
Abstract
Proton pump inhibitors (PPIs) are among the most common classes of medications prescribed. Though they were previously thought of as safe, recent literature has shown risks associated with their use including increased risk for Clostridium difficile infection, pneumonia, and fractures. Due to these risks, it is important to determine if PPIs are being used appropriately. This review evaluates seven studies in hospitalized patients. Additionally, this review evaluates literature pertaining to recently discovered adverse reactions; all studies found PPIs are being overutilized. Findings highlight the importance of evaluating appropriate therapy with these agents and recommending discontinuation if a proper indication does not exist.
Introduction
Proton pump inhibitors (PPIs) have become one of the most commonly prescribed drug classes with annual expenditures in 2009 estimated at US $13.5 billion in the United States and US $24 billion worldwide. 1 Several PPIs are currently approved by the US Food and Drug Administration (FDA) for disease states such as gastric or duodenal ulcer, erosive esophagitis, and gastroesophageal reflux disease (GERD).2–6 Additionally, current guidelines suggest the use of PPIs for the following reasons: preventing ulcer complications related to use of nonsteroidal anti-inflammatory drugs (NSAIDs), managing gastroesophageal reflux disease and ulcer bleeding, prophylaxis of stress ulcers, and preventing gastrointestinal risks in patients receiving anticoagulation.7–11 The maximum recommended treatment duration for many of these indications is 4 to 8 weeks. In order to prevent prolonged inappropriate use, evaluation of symptom resolution and need for continued therapy should be performed. Despite treatment recommendations, several studies from countries outside of the United States have shown that PPIs are often excessively and inappropriately used in the inpatient setting.12–15
PPIs have been generally regarded as safe, with the most common adverse reactions being headache, abdominal pain, nausea, diarrhea, vomiting, and flatulence.2-6,16 This perceived safety and tolerability has most likely contributed to their increased use and potential overuse. Alarmingly, more recent evidence has suggested that PPI use is not as benign as originally believed. In fact, studies have linked PPI use with more serious adverse effects such as increased risk of Clostridium difficile (C. difficile) infections, community-acquired and hospital-acquired pneumonia, and osteoporotic fracture, including hip fracture. 17 In addition to adverse reactions, risks with PPI therapy also include drug-drug interactions and drug-nutrient interactions, which may lead to vitamin deficiencies. A drug interaction with clopidogrel has been described, however, the clinical significance of this interaction is questionable. Other common drug-nutrient interactions include reduced absorption of calcium, iron, and vitamin B12. 17
Due to increasing reports of potentially serious adverse effects and drug-drug interactions, the possible widespread use of PPI in hospitalized patients requires further examination. The purpose of this review was to evaluate the appropriateness of use with PPIs in hospitalized general medical patients in the United States and outline potential consequences associated with the use of PPIs.
Methods
A literature search was conducted using MEDLINE® (1946 to July, week 3, 2012) and EMBASE® (1980 to 2012, week 29). Keywords and Medical Subject Headings (MeSH) used include proton pump inhibitors and hospitalization. Results were limited to studies conducted in adult subjects and published in the English language. Studies were selected for inclusion if they evaluated the use of proton pump inhibitors in the general medical inpatient population in the United States. Studies were also only included if the majority of patients in the study were taking a PPI (versus a histamine2 receptor antagonist). Studies were excluded if they were conducted outside of the United States, or if they studied only patients in the critical care setting. References of selected articles, review articles, and treatment guidelines were also examined for pertinent articles.
Mechanism of Action, Metabolism, and Pharmacokinetic Profile
PPIs are absorbed in the proximal small bowel and achieve peak concentrations of approximately 0.5 to 2 mg/mL. 18 All PPIs undergo low rates of hepatic first-pass metabolism and thus have high oral bioavailability; oral bioavailability ranges from 77% for pantoprazole to 90% for lansoprazole. 18 PPIs are highly protein bound, with each binding 95% or greater. Though PPIs are known to inhibit acid secretion for up to 36 hours, their elimination half-life is short, ranging from 30 minutes to 2 hours. 19
The mechanism of action of PPIs leads to a reduction in gastric acid production via the adenosine triphosphateases (H+, K+-ATPase) pumps, which are responsible for the regulation of gastric pH. PPIs selectively and irreversibly bind to H+, K+-ATPase pumps, also referred to as proton pumps, inhibiting both basal and stimulated secretion of gastric acid. 19
PPIs are metabolized primarily through the cytochrome P450 (CYP) enzymes 2C19 and 3A4. Though all PPIs utilize the CYP system, it should be noted that there are differences in the extent to which their degradation depends on the given CYP. 18 For example, only a small percentage of rabeprazole utilizes CYP2C19 and CYP3A4 for metabolism. Further, omeprazole, esomeprazole, and pantoprazole predominantly rely on CYP2C19 for metabolism, lansoprazole significantly relies on both CYP2C19 and CYP3A4.
