
Abstract
The aim of this study was to present a rationale to explore the use of clinical tests for the sacroiliac joints to detect early axial spondyloarthritis (SpA) and to suggest a protocol to validate these clinical tests. Based on the European Guidelines for Diagnosis and Treatments of Pelvic Girdle Pain, we propose a set of six clinical tests to identify the likely presence of inflammation in the sacroiliac joints associated with early axial SpA. As magnetic resonance imaging (MRI) is the current gold standard used to identify inflammation in the sacroiliac joints, the results of the proposed set of clinical tests are compared with those from the MRI examinations. We hypothesize that specific clinical tests, which combine pain provocation and functional tests, for assessing the sacroiliac joints will help to identify early active inflammation at the sacroiliac joints in axial SpA. If such tests prove to be sensitive and specific, they could add further value to the diagnostic classification criteria for axial SpA.
Introduction
New criteria for the identification and classification of spondyloarthritis (SpA) were developed by the Assessment of SpA International Society (ASAS)1,2 and have now been widely adopted. These criteria can be used to identify patients with predominant axial symptoms and have led to a new designation of non-radiographic axial SpA, which in some cases is a prodrome to the later development of ankylosing spondylitis.1,2 The term axial SpA is now used to classify not only patients with ankylosing spondylitis but also patients with inflammatory spinal pain associated with other forms of SpA, including reactive arthritis, psoriatic arthritis, enteropathic arthropathies, and undifferentiated SpA. 3 The principal features observed in patients with axial SpA are chronic low back pain and inflammation of the sacroiliac joints. 4 Unchecked inflammation can cause structural damage to the sacroiliac joints and spine over time, resulting in postural changes and decreased quality of life. 4 The prevalence of ankylosing spondylitis is 23.8, 16.7, and 12.2 per 10,000 inhabitants in Europe, Asia, and Latin America, respectively, 5 although different prevalence rates were reported for different European countries. 5 The prevalence rate of axial SpA considering the ASAS new criteria1,2 is estimated to be 3–4 times higher than that of ankylosing spondylitis. 6
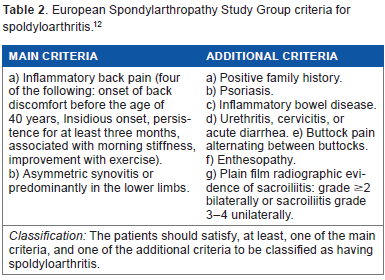
The most common classification criteria used for ankylosing spondylitis are the modified New York criteria (Table 1). 7 These criteria require the identification of advanced radiological changes at sacroiliac joints. 7 Although the modified New York classification identifies patients with well-established disease, its sensitivity is low for those with early inflammatory back pain that precedes radiographic change. 8 Such structural damage occurs several years after the onset of symptoms, and hence, these criteria do not identify patients in the early stages of disease. 9 The modified New York criteria also consider spinal mobility measures to classify patients with ankylosing spondylitis. However, the validity of these clinical tests has been questioned. 10 There are two other commonly used criteria for the diagnosis of SpA: the Amor criteria 11 and the European Spondylarthropathy Study Group criteria (Table 2). 12 These criteria have high sensitivity but lack specificity. 13
Modified New York criteria for ankylosing spondylitis. 7

European Spondylarthropathy Study Group criteria for spoldyloarthritis. 12
The development of biological therapies, specifically those targeting tumor necrosis factor alpha, has revolutionized the management of SpA, offering an effective therapy for the first time. 4 Furthermore, studies have suggested that continuous therapy with nonsteroidal anti-inflammatory drugs may retard radiological progression. 14 The advent of effective therapy has led to the suggestion that earlier diagnosis and earlier initiation of therapy may retard radiological progression and reduce disability. 15 To identify the early stage SpA, the ASAS group specifically included magnetic resonance imaging (MRI) in their criteria in order to identify active inflammation in the sacroiliac joint occurring prior to radiographic changes (Fig. 1). These criteria reached a sensitivity of 82.9% and a specificity of 84.4% in patients with chronic low back pain and of age at onset lower than 45 years. 2 The findings from the ASAS study suggest that the most relevant feature for early diagnosis of axial SpA is the detection of active inflammation of the sacroiliac joint, which was present in 64.7% of the patients with axial SpA (assessed by MRI) and only in 2.6% of the patients with no SpA. 2 The sensitivity and specificity of disease based solely on pelvic imaging (X-ray or MRI) were 66.2% and 97.3%, respectively. 2 Although the ASAS criteria (in particular MRI) present excellent sensitivity and specificity, they are dependent on the availability of MRI that is frequently resource limited and an expensive examination. Identifying physical factors (singularly or in combination) strongly associated with inflammation in the sacroiliac joint (demonstrated by MRI and biomarkers) may help to identify a subgroup of patients with inflammatory back pain. These patients will be most likely to have active inflammation detectable on MRI. Such an approach may improve the early identification of axial SpA that helps to control the healthcare costs.

