
Abstract
BACKGROUND:
Pelvic girdle pain represents a group of musculoskeletal pain disorders associated with the sacroiliac joint and/or the surrounding musculoskeletal and ligamentous structures. Its physical management is still a serious challenge as it has been considered the primary cause of low back pain.
OBJECTIVE:
This review sought to determine the effectiveness of motor control exercises for two clinically relevant measures; i.e., pain and disability, on patients with pelvic girdle pain of sacroiliac joint origin.
METHODS:
This review covered only randomized controlled studies. Online databases, such as PubMed, Embase, Scopus, and Cochrane Library, were searched from January 1, 1990, to December 31, 2019. PEDro scale was used to assess the methodological quality of included studies, while Review Manager was employed to synthesize data in view of meta-analysis. The PRISMA guidelines were applied for this review.
RESULTS:
Twelve randomized controlled trials of moderate-to-high quality were included in this review. The studies involved 1407 patients with a mean age ranging from 25.5 to 42.1 years as well as intervention and follow-up durations from 1 week to 2 years. Motor control exercises alone for pelvic girdle pain of sacroiliac joint origin were not effective in terms of pain reduction (SMD
CONCLUSION:
Motor control exercises alone were not found to be effective in reducing pain at short-term. However, their combination with other musculoskeletal therapies revealed a significant and clinically-relevant decrease in pain and disability at short-term, especially in peripartum period.
Keywords
Introduction
Pelvic girdle pain (PGP) represents a small but significant group of musculoskeletal pain disorders associated with the sacroiliac joint (SIJ) and/or the surrounding musculoskeletal and ligamentous structures [1]. Specific inflammatory pain disorders of the SIJs, such as sacroiliitis, are the most readily identified PGP disorders [2]. However, PGP more commonly presents as ‘non-specific’, often arising during or shortly after pregnancy [3, 4, 5] or following traumatic injury to the pelvis (pelvic bone fractures, ligamentous injuries) [6, 7].
SIJ pain has been acknowledged to be localized or pseudoradicular [8]. In 1905, it was for the first time reported to a potential source of low back pain (LBP) [9], whereas later, it was considered its primary cause in 15 to 72% of cases [10, 11], its prevalence ranging from 10 to 75% [12, 13]. The SIJ pain can cause groin, buttock, and thigh pain; via this mechanism it is likely to affect pelvic girdle biomechanical efficiency, daily life activities and functional movements [10].
Some risk factors such as abnormal gait pattern, leg length discrepancy, scoliosis, direct trauma, natural lumbar fusion with the sacrum, post-surgery, idiopathic onset, and pregnancy state have been reported to date [14, 15, 16]. In pregnant women, the increased laxity of soft-tissues surrounding the SIJ and greater synovial fluid volume can lead to increased SIJ motion, which diminishes the efficiency of load transmission and increases the sheer forces across the joint [17]. SIJ assessment is specific and is based on combining several pain provocation tests [18], whereas LBP assessment is based on a problematic and specific movement direction in addition to contributing factors [19]. However, PGP probably stems from multifactorial sources as does non-specific LBP within the biopsychosocial model [20]. Therefore, this review focused on PGP of SIJ origin.
Search terms used for database searches
Search terms used for database searches
Standard physical therapies are being used to cure the underlying pathology, in addition to reducing or alleviating the SIJ symptoms. Such interventions include manual joint mobilization and manipulation, sacroiliac belts, massage, patient education, aerobic conditioning, electrotherapy, and repetitive exercises, including motor control exercises (MCE) [21, 22].
Concerning physical therapy, there is an urgent need for an effective intervention strategy for managing PGP of SIJ origin. Such a treatment strategy has already been reported in the literature. However, no systematic review with meta-analysis, which aimed to investigate the effectiveness of MCE alone or MCE combined with other musculoskeletal therapies (MSKTS), has been conducted while being focused on PGP of SIJ [10, 23]. Nevertheless, definite conclusions concerning the use of MCE in patients with PGP of SIJ are still pending. Therefore, this research primarily sought to determine the effectiveness of MCE, as the standard exercise, on two clinically relevant parameters, i.e. pain and disability on patients with PGP of SIJ origin.
The review protocol was registered into PROSPERO under registration number CRD42020193186. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were employed for conducting this review [24].