Clinical Studies
Studies Evaluating Overuse of PPI Therapy Only
There are two published studies evaluating the sole use of PPIs in the hospitalized setting. The first of these studies was conducted by Reid et al as a retrospective review from two databases from university-affiliated hospitals in Colorado (Table 1). 20 This study was conducted in randomly selected adult patients aged 18 to 90 years admitted for medical services. Appropriateness of PPI therapy was determined using International Classification of Diseases, 9th Revision (ICD-9) codes. Interestingly, results from the evaluation of both databases found that 40% of patients in one database and 14% of patients in the other were prescribed PPIs during hospitalization. Of those that were prescribed PPI therapy, 39% and 27% of patients in these databases, respectively, were classified as having valid indications for PPI use. A random chart review of 5% of patients indicated that utilization of ICD-9 codes may be inaccurate and revealed a 19% error rate. Adjusting the data according to this administrative error rate resulted in >50% failing to meet proper indications for PPI therapy. Further, safety information was also collected, and patients receiving PPIs in both database populations had a higher rate of concurrent C. difficile infection: 1.16% in the PPI population versus 0.44% in the non-PPI group in one database and 1.32% versus 0.003%, respectively, in the second database (P < 0.001). Increased concurrent diagnosis of pneumonia was significantly greater in one population (8.2% in the PPI group versus 5.3% in the non-PPI group; P < 0.001) and a trend toward significance in the other population (10.1% in the PPI group and 8.7% in the non-PPI group; P = 0.023). After correction using the Bonferroni method, a P value < 0.01 was deemed statistically significant. The results of this study indicate that there is overuse of PPI in hospitalized patients. However, investigators utilized retrospective chart review, which led to a self-reported administrative error rate of 19%. This may have originated from the use of ICD-9 codes to determine appropriateness of therapy, as ICD-9 codes tend to have high specificity but low sensitivity in capturing all inpatient diagnoses. Further, the data on overutilization of PPI from the two databases were drastically different despite similar methods employed, bringing into question the accuracy of these findings.
Studies evaluating the use of proton pump inhibitors in hospitalized adult patients.
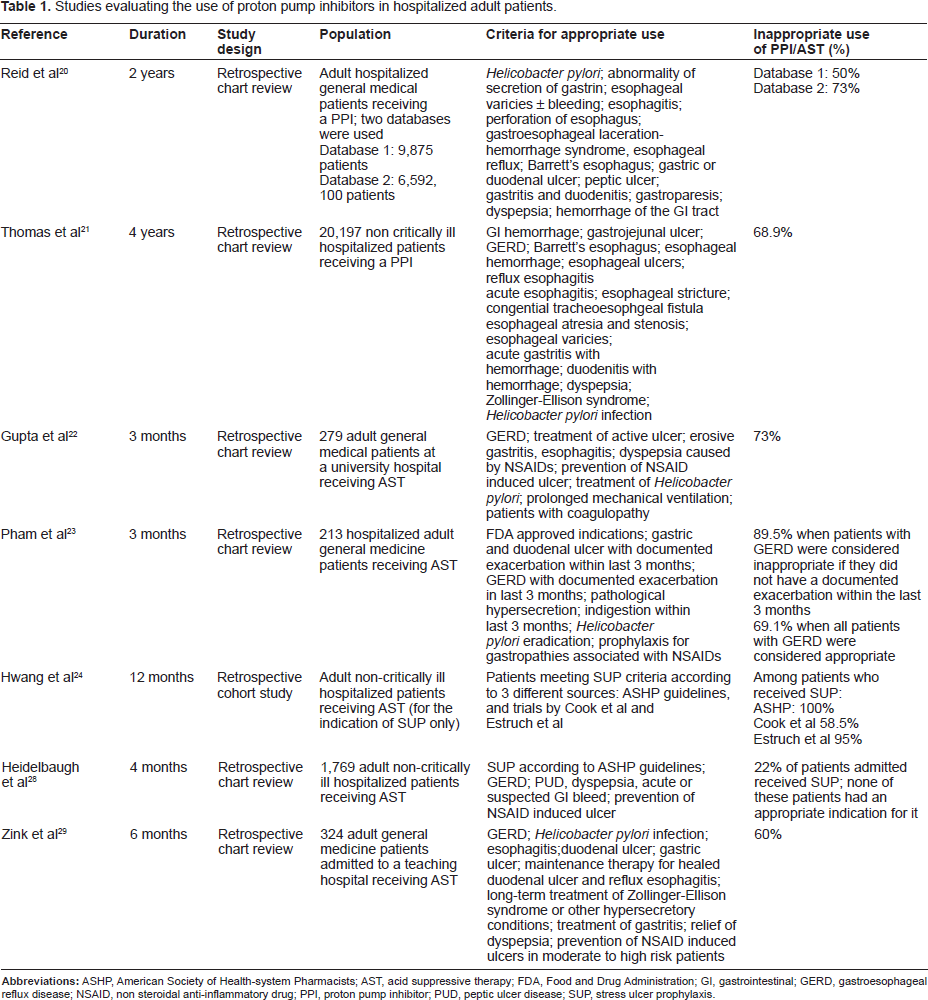
A study conducted by Thomas et al evaluated appropriate initiation of PPIs during hospitalization using ICD-9 codes (Table 1). 21 The investigators also evaluated the cost associated with inappropriate prescribing of PPI therapy in hospitalized, non–critically ill patients using medical and pharmacy claims from a large managed care database. Information was gathered through claims based on “place of service” field to only include information from inpatient claims. PPI therapy was only considered appropriate if the patient was using PPI therapy prior to hospitalization or if use was consistent with diagnoses. A total of 20,197 (68.8%) patients were categorized as inappropriate users of PPI therapy. When comparing critically ill patients versus medical patients, there was no statistically significant difference found with respect to inappropriate use (68.7% and 68.9%, respectively). Evaluation of PPI overuse was conducted continuously over 4 years; overuse of PPIs decreased slightly during this time. However, there was no significant difference over time. Similar to the study by Reid et al, concerns regarding the accuracy of results may have been limited by the retrospective nature of the design of this study. Additionally, miscoding or inaccurate diagnosis was likely given that there is no ICD-9 code for stress ulcer prophylaxis (SUP). Authors may not have accounted for potential inaccuracies in findings when using ICD-9 codes; however, the findings reported are significant and cannot be overlooked.
