
Abstract
Background
Tumor necrosis factor (TNF)-α and -β are cytokines with a wide range of inflammatory, apoptotic and immunomodulatory activities. TNF-α promoter –308 G < A polymorphism has been reported to be associated with rheumatoid arthritis (RA) with inconsistent results.
Objective
The aim of this study is to elucidate a possible association of TNF-α (G–308A) and TNF-β (A+252G) polymorphisms with the susceptibility of RA in Saudi patients.
Patients and Methods
This case control study consisted of 232 Saudi subjects including 106 RA patients and 126 matched controls. Genomic DNA was extracted using QIAampR DNA mini kit (Qiagen CA, USA). TNF-α and TNF-β genes were amplified using Arms primers.
Results
The frequencies of TNF-α (–308) allele G and genotype GG were significantly higher in RA patients as compared to controls while allele A and genotype AA were predominant in control group. On the other hand the frequency of TNF-β (+252) GG and AA genotypes were significantly higher in RA patients as compared to controls while GA genotype was predominant in controls. It was inferred that genotype GG positive individuals at position –308 of TNF-α were susceptible to RA while genotype AA might has a protective effect on RA susceptibility in Saudis. Whereas GG and AA genotype of TNF-β at +252 position might exert additive susceptibility to RA and GA might be refractory. However, there was no significant association between duration of morning stiffness, RF positivity and number of joints involved and distribution of alleles/genotypes of TNF-α (–308) or TNF-β (+252) polymorphism. It may be concluded that the TNF-α (–308) and TNF-β (+252) polymorphisms might influence the susceptibility to RA in Saudi population. These results might have prognostic value for future clinical observations.
Introduction
Rheumatoid arthritis (RA) is a chronic inflammatory autoimmune disease affecting 0.5 to 2% of the world's population. Abundant expression of pro- and anti-inflammatory cytokines observed in the affected tissues and serum of RA patients clearly indicates the involvement of cytokines in the etiopathology of RA. 1 Tumor necrosis factor (TNF), a pro-inflammatory cytokine has been shown to play a pivotal role in the pathogenesis of several autoimmune diseases including RA.1–3 This is further evident from significantly high levels of TNF in the synovial fluid of RA patients.
TNF-α and TNF-β are closely related cytokines that share 30% amino acid residues and use the same cell surface receptor. 4 Nedwin et al 5 reported that the TNF-α and TNF-β genes are located in tandem on chromosome 6 between the Class I and Class II cluster of the major histocompatibility complex (chromosome 6p21.1–6p21.3). Among the five polymorphisms (at position +691,–238, –308, –851, and –857) of TNFα gene identified by PCR-SSCP analysis, TNFα –308 polymorphism has been reported to be associated with several autoimmune diseases including RA.6,7 The genetic variation on position –308 results in two allelic forms in which the presence of guanine (G) defines the common variant and the presence of adenine (A) defines the less common one. TNFα-308A-allele displays increased gene transcription as compared to the common allele G. 8 It has been shown to produce 6–7 fold higher levels of TNF-α transcription.8,9
Tumor necrosis factor β (TNF-β) which is closely linked to TNF-α, has also been shown to contribute to the susceptibility of several autoimmune diseases.10,11 A polymorphism has been reported at position +252 within the first intron of the TNF-β gene, consisting of a Guanine (TNF-β +252G) on one allele and an Adenine (TNF-β +252A) on the alternate allele.
12
The presence of G at this position defines the mutant allele known as TNF-β
Overall the data related to allele and genotype distribution of TNF-α and TNF-β polymorphisms in RA patients from various populations is limited and inconclusive. In this study an attempt was made to determine a possible association of TNF-α (G–308A) and TNF-β (A+252G) polymorphism with RA in Saudi population.
Materials and Methods
Patients and Controls
A total of 232 subjects visiting Armed Forces Hospital, Riyadh, Saudi Arabia were recruited (during 2007–2008) for this study. The diagnosis of RA was made according to the revised criteria of American College of Rheumatology. 15 RA group consisted of 106 unrelated Saudi RA patients [male = 21, female = 85, age range 26 to 75 years (mean age 49 ± 12.5 years)]. The control group consisted of 126 matched, unrelated healthy blood donors [male = 50, female = 76, age range 25 to 70 years (mean age 48 ± 11.5 years)] from the same Saudi population.
PCR Amplification
Genomic DNA was extracted from the peripheral blood of RA patients and controls using QIAampR DNA mini kit (Qiagen CA, USA). TNF-α and TNF-β genes were amplified using amplification refractory mutation systems (ARMS)-PCR methodology 16 to detect any polymorphism involved at position –308 of TNF-α and position +252 in Interon1 of TNF-β gene respectively. The set of primers used to amplify target DNA in the promoter region of TNF-α and TNF-β genes are summarized in Table 1. PCR amplification was carried out using Ready to Go PCR Beads (Amersham Biosciences, USA). Reaction consisted of 10 temperature cycles of denaturation for 15 s at 94 °C, annealing for 50 s at 65 °C and extension for 40 s at 72 °C. Then 25 cycles of denaturation for 20 s at 94 °C, annealing for 50 s at 59 °C and extension for 50 s at 72 °C. Final extension was performed at 72 °C for 7 min. A positive control was included in the PCR assay by amplification of the human growth hormone (HGH) gene. The amplified product for various samples were separated on the 1.5% agarose gel, stained with ethidium bromide and photographed.
Showing sets of sense and antisense primers used to amplify the TNF-α and TNF-β to detect polymorphism.

