Pearson correlation: -0.424; P < 0.001) in chronic phase of the disease. Similarly, WBC counts had significant inverse correlation with hemoglobin levels (Pearson correlation: -0.464; P < 0.001). There was insignificant relation between spleen size and platelet counts of patients.

WBC counts in chronic (n: 240) and accelerated (n: 49) phases; and myeloid blast (n: 31) and lymphoid blast (n: 15) crises of CML patients (n: 335).
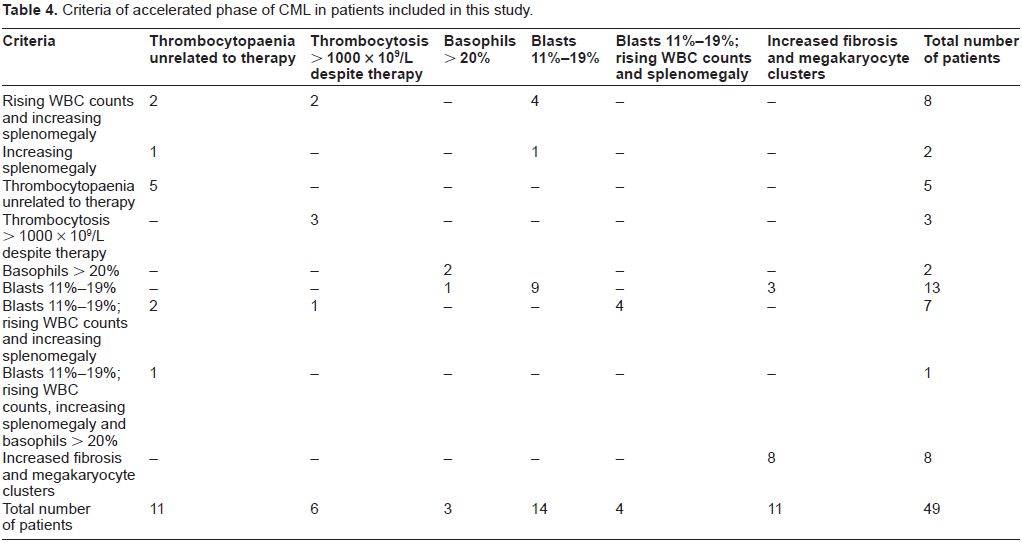
In patients with chronic phase of CML, 177/240 (74%) had LAP scores between 0-13 (Normal: 14-100). In accelerated phase of CML, 25 (51%) patients had LAP scores below 14, 4 (8%) patients had LAP scores above 100 while remaining had LAP score within normal limits. In patients with myeloid blast crisis, 9/29 (31%) had LAP score < 14, whereas 6/15 (40%) patients in lymphoid blast crisis had low LAP score (<14). Percentage of basophils in the peripheral blood film of patients with different phases of CML is given in Table 3. Mean percent of basophils in lymphoid blast crisis was 2.27 ± 4. Percentage of basophils in the peripheral blood film of patients with difference in basophils between myeloid and lymphoid blast crises was not statistically significant, patients with more than 8% basophils were found to transform only in myeloid blast crisis of the disease. The ages of patients in lymphoid and myeloid blast crisis were comparable (P > 0.05). Ten patients in accelerated phase (3% of total CML patients and 21% of patients in accelerated phase) were diagnosed without any prior history of diagnosis or treatment for CML, and were considered to be suffering from de novo disease. The duration of their symptoms ranged from 2 weeks to 12 months (median: 2 months). Seven patients who had transformed into accelerated phase from a previous chronic phase of CML were taking imatinib, for duration ranging from 8 months to 3 years (median: 2 years), whereas 32 patients were on hydroxyurea for period ranging from 3 months to 7 years (median: 3 years). Thus patients on hydroxyurea are at a greater risk of transformation to advanced phase of the disease. Grade II or more fibrosis was seen in 21/49 (43%) patients in accelerated phase, and 50/240 (21%) patients in chronic phase of the disease. The combination of criteria based on which the patients were diagnosed to be suffering from accelerated phase are given in Table 4. Twenty-six patients (53%) in this group were found to have blasts 11%-19%, either as sole criteria of accelerated phase or in combination with other criteria including basophils > 20%, rising WBC counts, increasing fibrosis, thrombocytosis and thrombocytopenia. Increasing fibrosis with presence of megakaryocyte clusters was the sole criteria of accelerated phase in 8 (16.3%) patients.