In addition to the two previous studies that examined the use of PPIs, several other studies included patients who were taking PPIs as well as those taking other acid suppressive therapy. For the purposes of this review, studies were only included if the majority of patients were taking a PPI.
Gupta et al looked at the frequency with which inappropriate administration of acid suppressive therapy (AST) (either a histamine-2 receptor antagonist [H2RA] or a PPI) occurred during hospital admission and at hospital discharge (Table 1). 22 Patients admitted to the general medicine unit of a university hospital and who received at least one dose of AST were eligible for the study. Patients were excluded if they were transferred from the intensive care unit (ICU) or had been prescribed AST prior to admission. Two hundred and seventy-nine patients were randomly selected over a 3-month period and included in this retrospective chart review. Indications that were considered appropriate included any FDA approved indication as well as any indication supported by current guidelines. The population evaluated had an average length of stay of 6.3 days, were mostly male (60%), and were mostly African Americans (55% versus 39% Caucasians). PPIs were the most commonly prescribed AST. Appropriate use was identified in 27% of patients who were prescribed an AST upon admission to hospital. The most common reasons for prescribing AST was stress ulcer prophylaxis in low risk patients and prophylaxis of ulcer in patients taking corticosteroids or anticoagulants. Of those who were inappropriately initiated on AST, 69% were discharged on this therapy. Patients initiated on AST for anemia or for an unknown cause were less likely to be discharged on AST. Low risk patients started on AST for stress ulcer prophylaxis and patients started on AST for prevention of corticosteroid or anticoagulation induced ulcer were just as likely or more likely to be discharged on these agents inappropriately compared with other indications that were considered inappropriate. Age, admitting diagnosis, and mean length of stay did not predict discontinuation of AST. Investigators of this review determined that a sample size of 246 patients was needed to detect a difference with a 95% confidence level. Data were gathered on 279 patients, and, therefore, the review was powered sufficiently. Although this study was performed at a single center, investigators noted that 35 prescribers were identified during data collection thereby minimizing the potential for bias. A high percentage of inappropriate use, both in the inpatient and outpatient setting, occurred in this review. Overuse in the inpatient setting may have been overestimated due to the fact that patients were included even if they only received one dose. Conversely, the prevalence of inappropriate use may have been underestimated since patients who were admitted on AST were not included in the analysis. Presumably, some of these patients may have lacked an appropriate diagnosis for PPI use or justification for continued use. Additionally, patients were excluded if they were transferred from the ICU, which is where AST for SUP is most often indicated. Had these patients been included, inappropriate continuation of SUP may have been seen. Inappropriate continuation upon discharge occurred at a high rate, which illustrates the need for more thorough medication reconciliation prior to discharge.