Statistical Analysis
The differences in allele/genotype frequencies between patients and controls were analyzed by the Fisher's exact test. P values less than 0.05 were considered significant. The strength of the association of disease with respect to a particular allele/genotype is expressed by odd ratio interpreted as relative risk (RR) following the Woolf's method as out lined by Schallreuter et al. 17 It was calculated only for those alleles/genotypes which were increased or decreased in arthritis patients as compared to control group. The RR was calculated for all the subjects using the formula given below:

a = number of patients with expression of allele or genotype
b = number of patients without expression of allele or genotype
c = number of controls with expression of allele or genotype
d = number of controls without expression of allele or genotype.
Etiologic Fraction (Ef)
The EF indicates the hypothetical genetic component of the disease. The values >0.0–0.99 are of significance. EF was calculated for positive association only where RR > 1 using the following formula. 18

Preventive Fraction (Pf)
The PF indicates the hypothetical protective effect of one specific allele/genotype for the disease. PF was calculated for negative association only where RR < 1 using the following formula. 18

Values < 1.0 indicate the protective effect of the allele/genotype against the manifestation of disease.
Results
The demographic and clinical characteristics of the RA patients are summarized in Table 2. Based on clinical history the mean duration of disease was found to be 9 ± 4.5 years. Number of joints involved varied from 2 to 22. Depending on the number joints involved RA patients were classified into two groups: polyarthritis patients (87.74%) with more than 5 joints involved and oligoarthritis (12.26%) with less than 5 joints involved. Morning stiffness duration varied from 10 minutes in mildly affected to several hour in severely affected patients. Number of swollen and tender joints ranged from 0 to 22. Serological results indicated that 82 (77.36%) patients were rheumatoid factor (RF) positive while 24 (22.64%) RF negative.
Demographic and clinical characteristics of RA patients.

The genotypes and alleles frequencies of TNF-α –308 promoter polymorphism in RA patients and control individuals are presented in Table 3. The frequency of allele-A was significantly lower in RA patients as compared to control group (P = 0.005, RR = 0.48, PF = 0.242) on the other hand the frequency of allele-G was higher in RA patients as compared to the controls (P = 0.005, RR = 1.87, and EF = 0.242). The homozygous GG genotype was present in 64.15% of the RA patients and 50% of controls (P = 0.033), while heterozygous GA was found in 33.01% of RA patients against 38.09% of controls (P = 0.492). The homozygous AA genotype was found in 2.83% of RA patients and 11.90% of control samples (P = 0.012). Allele-A containing genotypes (GA and AA) were present in 35.84% of patients and 50% of the healthy controls (P = 0.033). Susceptibility to RA was significant for homozygote for TNF-α 308 G-allele (GG) (P = 0.033; RR = 1.789; EP = 0.261). The predominance of GG genotype among the patients group indicated that the GG genotype was associated with the susceptibility to RA while AA has protective effect on the susceptibility to RA as it was more common in control samples (P = 0.012, RR = 0.25, PF = 0.337). G-Allele (1-allele) of TNF-α seems to be susceptible to RA (P = 0.005, RR = 1.87, and EF = 0.242) whereas A-Allele (2-allele) of TNF-α seems to be resistant to RA in Saudis (P = 0.005, RR = 0.48, PF = 0.242).
Genotype and allele frequencies of TNFα (G-308A) polymorphism in RA patients and matched controls.