Search strategy
The PubMed, Embase, Scopus and Cochrane Library databases were searched for relevant clinical trials. The following criteria were definied to guide our search strategy:
Participants/population: Patients (men and women) suffering from PGP of SIJ origin.
Interventions: These were MCE, such as pelvic girdle muscle strengthening exercises, pelvic-tilt exercises with pelvic floor muscle (PFM) voluntary contraction, as well as exercises involving hip extension, abduction, and abdominal crunches.
Comparators: These were other MSKTs that were used as controls, such as physical therapy modalities (massage, relaxation, joint mobilization, electrotherapy, hot packs, mobilizing and strengthening exercises, manipulation), pelvic realignmet device, as well as no rigid lumbopelvic belt.
Outcome measures: Pain [Visual Analogue Scale (VAS)] and disability [Pelvic Girdle Questionnaire (PGQ), Disability Rating Index (DRI), and Oswestry Disability Index (ODI)] were the main outcomes.
Selection criteria: (1) Randomized controlled trials (RCTs); (2) concerning patients with PGP of SIJ, diagnosed by means of SIJ tests or SIJ intra-articular steroid injections; (3) using specific MCE or exercises aimed at activating, training, or restoring PFM’s stabilization function; (4) reported lower back, lumbopelvic, or PGP referred from SIJ; (5) reports published between January 1,1990, and December 31, 2019; (6) papers written in English or French. The exclusion criteria for studies were as follows: (1) score
Methodological assessment of RCTs
The PEDro scale, which is deemed a valid and reliable tool for assessing RCTs [25, 26], was used for sample assessment. RCTs’ quality was blindly judged by two different reviewers (MJ and NG) in order to minimize potential bias [27]. Accordingly, RCTs were divided into three categories, as follows: low quality (0–3/10), moderate quality (4–6/10), and high quality (7–10/10). An overall assessment of the studies included was additionally performed based on whether each individual criterion was fulfilled.
Quality of evidence assessment
The reviewers (MJ and NG) employed the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework to assess the evidence level for each study included in the meta-analysis [28]. Evidence from RCTs considered of ‘high’ quality was graded down in the presence of concerns with risk of bias, indirectness, inconsistency, imprecision, or publication bias [29, 30, 31, 32, 33]. The risk of bias among the studies was considered ‘serious’ when the studies that contributed the most to the pooled result exhibited a ‘high’ risk of bias. For qualitative analysis, strength of evidence was determined by grouping similar Patients Interventions Comparisons Outcomes Study design (PICOs) to provide an overall level of evidence [34, 35].