Pham et al conducted a retrospective chart review of 213 patients admitted to a university hospital general medicine service over a 3-month period (Table 1). 23 The purpose of the review was to identify the indications and prevalence of AST with PPIs and H2RAs at admission and upon discharge. Similar to the study conducted by Gupta et al, appropriate indications included those that are FDA-approved or those supported by medical literature. Investigators decided that since the recommended maximum duration of therapy for most indications is 4 to 8 weeks, treatment duration of greater than 3 months without documented evidence of disease continuation would be considered inappropriate. Investigators did, however, acknowledge that patients being treated for GERD often require treatment for a longer period of time, and so, upon analysis, patients receiving long-term treatment for GERD were included in the evaluation in two different ways: (1) as being treated appropriately and (2) as being treated inappropriately (that is, where there was no documented evidence of active disease). Eight-four percent of patients included in the review were taking a PPI for AST. The mean length of stay was 3 days, 52% of patients were female, and 80% were Caucasian. This study found that when the therapy for patients treated for GERD who have not had an exacerbation in the last 3 months was considered inappropriate, AST was considered acceptable in only 10.5% of the evaluated population. When it was assumed that all GERD patients were appropriately treated, 30.9% of patients had an acceptable indication. The most common unacceptable indications included use for prophylaxis of a corticosteroid-induced ulcer and stress ulcer prophylaxis in low risk patients. Other common unacceptable indications included a history of peptic ulcer disease (PUD), GERD, or GI bleed with no evidence of disease in the past 3 months. Fifty-four percent of patients were discharged on AST. Of these, 27% of patients had an acceptable indication; this was with the assumption that all patients with GERD were continued appropriately. PPIs were the most common AST that patients were discharged on. This review also demonstrated a high rate of inappropriate use, especially when duration of therapy was taken into consideration. As with other retrospective reviews, this review was limited by assuming complete documentation in the patients' medical records; in some cases, patients may have had an undocumented justification for therapy or continued therapy. This is particularly true for those receiving AST for GERD; it would be difficult to determine if patients were taking therapy intermittently or were refractory to previous treatment. It is, therefore, possible to have an overestimation of inappropriate use.