Percentage of basophils in patients with different phases of CML (n: 335).*

Note:
P > 0.05.
Criteria of accelerated phase of CML in patients included in this study.
Six patients (1.8% of total CML patients) suffering from myeloid blast crisis had duration of symptoms of disease ranging from 2 weeks to 8 months (median: 2 months), with no evidence of disease prior to the diagnosis. Similarly, 4 (1.2% of total CML patients) patients presented lymphoid blast crisis without prior history of symptoms or diagnosis. Age of patients in myeloid blast crisis ranged from 28-65 years (median: 48 years), and was comparable to age range of patients suffering from lymphoid blast crisis was between 16-62 years (median: 45 years). The duration of chronic phase of the disease in patients with myeloid blast crisis, who were previously diagnosed (23/31 patients), ranged from 9 months to 14 years (median: 6 years), and 1-7 years (median 6 years) in those who later developed lymphoid blast crisis (9/15 patients). Only 3 (6.5%) patients suffering from myeloid and lymphoid blast crises were taking imatinib during the chronic phase, while the remaining patients (93.5%) were on hydroxyurea treatment.
Although there was a gradual increase in proportion of patients in advanced disease in comparison with those in chronic phase, from 0.23 at ages between 11-20 years to 0.67 at age range of 61-70 years, the difference was not statistically significant (P = 0.353). The median duration between development of accelerated phase (3 years) and blast crises (6 years) from chronic phase of the disease was also constant across all age groups. There was significantly higher number of patients suffering from intermediate and high-risk disease in the 41-80 years age group, as compared to patients between 2-40 years of age (Table 5), according to Sokal and Hasford scoring systems (P < 0.001).
Risk stratification of patients suffering from chronic phase of CML according to age groups.

Note:
P < 0.001.
Discussion
CML constitutes the most common myeloproliferative disorder in Pakistan. However, there is a unique age distribution of the disease in this region, in that the peak incidence of the disease plateaus between 21-50 years followed by continuous declining trend to the age of 80 years. In this study, 27% of patients were between the ages of 20-34 years. This is in contrast to data from the USA, 5 where the peak incidence of disease occurs between the ages of 75-84 years (22% of patients), while only 7.7% of patients suffering from CML are between the ages of 20-34 years and 9.5% between age ranges of 35-44 years. The data from the UK 13 also shows peak incidence of CML occurring between 65-84 years of age. Rising incidence of CML with increasing age has been linked to slow rate of expansion of Philadelphia clone, 14 which consists of three waiting times-time to develop the t(9;22) mutation, time required for expansion of malignant clone, and time when the malignant clone becomes detectable by laboratory methods. In contrast to the afore-mentioned one mutation model, several genetic polymorphisms may affect the risk of development of CML in the background of Philadelphia chromosome as the primary abnormality. This multistep model of development of CML is consistent with increased rate of somatic mutations with increasing age. Polymorphisms in p53 codon 72, single nucleotide polymorphism in FLT3 gene and NQO1 C609T polymorphism are linked with increased risk of development of overt CML.15–17 The fact that the incidence of CML in Pakistan peaks at ages between 21-30 year and remains so till 50 years, with a sharp decline beyond 60 years is intriguing. This, however, can be partly explained by the demographics of the country, 18 according to which 35.4% of the population of Pakistan consists of individuals from 0-14 years of age, whereas only 4.2% people are more than 65 years. This is in contrast to situation in the USA and UK 18 where 17%-20% of population comprises of individuals who are 0-14 years old, and 13%-16.5% of people are more than 65 years of age. Thus the age distribution pattern of CML in Pakistan may partly be due to greater number of younger individuals and a much smaller population of people beyond 60 years.