Study selection and data extraction
The studies, along with their titles, abstracts and data were identified and screened by two independent reviewers (MJ and NG). Only eligible full text studies were retrieved and then screened again by the same reviewers. In addition, the reference lists of the identified studies were manually checked for further inclusions. The same reviewers collected the included studies, classified them and displayed their main characteristics (Table 1).
Flowchart of the study design.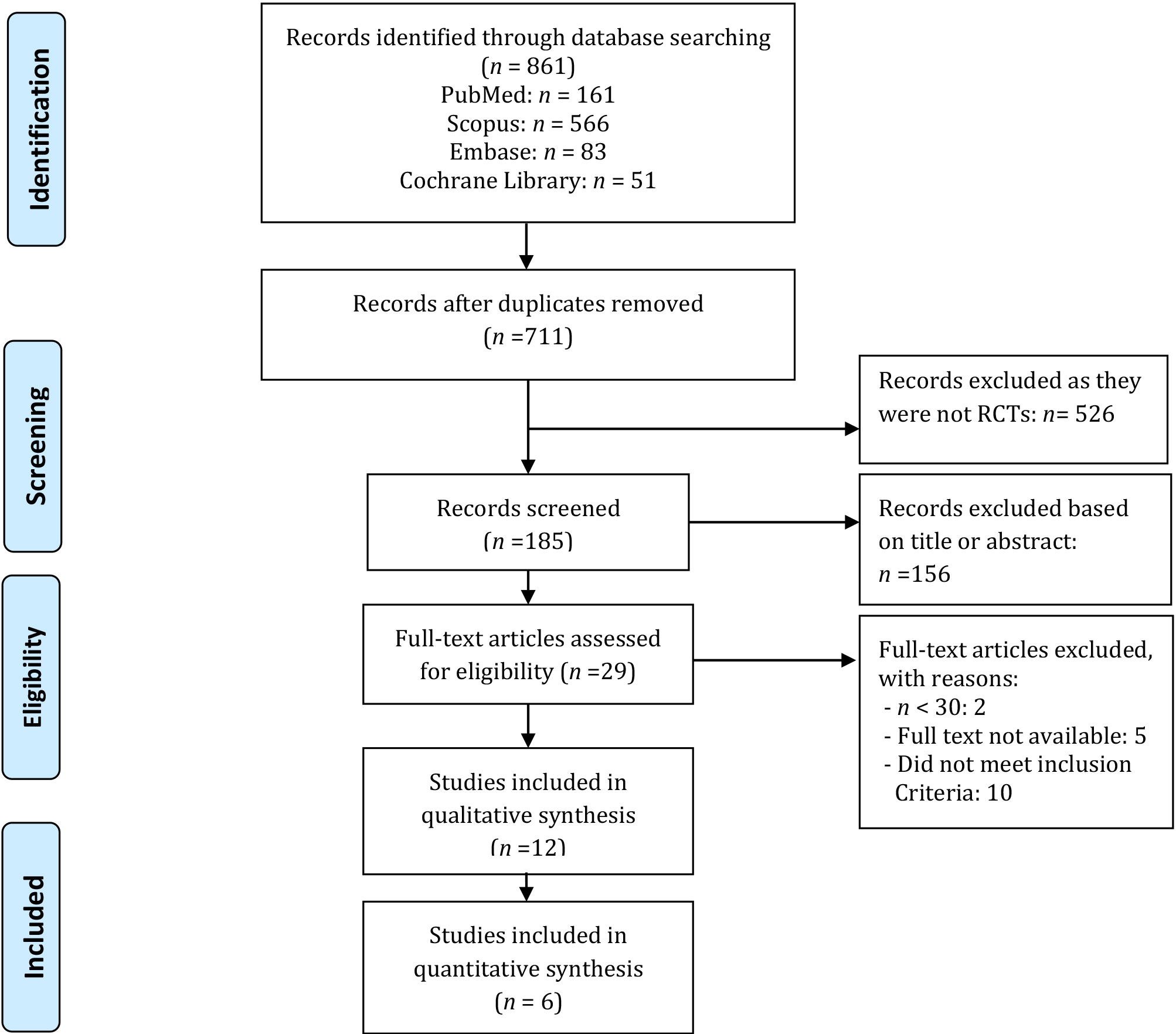
Results from studies exhibiting similar PICOs were considered for being pooled into separate meta-analyses. Pooled standard mean differences (SMDs) were calculated using Review Manager (RevMan V.5.3). Pooled estimates were calculated with their 95% confidence intervals (CIs) and an alpha level set at 0.05 [36]. Analyses were performed with random effects. The forest plots visual inspection was performed. The effect sizes (ES) calculated with SMD were interpreted using Cohen’s method; the effect was defined as small (0–0.20), medium (0.20–0.50), or large (0.50–0.80) [37].
MCE efficacy was judged based on the SMD interpretation [38]. Thus a SMD of zero means that the treatment in the intervention group (IG) and that in the control group (CG) display equivalent effects. If the improvement is associated with higher scores on the outcome measure, SMDs greater than zero indicate the degree to which the IG treatment is more effective than that administered to the CG, while SMDs less than zero indicate the opposite. If the improvement is associated with lower scores on the outcome measure, SMDs less than zero indicate the degree to which the IG treatment is more effective than that administered to the CG, while SMDs greater than zero indicate the opposite. In this review, considering the outcome measures (VAS and ODI), when SMD is less than zero the improvement is in favor of the IG, while SMD greater than zero indicates the opposite.
A quantitative analysis was performed for meta-analysis. I
0% to 40%: not relevant; 30% to 60%: may represent moderate heterogeneity; 50% to 90%: may represent substantial heterogeneity; 75% to 100%: considerable heterogeneity.
If a quantitative pooling was not performed, results were then qualitatively synthesized.
Study selection
We identified 861 potentially relevant studies, and after removing duplicates, 711 remained. Following title and abstract screening, we assessed 29 fulltext studies. Of these, 17 studies were excluded for different reasons after fulltext evaluation (Fig. 1). This systematic review took into account the remaining 12 RCTs, six of which were suitable for meta-analysis.