A retrospective cohort study was conducted in non–critically ill patients admitted to a medical teaching service to assess appropriateness of AST to prevent stress ulcers (Table 1). 24 All patients who were initially admitted to the critical care unit and subsequently transferred to the general ward were included in the study. Patients were excluded if they were admitted for less than 2 days or they were admitted with a diagnosis or suspicion of gastrointestinal bleeding. AST medications were defined as PPIs, H2-receptor antagonists, antacids, and cytoprotective agents, and SUP was defined as acid-suppressive medication given to prevent stress ulcer bleeding in the absence of current evidence for bleeding. SUP was most commonly given as a PPI (80.9%), followed by H2-receptor antagonists (20.1%), antacids (1%), and sucralfate (0.7%). Note that the total exceeds 100% due to some patients receiving multiple medications. If no reason was given for AST, it was categorized as SUP. Due to clinical controversy surrounding appropriate treatment of SUP, the authors used three different methods of evaluating appropriateness of therapy for SUP. The first included the guideline statement from the American Society of Health-System Pharmacists (ASHP), which recommended against SUP in non–critically ill patients. 25 ASHP guidelines were published in 1999 and provide specific recommendations for prevention of stress ulcers, which are defined as lesions involving the mucosal layer of the stomach that occur after events that induce stress on patients, such as surgery or trauma. The other methods used were based on two additional published studies, one randomized trial and one prospective cohort study, each of which was performed to identify risk factors for stress ulcer.26,27 Risk factors requiring SUP identitified by Estruch et al included respiratory failure, sepsis, heart failure, hepatic encephalopathy, jaundice, renal failure, stroke, hypotension, previous gastrointestinal disease, and treatment with corticosteroids, NSAIDs, heparin or warfarin. 26 Risk factors indicating SUP in the study by Cook et al included prolonged mechanical ventilation or coagulopathy. 26 A total of 545 patients were included in the study by Hwang et al. The most common risk factor for SUP was the use of NSAIDs or aspirin, and this was present in 42.6% of patients. A total of 54.9% of patients received AST for SUP and, of that percentage, 37.7% of patients had no risk factors for stress ulcer. Appropriateness of SUP therapy varied depending on the criteria used. Based on the criteria by Cook et al, 58.5% of patients receiving AST for SUP was deemed inappropriate. According to the ASHP criteria, non–critically ill patients should not receive AST for SUP, and, thus, 100% of patients were considered to have received inappropriate SUP treatment. When using the Estruch et al criteria, 95% of patients received inappropriate SUP. Limitations of this study include a patient population that only included those transferred out of the ICU and a potential for overestimation of inappropriate use since patients lacking an indication were categorized as SUP. Additionally, since stress ulcer prophylaxis is most commonly indicated in ICU patients, a higher rate of inappropriate use could have been observed because patients may have continued on SUP following transfer out of the ICU. The high percentage of inappropriate use does highlight the need for closer medication reconciliation upon transfer from the ICU. It should also be noted that this study was conducted in a teaching hospital, and documentation of the prescriber (physicians, resident, or attending physician) was not performed. This would have been important to document as part of the learning experience for resident physicians.
Heidelbaugh et al conducted a retrospective chart review at a large university hospital on adult non–ICU patients to assess the practice of prescribing SUP (Table 1). 28 ASHP guidelines were used to define appropriateness of SUP. Patients treated with an H2RA or a PPI were included; those taking AST for an approved GI diagnosis (GERD, PUD, or active GI bleed) were assumed to not be taking it for SUP. During the study period, 1769 patient admissions occurred. Thirty-three percent (n = 585) of patients were taking AST prior to admission, and, of those, 74% (n = 433) had an appropriate diagnosis for this therapy. In 22.1% (n = 391) of patient admissions, SUP was listed as the reason for prescribing AST. Of the 391 patient admissions prescribed SUP, no patient met the criteria for SUP according to the guidelines. The most commonly used medication was a PPI (89.4%) followed by an H2RA (8.3%). Fifty-four percent of those who were inappropriately prescribed AST for SUP were discharged on a prescription for AST. Of note, there was no documented occurrence of stress ulcer in any of the patients in the study, including those who were not prescribed AST. In this study, a large number of patients were assessed at one hospital. Although the number of patients in the study was large, the authors failed to mention the number of prescribers involved, which would have been helpful to rule out bias. The authors did specify, however, that there were no prescribing differences between admitting specialties. Similar to the other reviews, one limitation is a potential for the lack of a documented indication in a patient's chart, which may have led to overestimating the occurrence of inappropriate use. Additionally, it was assumed that if the patient had a documented indication, they had been treated appropriately, but the authors did not account for any therapy that may have exceeded the recommended maximum duration and would have been no longer necessary.
Zink et al performed a retrospective chart review of general medical patients admitted to a teaching hospital over a 6-month period (Table 1). 29 Patients were included if they received one dose of AST with an H2RA or a PPI. Patients were excluded if they were transferred from the ICU or a medical step-down unit, if they were admitted on AST, readmitted during the study period, or had an appropriate indication for AST. Appropriate indications were again defined as an FDA-approved indication or an indication supported by medical literature. Three hundred twenty-four patients met the inclusion criteria for review. Of those, 40% (n = 128) were initiated on AST for an appropriate indication, while 60% (n = 196) were not. Thirty-four percent of patients who did not have an appropriate indication for AST were discharged on the medication. Eight-four percent of patients were discharged on a PPI, while 15% were discharged on a H2RA. Once again, the incidence of inappropriate use in this study may have been affected by inaccurate or lack of documentation of diagnosis in the medical record and the exclusion of certain populations such as patients who spent time in the ICU or those who were admitted on AST. Although the percentage of patients taking a PPI in this study was not given, it is known that 84% of patients were discharged on a PPI and, presumably in most cases, patients were continued on their hospital medication and dose.
