
Abstract
Background:
Critically ill patients with moderate-to-severe physiologically stressful event are at high risk of developing stress ulcers. The use of pharmacological prophylaxis significantly reduces the incidence of stress ulcer in high-risk patients.
Objective:
The aim of this study was to assess the use of pharmacological prophylaxis for stress ulcer in the medical wards of University of Gondar Hospital.
Methods:
A cross-sectional study design was used. In total, 234 patients were selected through simple random sampling technique. The risk of stress ulcer development was assessed using Evidence-Based Medicine Guideline for stress ulcer prepared by Orlando Regional Medical Center. SPSS version 21 was used for data analysis.
Result:
The most common acute risk factor to stress ulcer was coagulopathy (18.4%), followed by hypoperfusion (9.8%). The concomitant non-steroidal anti-inflammatory drug use (16.7%), mild-to-moderate brain or spinal cord injury (11.1%), and concomitant or recent corticosteroid use (9.4%) were frequently seen risk factors that necessitate administration of a prophylaxis. In total, 82 (35%) study participants were given stress ulcer prophylaxis, among which 52 (63.4%) were given without indication. The most commonly used drug class in the prevention of stress ulcer was proton pump inhibitors (76/82, 92.7%). In total, 43 (18.4%) study subjects were not given stress ulcer prophylaxis while there was clear indication. Patients with a long hospital stay and a diagnosis of central nervous system disorders had significant risk for inappropriate stress ulcer prophylaxis use.
Conclusion:
In this study, inappropriate use of prophylaxis for stress ulcer was common. The higher proportion of inappropriateness was due to the use of stress ulcer prophylaxis while there was no enough indication. We recommend future researchers to assess the cost and impact of inappropriate stress ulcer prophylaxis use, and the physicians should be adherent to the standard guidelines.
Introduction
Stress ulcer is a form of hemorrhagic gastritis that can happen in critically ill patients who have suffered a moderate-to-severe physiologically stressful event. The pathogenesis is multifactorial including acid hyper-secretion, epithelial turnover in the gastric mucosa, and altered secretion of mucus and bicarbonate.1,2 Potential risk factors for stress ulcer–associated bleeding are taking drugs that increase the risk of bleeding, having a history of peptic ulcer or upper gastrointestinal (GI) bleeding, undergoing high-risk surgery, burns over 35% of the total body surface, head or spinal trauma, severe sepsis, hypotension, peritonitis, organ failure, respiratory failure requiring more than 48 h of mechanical ventilation, and coagulopathy.1,3–7
The frequency of acute GI ulceration and bleeding increased with the number of risk factors existing. 7 In critically ill patients, the risk of ulcer-related evident bleeding is estimated to be 5%–25%, while in inpatients who are not critically ill, the risk of overt bleeding from stress ulcers is less than 1%. 8
Clinically important GI bleeding may cause hemodynamic instability or require red blood cell transfusion. The attendant risks of transfusion include infection and potential for immunosuppression, as well as possible blood-related incompatibilities.7,9 In addition, there is a potential for an increased length of stay in the hospital and increased mortality. 10
Prophylaxis against stress ulcers can significantly minimize bleeding, but such therapy may be costly and can have adverse effects, including interactions with other drugs and foods, that preclude using it routinely for all hospitalized patients. Thus, it is important to ascertain risk factors that would confirm the need for prophylaxis and target interventions to those at highest risk. Because it is possible to identify patients who are at the highest risk for bleeding, strategies should rationally focus on the prevention of stress ulcer and bleeding, rather than on its treatment. Such an approach may minimize complications associated with stress ulcer and improve outcomes.5,7
Thus, prevention of acid injury and stress ulcer might be achieved by therapies that decrease acid secretion or enhance protective mechanisms. 7 Proton pump inhibitors (PPIs) and histamine2-receptor antagonist (H2RAs) are the most frequently utilized pharmacological prophylactic therapies for stress ulcer prevention. Sucralfate and antacids are seldom used.2,6,11 Compared to antacids and sucralfate, PPIs and H2RAs tend to be better tolerated and are easily administered. 11
When indicated, PPIs are well tolerated and considered superior in the treatment of acid-related conditions such as peptic ulcer disease. In addition, PPIs are more effective at keeping a constant gastric pH > 4.0, which may be sufficient to prevent stress ulcer, compared to H2RAs.12,13 As a result, PPIs are being increasingly used. 14 However, no difference was reported between PPIs and H2RAs in terms of mortality rate or reduction in the incidence of nosocomial pneumonia.5,15
Worldwide, clinicians administer stress ulcer prophylaxis (SUP) for 80%–90% of critically ill and injured patients, and prescriptions for acid suppressants in less severely ill patients are prevalent. 16 Accordingly, inappropriate PPI usage has raised concerns and is associated with increase in the healthcare costs and adverse drug reactions. 17
To the extent of our knowledge, there is no study so far that assessed the use of SUP in Ethiopia. Therefore, the aim of this study was to assess the use of pharmacologic prophylaxis against stress ulcer in hospitalized medical patients in an Ethiopian teaching hospital.