The distribution of genotypes and alleles frequencies of TNF-α –308 promoter polymorphism in relation to duration of morning stiffness, RF positive or RF negative and type of arthritis (polyarthritis and oligoarthritis) is given in Table 4. There was no significant association between duration of morning stiffness, RF positivity and number of joints involved (polyarthritis/oligoarthritis) and distribution of alleles/genotypes of TNF-α –308 polymorphism.
Genotype and allele frequencies of TNFα (G-308A) polymorphism in RA patients in relation to clinical features.
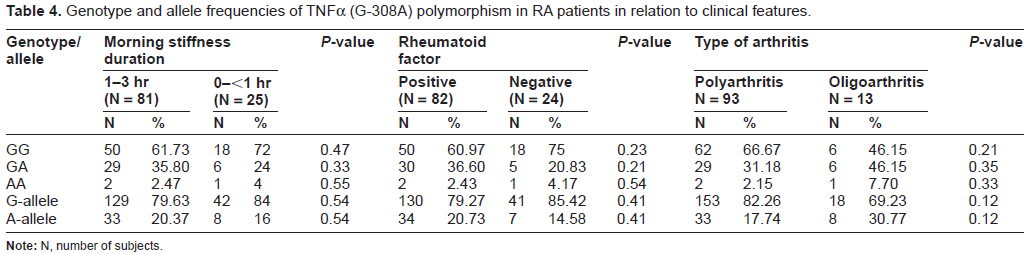
Note: N, number of subjects.
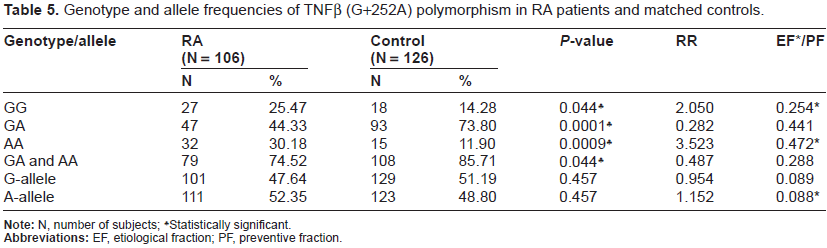
The distributions of genotype and allele frequencies of TNF-β (+252) promoter polymorphism in Saudi patients with RA and controls subjects are summarized in Table 5. The frequency of GG, GA and AA genotypes of TNF–β (+252) showed statistically significant differences between patients and controls. The GG and AA genotypes were significantly over-represented in RA patients as compared to the controls (P = 0.044 and P = 0.0009 respectively) while GA genotype was significantly higher in controls as compared to RA patients (P = 0.0001). These results indicated that GG and AA genotypes at +252 were susceptible to RA (RR = 2.050, EF = 0.254, and RR = 3.523. EF = 0.472 respectively), on the other hand GA was found to be refractory (RR = 0.282, PF = 0.441). Though there were differences in the frequency distribution of allele-A and allele-G of TNF-β (+252) polymorphisms in Saudi RA patients and controls however these differences were not statistically significant (P = 0.457).
Genotype and allele frequencies of TNFβ (G+252A) polymorphism in RA patients and matched controls.
The distribution of genotypes and alleles frequencies of TNF-β (+252) polymorphism in relation to duration of morning stiffness, RF positive or RF negative and polyarthritis/oligoarthritis is given in Table 6. Analysis of data suggested that there was no significant association between duration of morning stiffness, RF positivity and number of joints involved (polyarthritis/oligoarthritis) and alleles/genotypes frequency of TNF-β (+252) polymorphism.
Genotype and allele frequencies of TNFβ (A+252G) polymorphism in RA patients in relation to clinical features.

Note: N, number of subjects.
The comparison between the frequencies of genotypes of TNF-α (G–308A) promoter polymorphism in Saudi healthy population with the frequencies reported for healthy population of various ethnicities worldwide is presented in Table 7. These results clearly indicated ethnic variations in genotype distribution of TNF-α (–308) promoter polymorphism.
Genotype distribution of TNF-α (–308) promoter polymorphism in different healthy groups.