Studies Evaluating the Safety of PPIs
PPIs have been generally regarded as safe, but more recently have been associated with serious adverse reactions such as infection with C. difficile, pneumonia, and bone fracture. A meta-analysis of six nested case-control studies found an increased risk of community-acquired pneumonia (CAP) with PPI use. 30 Interestingly, this meta-analysis found an increased risk of CAP with short-term PPI use (OR [odds ratio]1.92, 95% CI 1.40-2.63, P = 0.003), while chronic use was not associated with this risk. Patients receiving PPIs are believed to be at increased risk of pneumonia due to overgrowth of bacteria in the stomach secondary to acid suppression, which increases the risk for microaspiration. PPI use can also inhibit innate and adaptive immunity by suppressing activity of neutrophils, natural killer cells, and T-cells. It is suggested that over time the body may develop a compensatory mechanism for this suppression, which may explain the higher risk of pneumonia with short-term versus long-term PPI therapy. It is important to note that the authors do not draw definitive conclusions from this meta-analysis because of significant heterogeneity between studies. A second meta-analysis of eight observational studies showed that the overall risk of pneumonia was higher among patients using PPIs (OR 1.27, 95% CI 1.11-1.46). 31 Two additional population-based cohort studies conducted by Laheij and Gulmez also showed an increased risk of CAP with an adjusted relative risk of 1.89 (95% CI 1.36-2.62) and an adjusted odds ratio of 1.5 (95% CI 1.3-1.7), respectively. Gulmez et al also found a greater risk in those patients who had recently (less than 7 days) begun therapy with a PPI (OR 5.0, 95% CI 2.1-11.7).32,33 In addition to CAP, PPIs use may also increase the risk for hospital-acquired pneumonia (HAP), although results are conflicting. A large, prospective cohort study evaluated the use of acid suppressive therapies and risk of HAP in patients outside of the ICU. 34 Investigators found a higher incidence in patients exposed to AST versus those not exposed (4.6% and 2.0%) with an adjusted odds ratio of 1.3 in the exposed group (95% CI 1.1-14, P < 0.05). Conversely, a smaller, retrospective cohort study did not find an association between PPI exposure and development of HAP in ICU patients. 35 There appears to be a larger body of evidence supporting a risk for the development of CAP with PPI use compared with HAP. Although the risk of development of pneumonia is modest, the consequences of pneumonia can be severe.
In addition to increased risks of pneumonia, there have been several studies demonstrating an association of C. difficile associated disease (CDAD) with PPI use. Similar to the presumed pathogenesis of pneumonia in patients taking a PPI, the risk for development of C. difficile is thought to be related to the ability of microbes to survive when the gastric pH is increased. Leonard et al conducted a meta-analysis to determine if an association between the risk of enteric infection and acid suppression exists. 36 Eleven papers were included in the evaluation, which found a statistically significant association between PPI use and CDAD (OR 2.05, 95% CI 1.47-2.85). A secondary analysis was performed on another recent investigation that looked at data from discharges over a 5-year period at a tertiary care medical center. 37 Investigators found a dose-dependent increased risk for CDAD in patients on acid-suppressive therapy with a PPI (OR 1.74, 95% CI 1.39-2.18). The Food and Drug Administration (FDA) has also recently reviewed 28 observational studies, 23 of which showed an association between PPI use and increased risk of CDAD. 38 Although the strength of association in these trials was mixed, most studies found the risk of CDAD was 1.4 to 2.75 times higher in patients with exposure to PPIs compared with those with no exposure. Once again, the risk for development of CDAD may be modest; however, the consequences of infection can be severe, and treatment can be costly.