Characteristics of studies included in the review
Characteristics of studies included in the review
Abbreviations: LPP
Abbreviations: PFM
Abbreviations: QOL
Abbreviations: FU
PEDro scores
A
The twelve RCTs included 1407 participants with a mean age ranging from 25.5 to 42.1 years. Ten RCTs involved only women in peripartum period. Only one paper included both genders, while the remaining other did not report the participant characteristics. For more details, see Table 2.
Short-term effect of MCE versus other MSKTs on pain and disability.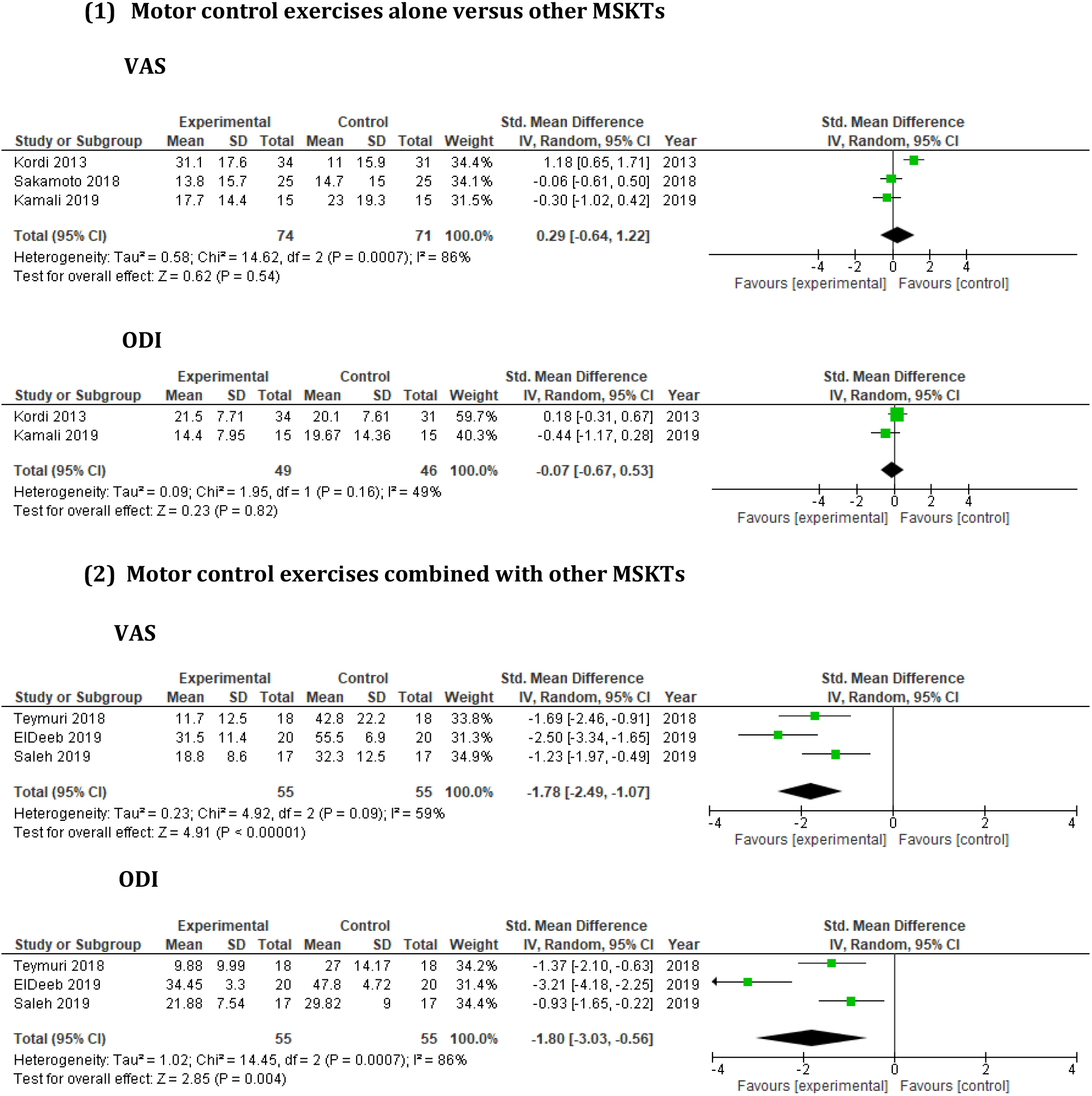
The PEDro score of the included studies ranged from 4 to 8/10. Four RCTs were considered as being of high quality (PEDro score: 7–8/10), with the remaining ones being of moderate quality (PEDro score: 4–6/10) (Table 3).