Discussion
This is the first study dealing with the TNF-α and TNF-β polymorphism in Saudi population with RA. Our results showing significantly lower frequency of –308A allele and higher frequency of –308G allele in RA patients as compared to healthy controls are similar to the findings reported in various other ethnic groups including Taiwan Chinese, 19 Japanese, 20 Swedish, 21 Turkish, 22 Hungarian 23 and Han population of Eastern China. 7 This study along with other published reports supported the view that –308 A allele of TNF-α may exert a protective influence for the development of RA. Contrary to our findings the reports from Australian Caucasian, 24 Spanish, 25 Mexicans, 26 American Caucasians 6 and Chilean 27 showed significantly higher frequency of Allele-A in RA patients as compared to control group. On the other hand no significant difference in frequency of Allele-A in controls and RA patient was observed in Taiwanese, 28 Polish, 29 Iranian 30 and Turkish populations. 31 Nemec et al 32 found no significant difference in genotype and allelic frequencies of TNF-α (–308) polymorphism in Czech population with and without RA.
The exact reason for such a vast variation in the distribution of alleles and genotypes of TNF-α (–308) polymorphism in RA patients in different ethnic groups is far from clear. These differences may be attributed to the ethnicity related genetic makeup in different populations which is evident from the genotype data of TNF-α (–308) polymorphism published from various ethnic healthy groups worldwide (Table 7). Lee et al 33 also suggested that ethnicity has a significant impact on the genotype distribution of TNF-α (–308) polymorphism in RA patients. RA is considered to be a complex disorder and its onset and severity is influenced by genetic as well as environmental factors. Hence the gene-environment interaction are likely to play a significant role on the outcome of polymorphism association studies on RA patients.
In this study no significant association was found between the TNF-α (–308) polymorphism and clinical features of RA such as number of joints involved, RF positivity and duration of morning stiffness. Similar to our results Ates et al. 34 also reported no association between TNF-α (–308) polymorphism and RF positivity and erosive disease of RA in Turkish patients. However, the association of the alleles and genotypes of TNF-α (–308) polymorphism has been reported with severity of RA in American, Mexican and Czech populations.6,26,32 Khanna et al 6 found an association between TNF-α (–308) polymorphism and progression of radiographic damage in American patients with early seropositive RA, and suggested that the association might be dependent on genetic variants in linkage disequilibrium with TNF-α (–308) A-allele and DRB1*0301. Rodriguiz-Carreon et al 26 also found an association between TNF-α (–308) A-allele and severity of RA in Mexicans but independent of HLA-DR alleles. On the other hand Nemec et al 32 found no difference in the distribution of genotypes and alleles frequencies between the Czech RA patients and control group. However, on dividing the RA group according to the radio graphical progression of disease they (loc.cit) noticed significant difference in the distribution of genotypes and suggested that GG genotype of TNF-a (–308) polymorphism is associated with the severity of RA in Czech. 32
Our results for TNF-β (+252) promoter polymorphism indicted that GG and AA genotype were susceptible to RA while GA was refractory. Recently Panoulas 10 also reported that GG genotype of TNF-β (+252) polymorphism occurs more frequently in RA patients as compared to general population. Earlier study from our laboratory showed an association of HLA-DRB1*04 and RA in Saudi patients. 35 Thus it may be postulated that GG and AA genotypes of TNF-β together with HLA-DRB1*04 might contribute to the RA susceptibility in Saudi population. Association of TNF-β alleles and HLA alleles with RA has also been reported in Japanese population. 14 These investigators reported that TNF-β * 2 (allele-A) along with HLA-DRB1*0405 contributed to the susceptibility to RA. Genetic variations in the TNF and HLA-DRB1 region have also been reported to affect the response to treatment of early RA. 36 In our study there was no significant association between the number of joints involved, RF positivity, duration of morning stiffness in Saudi RA patients and TNF-β (+252) polymorphism similar to TNF-α (–308) polymorphism.
Association of TNF-β polymorphism has also been reported with various other autoimmune disorders including Graves’ disease, 37 idiopathic membranous glomerulonephritis, IgA nephropathy, insulin dependent diabetes mellitus, 38 myasthenia gravis, 39 asthma diathesis, 40 SLE with nephritis, 41 systemic sclerosis 42 and plaque psoriasis. 43 This study indicates that besides its role in numerous autoimmune diseases TNF-β polymorphism is also involved in the pathogenesis of RA.
The present study suggested a significant association between allele frequency and genotype distribution of TNF-α (–308) and TNF-β (+252) polymorphisms and RA susceptibility in Saudi population. Our results together with other published reports supported an important role of ethnicity in the association of TNF-α and TNF-β polymorphism and RA. It is also concluded that TNF-α (–308) and TNF-β (+252) polymorphisms may work in tandem in the pathogenesis of RA in Saudi population. The results of this study may have prognostic value for future clinical observations of RA patients. Further, TNFα (–308) polymorphism may provide guideline in determining the response to anti-TNF α therapy as patients with GG genotype are better responders to anti-TNFα treatment than those with AA or GA.44–46
Funding
None.
Disclosures
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors of this paper report no conflict of interest. The authors confirm that they have permission to reproduce any copyrighted material.