PPI use has also been associated with increased risk of fracture. However, data on this association are conflicting. The mechanism is thought to be due to the ability of PPIs to cause calcium malabsorption. A nested case-control study found an increased risk of hip fracture in community patients on PPI therapy, particularly with long-term high-dose therapy. 39 This risk was greater with increasing duration of therapy (adjusted OR for 1 year, 1.22; 2 years, 1.41; 3 years, 1.54; and 4 years, 1.59; P < 0.001). Similarly, a retrospective cohort study found an increased risk of an osteoporosis related fracture after 7 or more years of PPI exposure (adjusted OR 1.92, 95% CI 1.16-3.18, P = 0.01) and an increased risk of hip fracture after 5 or more years of PPI exposure (adjusted OR 1.62, 95% CI 1.02-2.58, P = 0.04). The risk of hip fracture was even higher after 7 or more years of PPI exposure (adjusted OR 4.55, 95% CI 1.68-12.29, P = 0.002). 40 Another case-control study found a small but significant association between PPI use within the last year and increased risk of any osteoporotic fracture (OR 1.18, 95% CI 1.12-1.43). 41 However, a prospective analysis of 130,487 postmenopausal women found no association between PPI use and hip fracture. 42 The study did, however, find with PPI use an increased risk of clinical spine fracture (adjusted HR [hazard ratio] 1.47, 95% CI 1.18-1.82), forearm or wrist fracture (adjusted HR 1.26, 95% CI 1.05-1.51), and total fractures (adjusted HR1.25, 95% CI 1.15-1.36). Results from these studies suggest that long-term PPI use may increase risk of osteoporotic fracture. Although these data may not be relevant to the short-term use in the hospital setting, they may have implications for cases in which a PPI is continued unnecessarily upon discharge. As with the risk of CDAD and pneumonia, the risk of osteoporotic fracture is modest; however, when fractures occur, most notably hip fractures, they are associated with substantial cost as well as morbidity and mortality.
In addition to the discovery of more severe adverse effects, serious drug-drug and drug-nutrient interactions have surfaced. Clopidogrel is a potent antiplatelet agent used in the treatment of acute coronary syndrome, recent myocardial infarction, recent stroke, or established peripheral arterial disease. Some experts recommend that PPIs be prescribed to patients taking clopidogrel in order to reduce the risk of gastrointestinal bleeding. 10 Recently, a drug interaction has come to light due to the fact that some PPIs inhibit CYP2C19, which is the enzyme responsible for metabolizing clopidogrel to its active form. 43 Inhibition of this enzyme reduces the concentration of the active form of clopidogrel and thus theoretically places patients at higher risk for cardiovascular events. The clinical significance of this interaction has been examined by many large trials and observational cohort studies. Data concerning the interaction are conflicting and a consensus is not provided on the management of this interaction.44–50 The COGENT trial is the only trial that has evaluated the safety of clopidogrel alone versus clopidogrel in addition to a PPI. 45 Bhatt et al discovered that use of omeprazole with clopidogrel did not increase the risk of cardiovascular events and adding omeprazole did decrease the risk of gastrointestinal bleeds associated with clopidogrel. Several limitations to this trial exist including the fact that it was sponsored by industry and it ended prematurely as a result of bankruptcy of the company. Due to early termination, the study did not meet its statistical targets and thus may not have been powered appropriately. Pantoprazole has weaker effects on CYP2C19 and may be the preferred PPI in patients taking clopidogrel. 51 Alternatively, prasugrel, another antiplatelet agent similar to clopidogrel, may be used. Prasugrel is not extensively metabolized via CYP2C19, avoiding the potential drug interaction.