Methods
Study area and period
This study was conducted at the medical wards of University of Gondar Hospital, Gondar, Ethiopia. Gondar is found 727 km away from Addis Ababa in the north-west direction. The hospital serves for more than 4 million people in the region. It has more than 460 beds and delivers service in internal medicine, pediatrics, gynecology, ophthalmology, psychiatry, surgery, and other departments. The medical ward consists of three separate wards having an average of 30 beds each. All the three wards serve non-ICU (intensive care unit) medical patients. The study was conducted from 1 July to 30 September 2017.
Study design and subjects
Cross-sectional study design was used to assess appropriateness of SUP use in the medical wards of University of Gondar Hospital. Patients who have an indication for treatment with acid suppressive therapy (AST), such as duodenal ulcer disease and gastro-esophageal disease, were excluded from the study. Patients under 18 years old were also excluded. Single population proportion formula was used to calculate the sample size by taking the following assumptions: proportion of appropriate SUP use = 0.5, margin of error = 5%, and 95% confidence interval

Correction formula was applied as the source population was less than 10,000 (total population of patients in 3 months (N) = 599)

Finally, 234 patients were selected by simple random sampling technique.
Data collection and management
The data collection tool was developed by the authors after reviewing studies done on the topic.17–20 The tool contains information related to socio-demographic and clinical characteristics of study subjects, risk factors for developing stress-related ulcer, drugs prescribed for prevention of stress ulcer, and the rationality of SUP. The data collection tool was pretested on 5% of the sample population. Data were collected through review of patients’ medical charts by trained data collectors (research assistants). The risk of stress ulcer development was assessed using Evidence-Based Medicine Guideline for stress ulcer prepared by Orlando Regional Medical Center (ORMC). 20 According to the guideline, SUP is indicated in patients with at least one acute risk factor or patients who are nothing by mouth (NPO) and have at least two potential risk factors for stress ulcer. Acute risk factors for stress ulcer are mechanical ventilation (>48 h), coagulopathy, hypoperfusion (sepsis, shock, or organ dysfunction, that is, acute renal failure), high-dose corticosteroids (>250 mg/day hydrocortisone or equivalent), significant burn injury (total body surface area > 35%), and severe brain/spinal cord injury (Glasgow Coma Scale ⩽ 8). The potential risk factors for stress ulcer are concomitant use of a non-steroidal anti-inflammatory drug (NSAID), concomitant or recent corticosteroid use, history of upper GI hemorrhage, peptic ulcer disease, or gastritis, and mild-to-moderate brain/spinal cord injury. The data were collected by two pharmacists who were trained on the procedures of data collection. The completeness and accuracy of the collected data were checked on daily basis. SUP use was considered as appropriate if the patient has an indication for it and prescribed with an acid suppressing agent or if there is no indication for SUP and no acid suppressing agent was prescribed, otherwise it is labeled as inappropriate.
Data analysis
Data was checked for its completeness, coded, and entered into the Epinfo version 7 software. Then, it was exported to SPSS (version 21) (IBM Corporation, Armonk, NY, USA) for analysis. Descriptive statistics (mean values, standard deviations, and medians) was done and results were presented in tables. Categorical variables were presented in numbers and percentages. Continuous variables are presented as mean ± standard deviation. A test of association was done using univariate binary logistic regression to get the crude odds ratio (COR) and multivariate binary logistic regression to get the adjusted odds ratio (AOR). All the statistical tests were significant at p-value less than 0.05.
Ethical considerations
The study was commenced after ethical clearance was secured from the Ethical Review Committee of School of Pharmacy, University of Gondar. The hospital medical director was officially communicated and permission was granted. In order to maintain confidentiality, any personally identifiable information (e.g. name and address) was not recorded on the data collection format.
