
Abstract
Objective
To study whether the analysis of synovial fluid (SF) inflammatory cells can be used for the estimation of the grade of inflammation in the synovium and, therefore, for the prediction of the possible development of joint destruction in spondylarthropathy.
Methods
Forty-one patients with spondylarthropathy and hydropsy in a knee joint were studied. The cellular composition of SF aspirates was investigated and the grade of inflammation in synovial biopsy samples was evaluated by analyzing histological needle biopsy specimens.
Results
The count of SF polymorphonuclear leukocytes (PMN) reflected significantly the activity of acute inflammation. None of the SF cells reflected the chronic inflammation in the synovium.
Conclusion
The number of SF PMNs may reflect the severity of acute inflammatory process in the synovium in patients with spodylarthropathy at a given moment, but the analysis of SF aspirates may not be of use in estimating the activity of chronic phase of inflammation presumably causing the joint destruction.
Introduction
One of the characteristic clinical features of spodylarthropathies is the swelling of knee joints with increased volume of synovial fluid (SF). The joint inflammation component is characterized by accumulation of blood leukocytes into synovial tissues and fluid, as well as increased angiogenesis. The composition of SF is believed to reflect the pathological process in the in the synovium. SF analyses are commonly used as an aid to diagnose arthritis and to evaluate the inflammatory activity of joint effusions. Normal SF contains less than 200 leukocytes/mm3, whereas in acute phases of inflammatory arthropathies the leukocyte count is considerably higher and may be more than 50000/mm3 (1). However, it still remains largely unsolved whether the analyses of SF aspirates can be used to estimate the activity of chronic inflammation, supposed to be responsible for destructive changes and so possibly of prognostic significance.
In this study we have evaluated the relationship between the cellular composition of SF and the activity of inflammation in the synovium.
Materials and Methods
Patients
Forty-one patients with spondylarthroparhy and hydropsy in a knee joint were investigated. Nineteen of them were women and 22 were men. The median age of the patients was 49 (range 19–76) years and the median duration of arthritis was 0.5 (range 0.1–24) years. Twenty had psoriatic arthritis, 14 had reactive arthritis and 7 had seronegative oligoarthritis (undifferentiated spondylarthropathy). The HLA B27 antigen was investigated in 23 patients and it was positive in 9 of them. Twenty-six of the patients had no medication, 19 received non-steroidal anti-inflammatory drugs (NSAID), 3 disease modifying antirheumatic drugs (DMARD), corticosteroids and NSAID, one DMARD and NSAID and one DMARD and prednisolone. The study was performed in accordance with the principles of the Declaration of Helsinki and was approved by the Ethics Committee of the Satakunta Central Hospital District. Prior to enrolment in the trial, the purpose of the study was explained to all patients and their informed consent was obtained. The knee joints were aspirated and synovial biopsies were performed blindly from the suprapatellar pouch using Parker-Pearson needle (2). At least two specimens were obtained within the range of the needle.
Analyses of sf and Synovium Biopsy Samples
The following SF variables were investigated: the number of leukocytes, polymorphonuclear leukocytes (PMN) and mononuclear cells. The number of leukocytes was evaluated microscopically and that of PMNs and mononuclear cells by using the method of May-Grundwald-Giemsa (3). The histological needle specimens were fixed in neutral buffered formalin, embedded in paraffin, cut in 5 micrometer thick sections and stained with hematoxylin and eosin. The activity of acute inflammation of synovium was evaluated by calculating microscopically the number of PMNs and that of chronic inflammation by calculating the number of total mononuclear cells (lymphocytes, macrophages and plasma cells) in an area of 0.1 mm2 of the most affected part of the specimen. The patients were divided into two groups according to both the acute and the chronic components of inflammation.
Statistical Analysis
The investigated SF variables between the groups were compared using t-test and SF variables with the age and the duration of the disease of the patients using the Pearson's correlation coefficient.
