
Abstract
Osteoarthritic changes in the facet joints are common in the presence of degenerative disc disease. Changes in the joint capsule accompany changes in the articular surfaces. Intraspinal synovial cysts that cause radicular pain, cauda equina syndrome, and myelopathy have been reported; however, there have been few reports in orthopedic or neurosurgical literature regarding hypertrophic synovitis of the facet joint presenting as an incidental para-articular mass. Here, we report a case of hypertrophic synovitis causing root pain. We describe the case of a 65-year-old man suffering from right sciatica and right leg pain in the L5 nerve-root dermatome for 1 year; magnetic resonance imaging (MRI) revealed an enhanced mass around the L4–5 facet joint. We investigated this mass pathologically. After right medial facetectomy, the symptoms resolved. Pathological investigation revealed this mass was hypertrophic synovitis. Hypertrophic synovitis of the facet joint might cause root pain.
Introduction
Degenerative disease in the intervertebral disc is generally associated with damage to the posterior joints. Minor strains in the articular ligaments produce synovitis of the facet joint. Rupture of the synovium results in hemarthrosis (7)(9). When the synovium is torn, hemarthrosis results (9). As observed in all diarthrodial joints, fibrillation and degeneration of the cartilage accompany cartilage erosion. Further, osteophyte formation occurs at the joint periphery or the entire articular process increases in size (3). Such kinds of changes in the facet joint capsule are recognized with the changes in the articular surfaces and lead to the hypertrophic synovitis of the facet joint. It might occur and compress the root, thereby causing root pain. However, there are few reports in orthopedic or neurosurgical literature regarding hypertrophic synovitis of the zygapophyseal joint presenting as an incidental para-articular mass (7)(4).
Case Report
A 65-year-old man suffering from right sciatica and right leg pain in the L5 nerve-root dermatome for the past 1 year visited our clinic. Initially, his pain was localized to the lumbosacral area; however, after several months, the pain radiated to the right lower extremity. Following two separate trials of complete bed rest for 1 month at home, he was admitted to the hospital. Neurologic examination demonstrated slight weakness of the right extensor hallucis longus muscle, hypesthesia in the right L5 dermatome. T1, T2 -weighted magnetic resonance imaging (MRI) revealed a slightly shortened ring-like mass at the level of L4–5 disc. The mass was enhanced with gadolinium-diethylenetriaminepentaacetic acid (Gd-DTPA)(Figs. 1, 2). There was no cystic formation around the facet (Figs. 1, 2). The patient was taken to the operating room where he underwent partial laminectomy with medial facetectomy. During the surgery, as the paravertebral muscle was separated from its attachments to the underlying spinous processes and laminae, the dorsal capsule of the right L4–5 facet joint was observed to be hypertrophic, and the right L5 nerve root was compressed under it (Fig. 3). Therefore, medial facetectomy was performed, and the right L5-nerve root was decompressed. Histological examination of hematoxylin-eosin (HE) revealed a vessel with inflammatory cells (Fig. 4a: arrow) and a slightly basophilic portion embedded in the connective tissue (Fig. 4a: arrow heads). The portion showed metachromasia on toluidin-blue staining (Fig. 4b: arrow heads). It indicated a cartilage formation and hypertrophic chondrocytes. Thus the diagnosis of hypertrophic synovitis of facet joint was made.
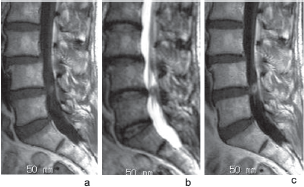
Sagittal T1 (a) and T2 (b)-weighted magnetic resonance images revealing a slightly shortened ring-like mass located at the level of the L4–5 disc. The mass was enhanced with gadolinium-diethlenetriaminepentaacetic acid (Gd-DTPA) (c).

Axial plain T1-weighted image (a). Axial T1-weighted image with Gd-DTPA revealing enhancement (arrow) around the facet (b).
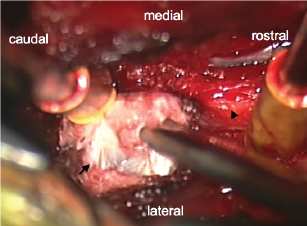
Intra-operative picture. The white color mass was recognized at the right L4–5 paraarticular region (arrow), and the right L5 nerve root (arrow head) was compressed under it.

Hematoxylin-eosin staining (HE)(a). High-power view of Toluidin-blue staining (b). Histological examination of HE revealed a vessel with inflammatory cells (Fig. 4a: arrow) and a slightly basophilic portion embedded in the connective tissue (Fig. 4a: arrow heads). The portion showed metachromasia on toluidin-blue staining (Fig. 4b: arrow heads).
Postoperative MRI and CT revealed no mass (Fig. 5). Postoperatively, his right sciatica resolved.

Postoperative sagittal T1- (a) and T2 (b)-weighted images. Axial T1-weighted image (c) revealing no preoperative mass. Postoperative axial computed tomography (CT) image revealing partial laminectomy and medial facetectomy (d).
Discussion
Intraspinal synovial cysts that cause radicular pain, cauda equina syndrome, and myelopathy have been reviewed (7)(6) most recently by Baum and Hanley (1) and Kjerulf et al. (5). Although the histopathologic findings in the synovial membranes after trauma are well known (9), the limited number of reports on this topic have not adequately dealt with the etiology or incidence of these benign lesions.
Osteoarthritic changes in the facet joints are common in the presence of degenerative disc disease. Changes in the joint capsule accompany changes in the articular surfaces. The dorsal capsule thickens and frequently develops areas of cartilage within its substance. With continuing avulsion, reinjury, and scarring, synovial loculations can form that can trap within themselves fibrotic elements, connective tissue, or clefts that represent the collapsed synovium.
In studies of autopsy specimens, nodules considered to be primarily cartilaginous in origin have been described as varying in size from barely visible to large masses protruding like beads behind and below the facet articulations (2).
In our case, the synovium was observed to have hypertrophied with inflammation. With continuing avulsion, reinjury, and scarring, synovial loculations were formed. Fibrotic elements, connective tissue, and clefts representing the collapsed synovium were trapped within these loculations. The Gd-DTPA-enhanced hypertrophic synovium indicated synovitis.
Hypertrophic synovitis of the facet joint is a common pathologic process that may rarely be observed as a true intraspinal neoplasm; however, it appears to occur incidentally as a para-articular mass in 2% of lumbar laminectomies for the removal of a herniated disc (7)(8).