Pelvic girdle pain resulting from a wide variety of causes can be assessed reliably by a combination of manual clinical tests. 16 However, imaging techniques have been used most commonly in patients suspected of having axial SpA to confirm sacroiliac joint involvement. 16 Currently, the validity and reliability of the clinical tests for assessing the sacroiliac joints in patients with axial SpA are not established. The aim of this study is to present a rationale to explore the use of clinical tests for the sacroiliac joints to detect early axial SpA and to suggest a protocol to validate these clinical tests. We hypothesize that specific clinical tests, which combine pain provocation and functional tests, for assessing the sacroiliac joints will help identify the presence of early active inflammation in these structures in axial SpA. If such tests prove to be reliable, sensitive, and feasible, they could add further value to the diagnostic classification criteria for axial SpA. The clinical relevance of such set of clinical tests is as follows: (i) providing an alternative approach for assessing active inflammation in the sacroiliac joint when MRI is not available; (ii) providing justification for performing MRIs; (iii) discriminating sacroiliitis from low back pain of mechanical origin; (iv) helping primary care clinicians identify chronic back pain patients with potential axial SpA at an early stage and refer appropriately; (v) increasing the sensitivity and specificity of the current classification criteria for axial SpA; and (vi) improving the understanding of sacroiliac joint behavior in early axial SpA. Furthermore, it may be possible to use current knowledge of the biomechanics of the pelvic girdle to develop clinical tests capable of identifying sacroiliac joint dysfunction in patients with the early stage axial SpA. Such a result could provide a valuable tool for the evaluation of patients with SpA.
Pelvic Girdle
Optimal stability in the pelvic girdle is achieved when performance and effort are balanced. 16 Optimal joint stability is reached by appropriately coordinated muscle and ligament forces, which promote a smooth and effortless transference of load and movement. Altered joint laxity or stiffness may affect joint position, alter joint compression, and disturb the balance between performance and effort, reflecting as nonoptimal joint stability. 16 Changes in the pattern of movement, pain, and functional disturbances in the sacroiliac joints may either be provoked or in turn provoke nonoptimal stability.16,17 In order to understand biomechanical dysfunction at the pelvic girdle, specific clinical tests must be used to assess the function, as well as to stress the symptom provocation. 16
Clinical Assessment of the Pelvic Girdle
Although clinical tests used to assess the pelvic girdle can be classified as pain provocation tests, as well as mobility tests and functional – load transfer – tests, there is no consensus regarding the reliability of these procedures. van der Wurff et al. 18 systematically reviewed the literature and observed poor inter-examiner reliability when using mobility tests to assess the sacroiliac joint. They advised that mobility tests should not be used in daily clinical practice. Hence, mobility tests were not considered for inclusion in this study. On the other hand, moderate-to-excellent reliability has been found for pain provocation tests.18,19 However, for some patients, pain may not accurately reflect biomechanical dysfunction. 20 Functional tests have gained acceptance in the assessment of pelvic girdle dysfunction, as their validity 21 and reliability20–22 have been recognized in sample populations. Both pain provocation and functional tests appear to be important in order to fully understand the mechanisms underlying dysfunction in patients with low back pain suspected of having pelvic girdle dysfunction. 16
Pain Provocation Tests