Result
Among 234 patients included in this study, 112 (47.9%) were below 40 years old, more than half, 124 (53%), were female, and 106 (45.3%) stayed in the hospital for more than a week. The mean age of study subjects was 43.3 ± 18.0 years. The median duration of hospital stay was 7 days. Infectious and cardiovascular diseases were the most common diagnosis recorded in the 62.8% and 44% of study participants, respectively. The detailed description of characteristics of study participants is given in Table 1.
Socio-demographic and clinical characteristics.

Cancer, arthritis, trauma, chronic obstructive pulmonary disease (COPD), anemia, schizophrenia, and asthma.
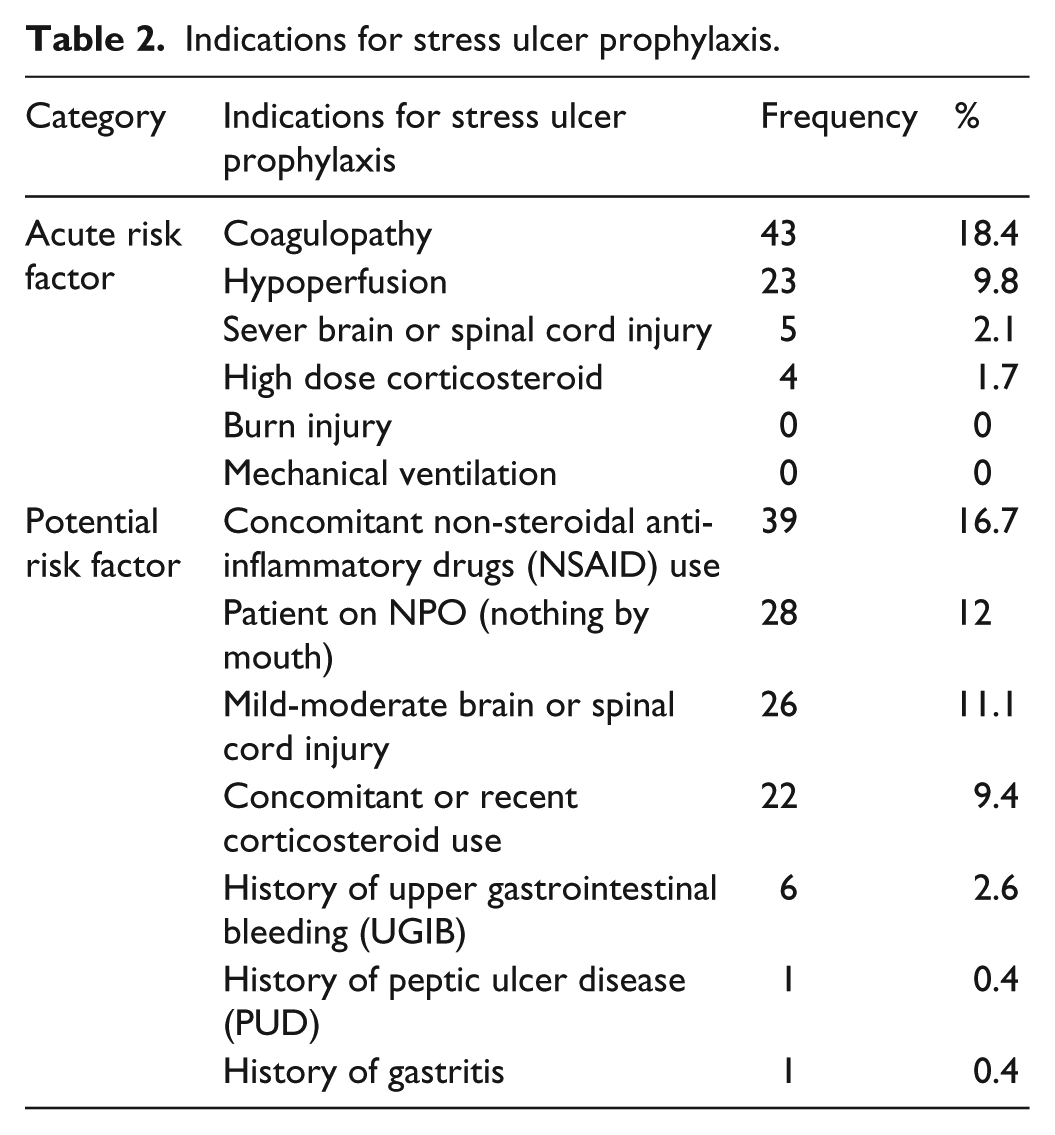
As indicated in Table 2, the most common acute risk factor to stress ulcer is coagulopathy (18.4%), followed by hypoperfusion (9.8%). The concomitant NSAID use (16.7%), mild-to-moderate brain or spinal cord injury (11.1%), and concomitant or recent corticosteroid use (9.4%) were the most frequent potential risk factors that necessitate administration of a prophylaxis for patients who were on NPO.