Results
There were no significant differences in SF variables between the males and the females. The correlation between duration of the disease and the PMNs was not significant (r = 0.11, p = 0.55) and there were also no significant correlations between the other investigated SF variables neither with the age nor the duration of the disease of the patients.
Acute inflammation
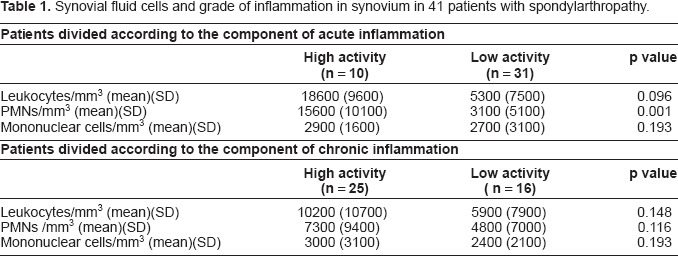
Ten patients had one or more PMNs in an area of 0.1 mm2 of the most affected part of the specimen and formed the high activity group of acute inflammation. The remaining 31 patients had no PMNs in the corresponding area and they formed low activity group of acute inflammation. Of the studied SF cells only PMNs differed significantly (p = 0.001) between these groups being higher in patients with high activity of inflammation (Table 1).
Synovial fluid cells and grade of inflammation in synovium in 41 patients with spondylarthropathy.
Chronic inflammation
Twenty-five patients had 2 or more mononuclear cells in an area of 0.1 mm2 of the most affected part of the specimen and they formed the high activity group of chronic inflammation. The remaining 16 patients had 0 or 1 mononuclear cells in the corresponding area and they formed the low activity group of chronic inflammation. None of the studied SF cells differed significantly between these groups (Table 1).
Discussion
Inflammatory changes in all rheumatic diseases that cause joint destruction include both local and systemic aspects. Synovial inflammation may be divided into an acute component dominated by vascular changes and PMN infiltration and into a chronic one dominated by reparative processes and the infiltration of mononuclear cells. This distinction, however, is somewhat artificial since both processes occur simultaneously influencing continually each other. The joint destruction in inflammatory arthritis has commonly been regarded to result mainly from chronic rather than from acute type of inflammation (4).
In this study the SF PMNs had a significant relationship with the activity of acute inflammation of the synovium, but they had no significant connection with the activity of chronic inflammation, which may lead to joint destruction in patients with arthritis. Also the SF leukocytes were considerably higher in patients with high activity group of acute inflammation than in that of low activity, but the difference did not reach the level of significance.
Synovial membrane biopsies are performed mainly for diagnostic purposes (5). In most studies synovial tissue has been obtained for analysis following blind or arthroscopic biopsy of the knee joint. These two techniques migth yield contrasting tissue characteristics, since needle biopsy provides access mainly to the suprapatellar pouch, whereas arthroscopy allows access to most areas of the joint, including the cartillage-pannus junction. However, according to a recent study by Youssef et al. (6) most measures of inflammation in synovial tissue samples obtained blindly were similar to those obtained at arthroscopy in patients with rheumatoid arthritis (RA). Also in our study at least 2 biopsies were taken in order to obtain representative samples and no differences were seen between the different samples.
Altough the pathogenesis of spondylartopathies differs from that of RA (7), the present results are in accordance with studies concerning the prognostic significance of synovial fluid analysis in RA, where SF cells did not predict the radiologically detected progress of joint destruction during the period of 3 or 7.5 years (8,9). To our knowledge, there are no studies concerning the prognostic significance of SF in spondylarthropathies in this respect. It is still possible that longitudinal levels of SF cells could predict the joint destruction in inflammatory arthritis. However, it would be almost impossible to arrange studies, where SF analysis were made at regular intervals, since especially locally treated joints may be free from hydropsy for years.
These results indicate that of the SF cells only PMNs may significantly reflect the activity of acute inflammation but not that of chronic inflammation of synovium which may lead to joint destruction in patients with spondylarthropathy.