These clinical tests aim to stress the sacroiliac structures in order to identify dysfunction by producing pain. Among the sacroiliac joint tests, the pain provocation tests are the most acceptable and are most frequently used in clinical contexts. 16 The European guidelines for the diagnosis and treatment of pelvic girdle pain 16 suggest the following four provocation tests for clinical use (Fig. 2): (i) Gaenslen's test, (ii) posterior pelvic pain provocation test (also named as thigh thrust), (iii) Patrick's test (also named as FABER test), and (iv) palpation of the long dorsal sacroiliac joint ligament. Although these tests individually have very high specificity, their sensitivity is low. Thus, it was recommended to use all the tests to fully assess the sacroiliac joints. 16

Pain provocation tests: (A) Gaenslen's test; (B) Posterior pelvic pain provocation test; (C) Patrick's (FABER) test; and (D) Palpation of the long dorsal sacroiliac joint ligament.
Functional Tests
Active straight leg raise.
Active straight leg raise is the main functional clinical test used to assess the pelvic girdle (Fig. 3A). It assesses the ability of the pelvis to transfer load between the spine and lower limbs. 22 During this test, there is a forward rotation of the ipsilateral hip, while reaction forces are being generated in the sacroiliac joints, iliolumbar ligaments, and pubic symphysis. As a consequence, the lower lumbar spine is pulled in the side flexion to the ipsilateral side and rotated to the contralateral side. The intricate mechanism of force distribution between sacrum, lumbar spine, and hips is influenced by the mobility of their connections and makes every part of this complex system able to influence the active straight leg raise. 21 This test was found to be reliable, having good sensitivity and specificity in a population of patients with pelvic girdle pain related to pregnancy.21,22 The active straight leg raise is also recommended in the European guidelines for diagnosing pelvic girdle pain. 16

Functional tests: (A) Active straight leg raise; and (B) Stork test on the support side.
Stork test on the support side.
This test allows assessing the load transfer between lower limbs and spine during a weight bearing task (Fig. 3B). Based on the self-bracing mechanism, prior to the movement, it is expected to have the preactivation of lumbo-pelvic muscles, 23 and tensioning of fascia and ligaments promotes a relative posterior rotation of the innominate bone that puts the sacroiliac joints in maximal contact (closed pack position). Hungerford et al. 20 rated the ability of physiotherapists as good for discriminating between no movement and anterior rotation of the innominate bone relative to the sacrum during this test. In the presence of pelvic girdle pain, anterior rotation of the innominate relative to the sacrum appears to be common and is a likely consequence of failure of the self-bracing mechanism and poor stabilization of intrapelvic motion.20,24
Pelvic Girdle and Axial SPA
A previous study assessed the diagnostic accuracy and reliability of pain provocation tests for the sacroiliac joints in patients with chronic low back pain potentially related to early axial SpA. 25 Seven pain provocation tests (namely Gaenslen's test, Patrick's (FABER) test, Mennell test, compression test, posterior pelvic pain provocation test, sacral thrust test, and distraction tests), as well as MRIs of the sacroiliac joints, were performed. From the 40 patients enrolled in the study, 13 showed acute/active inflammatory changes in the sacroiliac joint on MRI. Ozgocmen et al. 25 verified that although these pain provocation tests are reliable for assessing sacroiliac joints in patients with low back pain, they lack discriminatory capacity. The pain provocation tests reached a sensitivity of around 50% and specificity of around 80%. Ozgocmen et al suggested either a multi-test regimen of four out of five positive tests or alternatively two out of three as cutoff values to reach a favorable decision.