Reduced absorption of calcium, iron, and vitamin B12 may also occur in patients taking PPI therapy. 52 Absorption of vitamin B12 may be decreased due to the ability of PPIs to inhibit the synthesis of intrinsic factor in parietal cells. Vitamin B12 must bind to intrinsic factor to be absorbed in the ileum. An acidic environment is also required for iron absorption to occur; gastric acid must reduce ferric iron to the more soluble ferrous form. 1 Calcium carbonate is another vitamin requiring an acidic environment for absorption. 53 Calcium citrate is an alternative form of calcium that is not as sensitive to gastric acidity and is preferred in patients with achlorhydia or those on AST. 54 It is also important to consider that certain drugs such as ketoconazole, itraconazole, sucralfate, indinavir, didanosine, midazolam, and methadone also require an acidic environment for absorption and may also be affected by the use concomitant of a PPI.1,44
Efficacy
The most potent inhibitors of gastric acid secretion are PPIs. 55 All PPIs are similarly effective for approved indications when used in equipotent doses. Some studies suggest that esomeprazole and rabeprazole inhibit gastric acid secretion more rapidly, which may be associated with faster symptom relief. 55 PPIs are considered superior to other ASTs with regard to efficacy, but do not demonstrate improvement in mortality. 56
Discussion
Inappropriate use of acid suppression therapy has been consistently demonstrated in the inpatient general medical population. Many of the reviews discussed here identify SUP as a common reason for inappropriate therapy. Current stress ulcer prophylaxis guidelines recommend AST with an H2RA, an antacid, or sucralfate for patients who are at high risk of developing a stress ulcer (PPIs are not recommended in these guidelines due to lack of efficacy and safety data at the time of publication). 25 Patients who meet these criteria include those who require mechanical ventilation for greater than 48 hours, those with coagulopathy, those who have a history of GI ulceration or bleeding within the past year, and those who have two or more of the following risk factors: sepsis, ICU stay greater than 1 week, occult bleeding > 6 days, or use of high dose corticosteroids defined as a daily dose of, or equivalent to, 250 mg of hydrocortisone. As presented at the 2012 Society of Critical Care Medicine Annual Congress, updated guidelines for stress ulcer prophylaxis are due out at the end of this year. It is expected that H2RAs will be recommended as first line therapy and that the use of PPIs will be reserved for those who have failed or cannot tolerate a H2RA, those with a GI bleed, or those with another indication for a PPI. Guidelines for the prevention of stress ulcer in non–ICU patients have yet to be defined, and current medical lliterature does not support the routine use of AST with PPIs. 25 Inappropriate use of AST in the studies described above ranged from 25% to 70%, and although most studies considered both H2RA and PPI use, the majority of patients in the studies were found to have been taking a PPI. Further, some of these studies also showed inappropriate continuation of PPI upon discharge.28,44,57,58 Both inappropriate use and inappropriate continuation of AST upon discharge put patients at risk for adverse events and drug interactions.
Increased cost associated with use of AST is also a concern. The previously discussed study conducted by Heidelbaugh et al looked at the economic impact of inappropriate use of SUP in non–ICU patients and found that the annual cost of providing SUP to this population at their facility was US $44,096, and, furthermore, outpatient prescriptions in this population were associated with an annual cost of US $67,695. 28 Additionally, results of the Thomas et al study evaluating overuse of PPI in hospitalized patients found a considerable increase in cost to both the managed care organization and to patients through co-pays or co-insurance after discharge. A total of US $3,013,069 was incurred through the 4 years the study was conducted. 44
Several studies have demonstrated that implementation of institution-specific SUP guidelines or protocols, and/or educational interventions can reduce the incidence of inappropriate use.59–61 Although these strategies may reduce inappropriate SUP, they do not reduce the incidence of inappropriate continuation of AST upon admission in instances such as the lack of an appropriate medical diagnosis or justification for continued use.
The studies discussed in this review all have similar limitations. For example, all were retrospective reviews relying on complete and accurate documentation in the patient's medical record. Patients may have had an appropriate indication without complete documentation, which may have led to inflated rates of inappropriate use. Additionally, patient recall, if relied upon for a current medication list, may have biased the information in the medical record leading to inaccurate estimations. This is especially true considering that many PPIs are available over the counter and patients can practice self-care without consulting their primary care physician. It is also important to note that the potential benefits of SUP in the general medical population are not known at this time; future medical literature may prove the benefit of SUP in this population. Regardless of these limitations, the rate of inappropriate use of PPIs in hospitalized patients remains high.
Conclusion
Several studies have demonstrated high rates of inappropriate use of PPIs and other acid suppressing agents in the inpatient setting. Until benefit of SUP in general medical patients is demonstrated, use of PPIs for SUP should be avoided in this population. Additionally, for those patients who are taking a PPI at home, appropriateness of continuation of PPI therapy upon admission should be determined in order to decrease cost and decrease potential for serious adverse reactions and drug interactions. Interventions such as educational programs and/or institution-specific guidelines for use may be developed and implemented to help decrease the use of PPIs in the inpatient population.
Author Contributions
Conceived and designed the experiments: CD, KW, AD. Wrote the first draft of the manuscript: CD, KW, AD. Contributed to the writing of the manuscript: CD, KW, AD. Agree with manuscript results and conclusions: CD, KW, AD. Jointly developed the structure and arguments for the paper: CD, KW, AD. Made critical revisions and approved final version: CD, KW, AD. All authors reviewed and approved the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest. Provenance: the authors were invited to submit this paper.