Interventions and comparators
Four RCTs compared MCE alone to other MSKTs [23, 39, 40, 41], while eight RCTs compared MCE (as detailed above) in combination with other MSKTs (as detailed above) to these MSKTs [10, 22, 42, 43, 44, 45, 46, 47].
Outcome measures
For pain assessment, the Visual Analogue Scale was used in all RCTs, but the assessment method was not further described in any study (Table 2). For self-reported function, Sakamoto et al. [40] and Nilsson-Wikmar et al. [44] used the Pelvic Girdle Questionnaire (PGQ) and Disability Rating Index (DRI) in their studies, respectively; the remaining studies used the Oswestry Disability Index (ODI) instead (Table 2).
Subgroup analysis
Short-term (
12 weeks [48, 49]) MCE effect on pain and disability
Short-term effect of MCE alone on pain and disability
Three RCTs [23, 39, 40] involving 145 participants were considered in order to evaluate the short-term effect of MCE alone on pain and disability, and were suitable for meta-analysis (Fig. 2).
Kordi et al. [39] compared the effects of lumbopelvic belt plus information about anatomy, body posture, and ergonomic advice, home based pelvic girdle MCE (pelvic girdle muscle strengthening such as aerobic, stretching and strengthening exercises) plus information and these information alone on pregnant women with PGP. Lumbopelvic belt was removed only during the sleeping time. MCE were performed 2–3 times per week for 6 weeks. The pain intensity in the belt group, in comparison to other groups, significantly decreased at both 3-week and 6-week follow-ups. The mean ODI score was also significantly more improved in the belt group compared to the MCE and information alone groups.
Sakamoto et al. [40] compared the effect of MCE (isolated voluntary contraction of the PFMs, pelvic-tilt exercises with voluntary contraction PFM contraction, exercises involving hip extension, abduction, and abdominal crunches) to exercises (stepping, pelvis shifting, pelvis rotation with knee extension, pelvis rotation with knee flexion, and trunk flexion and extension) with pelvic realignment device and to no therapy on LBP and PGP after childbirth. MCE and other exercises were repeated 10 and 10–20 times per session, respectively, and twice a day for four weeks post-delivery. The immediate and short-term exercise effects with a pelvic realignment device resulted in greater improvements in pain and disability compared to pelvic MCE alone.
Kamali et al. [23] compared the effect of manipulation and MCE (voluntary contraction of the local stabilizers of the lumbopelvic region to ensure segmental control in different positions such as supine, crook-lying, side-lying, prone, four-point kneeling, sitting, and standing) in patients with subacute or chronic SIJD. Patients pertaining to the manipulation group were treated individually three times a week for two weeks. In the MCE group, exercises in each position were performed using 10 repetitions for 20 min three times a week, for 4 weeks. Both groups demonstrated significant improvements in pain and disability, and there was no significant between-group difference in the treatment effects. This result suggests that neither manual therapy nor MCE therapy proves to be superior for treating PGP of SIJ.
Concerning the meta-analysis of the three above studies, in terms of pain and disability, the overall analysis demonstrated non-significant effect and moderate heterogeneity (Fig. 2). For pain and disability, SMDs were small and respectively greater and less than zero. These results showed that MCE alone for PGP were not effective in terms of pain reduction compared to other MSKTs, such as manipulation, pelvic realignment device, or no rigid lumbopelvic belt; however, MCE alone for PGP were slightly effective in terms of disability reduction at short-term follow-up (FU).
Short-term effect of MCE combined with other MSKTs on pain and disability
Seven RCTs involving 1051 participants were considered in order to evaluate the short-term effect of MCE combined with other MSKTs on pain and disability [42, 43, 44, 45, 46, 47]. Nevertheless, only three RCTs [45, 46, 47] were suitable for meta-analysis (Fig. 2).