It is important to consider, however, that during the early stages of biomechanical dysfunction, tenderness may be under the threshold of reportable clinical pain induced by these clinical tests. 26 Thus, pain provocation tests might be negative even in the presence of joint dysfunction. If pain provocation tests are used in isolation, they may display poor sensitivity. Another study assessing patients with well-established axial SpA identified differences in hip and sacroiliac joint patterns of movement when compared with a control group. 27 However, it is unclear whether the changes in the pattern of movement were caused by structural damage, inflammation, the combination of both, or other factors. An alternative potential method of identifying inflammation at the sacroiliac joints is the use of functional clinical tests, which may identify dysfunction without producing significant pain. 20 These two categories of clinical tests (pain provocation and functional tests) cover a wider spectrum of features when clinically assessing patients of suspected sacroiliac joint dysfunction with low back pain. As a consequence, the sensitivity of such a set of tests could be higher, and the relevance in clinical contexts clearer.
Testing the Hypothesis– Research Proposal
In order to test such a hypothesis, we will enroll participants into a study who have chronic low back pain of unknown origin and insidious onset. Participants will be excluded if they have radiologically evident structural damage to the sacroiliac joints. Based on the European Guidelines for Diagnosis and Treatment of Pelvic Girdle Pain, 16 we propose a set of six clinical tests (four pain provocation tests and two functional tests, Figs. 2 and 3) to identify the likely presence of inflammation in the sacroiliac joints associated with early axial SpA. The reference standard used to determine the sensitivity and specificity of the set of clinical tests would be edema identified at the sacroiliac joints on MRI accepted as the current gold diagnostic standard.8,28
Complementary analyses to MRIs and X-rays will include the presence of inflammatory back pain, comorbidities (peripheral arthritis, uveitis, dactylitis, psoriasis, inflammatory bowel disease, and positive family history of SpA), good response to nonsteroidal anti-inflammatory drugs, positive HLA-B27, and elevated C-reactive protein and will provide additional support for diagnosis. Thus, the study will compare the sensitivity and specificity obtained using the new criteria (clinical tests) when compared with the current ASAS criteria.
A statistical approach will use 2 × 2 contingency tables to calculate specificity, sensitivity, positive and negative predictive values, and likelihood ratios for each independent clinical test, for the composite of the four pain provocation tests, for the composite of the two functional tests, and for the composite of all the six tests.
Alternative Classification Criteria for Axial SPA
We hypothesize the eventual construction of a reliable, valid, sensitive, and specific classification criterion where neither imaging nor blood examinations are required. This criterion would be based exclusively on clinical tests and patient's history (Fig. 4). These clinical tests could also be used to implement the current classification criteria when MRI is not available.

Alternative classification criterion to axial SpA.
Conclusion
By investigating the validity of a combination of clinical tests, we consider that the identification of pelvic girdle dysfunction may be possible with acceptable sensitivity and specificity in patients with axial SpA. If this identification is proved feasible, this combined test could improve the classification criteria for axial SpA by enabling a cost-effective alternative to identify early axial SpA. Specifically, clinicians working in primary health care, in low-income rehabilitation centers, and in regions with limited technology and funding would gain substantial benefit by allowing them to identify patients with potential axial SpA at an earlier stage and refer appropriately. Further investigation of the biomechanics of pelvic girdle in patients with early axial SpA may also provide new insights into the pathogenesis, prognosis, and physical management of this condition.
Author Contributions
Conceived and designed the experiments: MPC, SMS, SM, MDB. Wrote the first draft of the manuscript: MPC. Contributed to the writing of the manuscript: MPC, SMS, SM, MDB. Agree with manuscript results and conclusions: MPC, SMS, SM, MDB. Jointly developed the structure and arguments for the paper: MPC, SMS, SM, MDB. Made critical revisions and approved final version: MPC, SMS, SM, MDB. All authors reviewed and approved of the final manuscript.