Indications for stress ulcer prophylaxis.
The most commonly used drug class in the prevention of stress ulcer was PPIs (92.7% of patients who were on SUP). Drugs used for SUP is shown in Table 3.
Drugs used for stress ulcer prophylaxis.

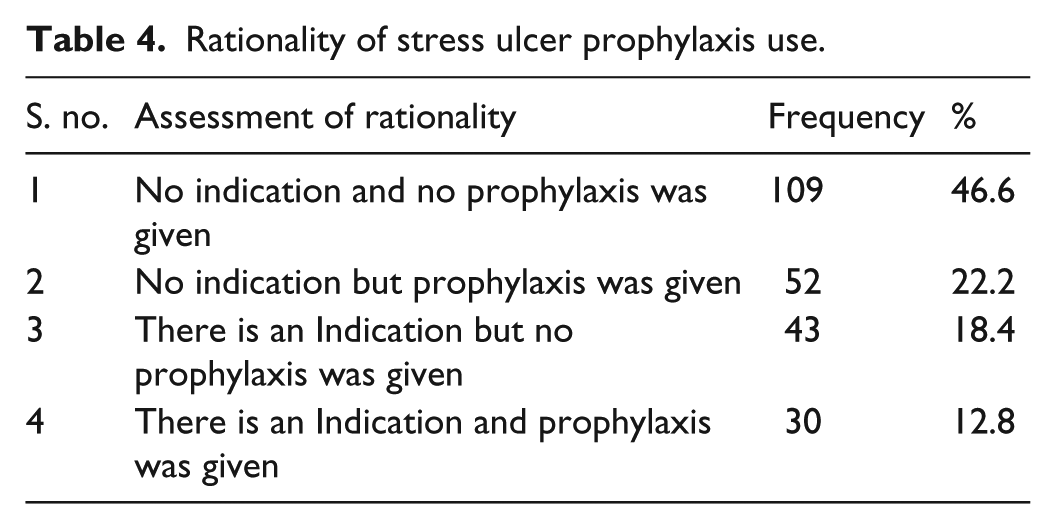
As shown in Table 4, 82 (35%) of the study participants were given SUP, among which 52 (63.4%) were given without indication. In total, 43 (18.4%) of the study subjects were not given SUP while there were clear indications.
Rationality of stress ulcer prophylaxis use.
As indicated in Table 5, patients with ⩽7 days of hospital stay are two times more likely to have appropriate SUP use (AOR 2.11, confidence interval (CI) 1.22–3.67), which indirectly implies longer hospital stay is associated with inappropriate SUP use. SUP use in patients without a diagnosis of central nervous system (CNS) disorders is more appropriate as compared to those having a CNS disorder (AOR 3.61, CI 1.47–8.89).
Factor associated with appropriateness of SUP use.

SUP: stress ulcer prophylaxis; COR: crude odds ratio; CI: confidence interval; AOR: adjusted odds ratio; CNS: central nervous system; CV: cardiovascular.
Indicates significant values (p < 0.05).
Discussion
In this study, SUP was prescribed for more than one-third (35%) of patients admitted at medical wards. This is in line with study conducted in the United States, which reported the use of SUP in 32% of hospitalized patients. 17 However, this figure is less compared to the study conducted in ICU setting.21,22 According to the survey conducted in the United States in 2014, a median of 90% of ICU patients were started on SUP. 23 This disparity may be due to increased risk for stress ulcer developing among patients admitted at ICU has more probability of having the risk factors for stress ulcer like mechanical ventilation, enteral feeding, hypoperfusion, and Glasgow Coma Scale (GCS) < 8.