Elden et al. [43] compared the efficacy of standard treatment (patient education about the condition, and back and pelvis anatomy, pelvic belt, home exercise programme designed to increase abdominal and gluteal muscle strength), standard treatment plus MCE (activation and control of local deep lumbopelvic muscles; training of more superficial muscles in dynamic exercises to improve mobility, strength, and endurance capacity) for PGP, and standard treatment plus acupuncture during pregnancy. Treatment was given twice a week over six weeks. After treatment, the MCE group experienced less pain in both the morning and evening than the standard group. The acupuncture group, in turn, had less pain in the evening than the MCE group. Moreover, the acupuncture group had less pain in both the morning and evening than the standard treatment group. These results indicate that both MCE and acupuncture constitute efficient complements to standard treatment for managing PGP with acupuncture being somewhat superior to MCE. In 2008, the same authors [42] described the post-delivery regression of PGP observed in these women using similar interventions over six weeks. Three-quarters of the women were pain-free three weeks after delivery, and there were no differences in recovery between the three treatment groups. PGP had resolved in 99% of the women twelve weeks after delivery.
Nilsson-Wikmar et al. [44] compared the efficacy of non-elastic sacroiliac belt plus oral or written information (about anatomy, body posture and ergonomic device), non-elastic sacroiliac belt plus oral or written information about PGP plus training programme (strengthening and MCE; lateral pulls, standing, leg press, sit-down rowing, and curl-ups), and non-elastic sacroiliac belt plus oral or written information plus home exercises in order to stabilize PFMs (exercises performed with a ball between knees in sitting, standing, and in four-point kneeling position with arm or leg movements, stretching of hamstrings, hip flexors and calf muscles at the end of exercise programme) in pregnant women with PGP. The treatments were performed twice a week from inclusion to gestation week 38; FUs were carried out at 3, 6, and 12 months after delivery. There was no significant difference in terms of pain and activity noticed among the three groups during pregnancy or at FUs.
Nejati et al. [10] compared the effectiveness of exercise therapy (self-mobilization, SIJ stretches, and spinal MCE), manipulation therapy, and the combination of the two on patients with SIJD. All groups demonstrated significant improvement in pain and disability compared to baseline. At 6 weeks, manipulation therapy showed notable results, while exercise therapy was associated with remarkable effects at 12 weeks.
Teymuri et al. [47] investigated the effects of MCE, such as local segmental control exercises (isometric contraction of PFMs and transverse abdominis co-contraction), open chain segmental control exercises (adding limbs’ movements during PFMs contraction), and closed chain segmental control exercises combined with electrotherapy in comparison to electrotherapy alone, in postpartum patients with lumbopelvic pain. Both groups were treated for 6 weeks, three times per week. After treatment, there was a significant decrease in pain and disability observed in both groups. However, MCE group showed a significant decrease in pain and disability, as compared to the electrotherapy group.
Saleh et al. [45] investigated the effect of core MCE (abdominal hollowing, bilateral knee raise, supine extension bridge, straight leg rise from prone, alternate arm and leg raise from quadruped position, and prone abdominal body bridge) in addition to infrared radiation and continuous ultrasound in comparison to infrared radiation and continuous ultrasound alone on lumbosacral region in patients with postpartum lumbopelvic pain. Both groups performed three sessions per week for 6 weeks. Both groups reported a significant improvement in VAS and ODI post-treatment. In MCE group, the improvements in VAS and ODI were more significant compared to traditional treatment group.
ElDeeb et al. [46] investigated the effect of PFM training, such as rhythmic, and sustained contractions combined with MCE (lumbar multifidus activation exercise and transverse abdominis drawing-in maneuver) versus these MCE alone on postpartum women with PGP. Both groups carried out the exercises three times a week for 3 months. In both groups, there was a significant decrease in pain and disability following the intervention. However, the PFM group exhibited a significant decrease in pain and disability, along with a significant increase in PFM strength, compared to the MCE group.
Concerning the meta-analysis of the three studies [45, 46, 47], the overall analysis demonstrated a significant effect with moderate and substantial heterogeneity for pain and disability, respectively, with large SMDs less than zero (Fig. 2). This analysis revealed that MCE when combined with other MSKTs prove to be more effective in terms of pain and disability reduction than control interventions alone in post-delivery patients at short-term FU.