As shown in this study, males are affected more commonly (M:F ratio: 2:1) with the disease. This could be related to greater exposure of males to environmental or occupational hazards. Studies in the Caucasian patients 19 suffering from CML have, however, shown only slight preponderance of males (M:F ratio: 1.3:1). Amongst the patients of chronic phase of CML who were diagnosed incidentally (n = 14; <6%) on routine blood counts, 10 had WBC counts ranging from 136-231 x 109/L. The patients did not notice any symptoms, even though they had splenomegaly ranging from 2-8 cm. This is contrary to an earlier study 20 in which much greater percentage (20%) of patients were diagnosed incidentally as suffering from chronic phase of the disease, based on routine blood tests or investigation of splenomegaly discovered during routine check up. The lack of early diagnosis as apparent in our study is related to limited access of medical facilities in Pakistan due to non-affordability and lack of health insurance. We also observed that 6% (n = 20) patients had accelerated phase and myeloid/lymphoid blast crises of CML at the time of diagnosis. It is possible that these patients may either be suffering from an aggressive disease or that they may have failed to notice any symptoms during the chronic phase. It is known that patients may present in advanced stage of the disease as a de novo presentation.21,22
The most frequent presentation of chronic myeloid leukemia in Pakistan, apparent from this study is history of illness of less than 6 months duration, anaemia and massive splenomegaly with WBC counts more than 100 x 109/L. This is similar to the observation by others, 7 who found massive splenomegaly in more than 40% of patients suffering from CML. If, however, all patients who had mild, moderate and massive splenomegaly were included, then most patients (>97%) in this study had splenomegaly, with only 13 (2.3%) patients not having palpable spleens. This is higher than the rate of splenomegaly observed in 40%-60% patients of CML in the USA, 23 and 70%-79% patients in the UK. 7 Similarly, almost one third of patients in this study had hepatomegaly, while this finding was seen in only 2% of patients as reported earlier. 7 Our patients have a greater tumor burden at the time of diagnosis, with one fifth of them presenting with symptoms of hyper-metabolic state.
More than 70% of patients who presented with excessive bleeding had normal platelet count or thrombocytosis, suggesting that platelet dysfunction was the cause of increased tendency to bleed in these patients. Platelet function defects in chronic myeloid leukemia have been reported by others,7,24 and are usually not associated with life threatening haemorrhage.
When data from patients suffering from blast crises was analyzed, it was interesting to note that those who had more than 8% basophils in peripheral blood were found to be suffering exclusively from myeloid blast transformation. It has been reported earlier 25 that patients of CML who present as peripheral blood basophilia (>10%) and myeloid blast crisis have isochromosome 17q [i(q17)] mutation. Since it was a retrospective study, it was not possible to do cytogenetic studies in our patients presenting with blast crisis.
It is possible that patients in our study who had marked basophilia (>10%), and developed myeloid blast crisis may have acquired i(17q) abnormality. It has been noted by others that lymphoid blast crisis of CML is associated with lower peripheral basophil counts as compared to myeloid blast crisis.26–28
According to the Sokal scoring system, 36% of patients belonged to the intermediate or high-risk groups. In Pakistan, most of the patients cannot afford imatinib or second-generation tyrosine kinase inhibitors because of poor socio-economic status and lack of entitlement to health care. These drugs are available to eligible patients, free of cost, in three major oncology centers in the country through the GIPAP (Glivec International Patient Assistance Programme). We are not aware of the number of patients in the chronic phase who were diagnosed by this centre and subsequently registered with the GIPAP as patients generally come only for initial diagnosis and then were managed elsewhere. Although Pakistan is one of the major beneficiaries of the GIPAP assistance, 29 accounting for 8% of patients registered in 15 countries, the ratio of patients registered for free access to imatinib/second generation tyrosine kinase inhibitors and those taking hydroxyurea is not known. It has been shown that patients of CML in Pakistan with low Sokal scores had superior major cytogenetic responses (70.3%) to imatinib, 30 compared with 56% response rate in patients with intermediate Sokal score, and 43.8% response in patients with high Sokal scores. According to the findings of this study, 36% of patients with intermediate and high Sokal scores are potential candidates for second line tyrosine kinase inhibitors including nilotinib/dasatinib or bone marrow transplantation. A central CML registry needs to be established, and the patients should only be eligible for the GIPAP if they are entered into that registry. This will help to prepare national guidelines for optimum management of patients in this part of the world.
Authors’ Contributions
FAB conceived the study, compiled the patients’ data in Microsoft Excel Sheet, analyzed it with statistical methods, and wrote the article. He is also working as Consultant Haematologist and is responsible for final diagnosis when he is on weekly duty roster. SA is HOD of the department, and is responsible to review problem cases referred by Consultants and finalize the diagnosis. He has also reviewed the article and gave useful advice. NA is working as Consultant Haematologist and is responsible for making final diagnosis of cases referred to him during his weekly rotation as Consultant.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.
Footnotes
Acknowledgements
We are grateful to Mr. Intisar Siddiqui for providing help in doing statistical analysis of the data.