In this study, SUP is inappropriately used in more than two-fifths of the study subjects. Similarly, Nasser et al. 24 and Barletta et al. 25 reported inappropriate SUP use among 51% and 32% of study subjects, respectively. However, the proportion of inappropriate SUP prescription in this study was less than what was reported in other studies, which indicated 60%–80% of inappropriate SUP use.19,26–29 This difference may be because our study was conducted at a teaching hospital where standard guidelines may be better practiced. Our claim was supported by many studies which revealed SUP usage in academic centers was more compliant with the guidelines than nonacademic hospitals.18,26,30
Routine administration of SUP in most non-ICU hospitalized patients has emerged as an important challenge in the health system.31,32 The high prevalence of inappropriateness in our study was attributed to the use of SUP while there was no clear indication. The result of this study is in agreement with previous reports.27,33–36 According to Farsaei et al., 19 70.3% of patients received SUP when it was not indicated. In addition, overuse of AST in non-critically ill patients has been reported by several investigators.37–39 Obviously, overutilization of acid suppressing agents could increase the cost of the patient and it will also increase the risk of drug interactions and long-term side-effects.40,41 Even though overutilization was high, there were also patients (18.4%) who did not get prescription for SUP while there were clear indication. Similar result was reported from a study done in Iran. 19 According to Masood et al., 22 9.67% of patients were not receiving SUP while it was indicated.
In this study, majority of patients were prescribed with PPI. This is comparable with studies conducted elsewhere.19,21,22,25,42–45 Possible reasons for the widespread use of PPIs in our setting might be due to the availability of the oral dosage form and the clinicians’ preference on PPIs to H2RAs. This widespread use of PPI is justifiable as there is strong body of evidence indicating their effectiveness for prevention of GI bleeding compared to H2RA. 46
In our study, the most common acute risk factor for stress ulcer was coagulopathy. This is consistent with other studies.19,22,29 According to Foroughinia and Madhooshi, 18 coagulopathy was the only absolute indication for SUP. Mechanical ventilation and burn were not found as an indication for SUP in the this study, while some other studies reported so far found mechanical ventilation as a common indication for SUP use.22,47 This difference may be because our study was conducted at a non-ICU setting where mechanically ventilated patients were less likely to be admitted. In line with our finding, studies by Farsaei et al. 19 and Mousavi et al. 29 reported that no patient was indicated for SUP due to mechanical ventilation and burn, respectively. Our finding showed that NSAID use was the commonest minor risk factor for SUP use. Similar result was reported in a study conducted at the nephrology wards of the Imam Khomeini Hospital, Tehran, Iran. 29
Different factors have been associated with inappropriate use of SUP for hospitalized patient. In this study, length of hospital stay and a diagnosis of CNS disorder were found to be significantly associated with inappropriateness of SUP use. This report is different from study conducted in Iran and ICU setting in North America (the United States and Canada).19,25 The possible justification for significant association between inappropriate SUP use and longer hospital stay may be because patients with longer stay had more chances of unnecessary SUP prescription as a result of more number of physicians’ visits over the longer periods of stay. This is further supported by the result of this study which states that the SUP use in the absence of indication is more common than the denial of SUP for indicated patients.
Limitations of the study
This study was undertaken at a single teaching hospital so that the results could not be generalized to other centers. Incomplete documentation may also be another potential limitation. For example, patients who were on AST and no indication was noted on the chart were presumed to be taking it as SUP. However, it may be possible that some of these patients had an appropriate indication that was not documented in the chart. Hence, we recommend cautious interpretation of this finding.
Conclusion
In this study, inappropriate use of prophylaxis for stress ulcer was common. The higher proportion of inappropriateness was due to the use of SUP while there was no enough indication. The long hospital stay and diagnosis of CNS disorders had a significant association with inappropriate SUP use. We recommend future researchers to assess the cost and impact of inappropriate SUP use, and the physicians should be adherent to the standard guidelines. Furthermore, all the possible factors that may directly or indirectly contribute for inappropriate use of SUP including prescriber-related factors should also be addressed.
Footnotes
Acknowledgements
The authors are very grateful to the nursing staff of medical wards of University of Gondar Hospital for their cooperation in the data collection process.
Data availability
The data used to support the findings of this study are available from the corresponding author upon request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the Ethical Review Committee of School of Pharmacy, University of Gondar (ethical approval number: SOP/821/2017).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was not sought for the present study because the data were obtained from charts.