Long-term (
12 weeks [50]) MCE effect on pain and disability
Long-term effect of MCE alone on pain and disability
One RCT involving 81 participants was considered to evaluate the long-term effect of MCE alone on pain and disability [41]. The authors compared the efficacy of specific MCE (deep local muscle training: transverse abdominal wall muscles with coactivation of the lumbar multifidus in the lumbosacral region; superficial global muscles training: gluteus maximus, latissimus dorsi, oblique abdominal, erector spinae, quadratus lumborum, as well as hip adductors and abductors) to physical therapies on post-pregnancy patients with PGP. Treatment was performed over 20 weeks with a 2-year FU. Significant between-group differences were observed in functional status, pain, and physical health in favor of MCE group, which were maintained at 2-year FU.
Long-term effect of MCE combined with other MSKTs on pain and disability
Three RCTs involving 250 participants were considered in order to evaluate the long-term effect of MCE combined with other MSKTs on pain and disability [10, 22, 44].
Stuge et al. [22] investigated the efficacy of physical therapy (massage, joint mobilization, relaxation, and stretching) combined with specific MCE and physical therapy alone on post-pregnancy patients with PGP. Treatment was performed three times a week for 18 to 20 weeks with a 1-year FU. After intervention and at 1-year FU, the MCE group exhibited significant lower pain intensity and disability compared to the control group.
In addition to the above short-term results, Nilsson-Wikmar et al. [44] also reported that pain and disability decreased in all groups between gestation week 38 and 12 months postpartum. Indeed, neither home nor clinic exercises had any additional value as compared to providing a nonelastic sacroiliac belt and information.
In addition to the detailed short-term results, Nejati et al. [10] found no significant difference among the study groups at week 24. Based on the study results, exercises and manipulation therapy appeared to be effective in reducing pain and disability; their combination, however, did not bring about significantly better therapeutic results than either approach implemented separately in SIJD-affected patients.
Discussion
This review sought to investigate the effectiveness of MCE of two clinical measures; i.e., pain and disability on patients with PGP of SIJ origin. Initially, the research concerned patients with PGP of SIJ in general, but applying the selection criteria led us to retrieve a majority of studies involving women in their peripartum period. This review identified twelve studies evaluating MCE either administered alone or combined with other MSKTs, as an intervention to manage PGP of SIJ. Nevertheless, only six studies were suitable for the meta-analysis.
With a high quality of evidence (Table 4), the overall findings revealed that MCE alone proved to be uneffective for PGP in terms of pain reduction compared to MSKTs; yet, these MCE were demonstrated to be slightly effective in terms of disability reduction at short-term. These results are similar to those from recent studies which did not conclude on the effectiveness of MCE on PGP, whereas they were effective on LBP [51, 52]. However, the combination of MCE with other MSKTs was found to be more effective than the MSKTs alone in reducing pain and disability at short-term with a strong evidence.
For qualitative analysis, three studies [10, 41, 44] evaluating the effectiveness of MCE combined with other MSKTs at long-term exhibited a PEDro score ranging from 4 to 6/10. Consequently, evidence level in favour of intervention group was considered to be only moderate. Nevertheless, evidence at short-term was revealed to be conflicting [10, 42, 43, 44].
Regarding methodological consideration, the majority of studies were shown to be of moderate quality, as based on their PEDro score, with most of them failing to blind the participants, therapists, and assessors. This, however, is very difficult to avoid in physical therapy unless participants and therapists are both naive to the treatment [10, 23, 39, 40, 41, 42, 45].
Evidence quality of the meta-analysis
Evidence quality of the meta-analysis
Footnotes
Conflict of interest
None to report.
Author contributions
Concept development (provided idea for the research): JM and GN; Design (planned the methods to generate the results): JM and GN; Supervision (provided oversight, responsible for organization and implementation, writing of the manuscript): BH and PM; Data collection/processing (responsible for experiments, patient management, organization, or reporting data): JM and GN; Analysis/interpretation (responsible for statistical analysis, evaluation, and presentation of the results): JM and GN; Literature search (performed the literature search): JM and GN; Writing (responsible for writing a substantive part of the manuscript): JM and GN; Critical review (revised manuscript for intellectual content, this does not relate to spelling and grammar checking): BH and PM.