
Abstract
Metastatic tumors to the liver resulting in fulminant hepatic failure are a rare occurrence and have not been previously described in patients with gastrointestinal stromal tumor (GIST). A 70 year-old man was referred to hospital with postprandial discomfort. On examination a 19.5 cm large epithelioid GIST of the stomach was diagnosed. The mass exhibited unfavorable prognostic features: mitotic index 18/50 high-power fields, large primary tumor size and male sex. Complete tumor resection with negative margins was achieved and metastases were not detected. The patient presented six months later with jaundice, asterixis and elevated liver enzymes. Computerized tomography showed multiple liver hypodense lesions representing metastases. Treatment with imatinib mesylate was of no avail and the patient died 3 days later as the result of hepatic failure. Massive liver metastases can, even though rarely, be responsible for fulminant hepatic failure. Clinical and radiological follow-up are crucial in patients with GIST even after surgical resection.
Introduction
Fulminant hepatic failure is defined as liver disease that causes encephalopathy within 8 weeks of onset of symptoms or within 2 weeks of onset of jaundice in a patient with no prior evidence of liver disease. 1 Viral hepatitis or drug hepatotoxicities are the underlying cause in the majority of patients. 2 Although the liver is a common site for the metastatic spread of various malignant diseases, hepatic involvement is usually mild, and fulminant hepatic failure is unusual.3,4 We report the case of a patient with fulminant hepatic failure secondary to massive infiltration of the liver by metastases, probably originating in the recently resected gastrointestinal stromal tumor (GIST). We could not find reports of similar cases in the literature.
Case Report
A 70-year-old man was referred to hospital for the evaluation of malaise of 2-week duration; anorexia, abdominal distension and jaundice occurred in the past 3-5 days. He was apparently in good health until March 2007, when nausea and postprandial discomfort occurred. A 19.5 cm large tumor, confined to the antrum of the stomach, was detected on gastroscopy. Partial gastrectomy was performed. Histological examination revealed typical features of an epithelioid gastro-intestinal stromal tumor. The tumoral cells were polygonal or rounded, with clear or eosinophilic cytoplasm and mild to moderate nuclear atypia. Areas of necrosis were seen. There were numerous mitoses (up to 18) in 50 high-power field power fields counted. There was also strong positive staining for CD 117 (c-kit) in the cytoplasm of tumor cells (Fig. 1). Complete tumor resection was accomplished with negative margins. Metastases were not detected on enhanced computed tomography examination, colonoscopy, surgical exploration and subsequent positron emission tomography. The patient made an uneventful recovery.
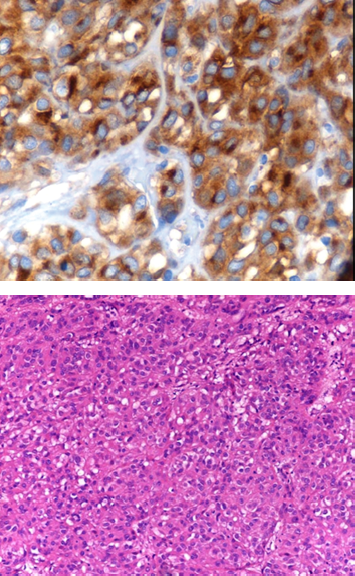
Epithelioid gastro-intestinal stromal tumor of stomach, unfavorable prognostic group. Tumor cells are polygonal or rounded, with clear or eosinophilic cytoplasm and mild to moderate nuclear atypia. Areas of necrosis were seen (not shown) and up to 18 mitoses in 50 high power fields counted (Hematoxilin and eosin, x 200).
In November 2007 he presented with anorexia, abdominal distension and jaundice. On physical examination the patient was sleepy, but not disoriented. The vital signs were unremarkable. Notable were flapping tremor, icteric sclera, severe loss of adipose tissue and skeletal muscle and enlargement of the liver. The liver was palpable 6 cm below the costal margin and felt hard and irregular. Pertinent biochemical parameters were as follows: total protein 6.9 g/dl, albumin 4.2 g/dl, total bilirubin 20.1 mg/dl, conjugated bilirubin 13.4 mg/dl, aspartate aminotransferase 625 IU/l, alanine aminotransferase 428 IU/l, alkaline phosphatase 1440 IU/l, and γ-glutamyl transpeptidase 1318 IU/l, prothrombin activity 32% (INR 1.8). The patient's hepatitis A, B, C, and cytomegalovirus (IgM) serologies were negative. Acetaminophen and alcohol were not present in the patient's blood. Computerized tomography showed multiple hypodense lesions within the liver, representing metastasis, sub-totally replacing the hepatic parenchyma (Fig. 2). Two small nodules were also noticed in right lung corresponding to metastases. Colonoscopy was performed to rule out alternative cause of liver metastasis and was interpreted as normal. Treatment with imatinib mesylate 400 mg per day was started, but was of no avail. The patient died 3 days after admission to the hospital in hepatic coma. Permission to autopsy was declined.

70-year-old patient with gastro intestinal stromal tumor. Non-enhanced axial CT images obtained at the level of the liver showing multiple hypodense lesions involving the left and right hepatic lobes and representing liver metastasis.
Discussion
The liver is commonly involved in metastatic disease, but fulminant hepatic failure due to metastatic carcinomatosis is exceptionally rare. Review of the literature in 2005 spotted 34 cases, 3 in the settings of various primary cancers. The mechanism of fulminant hepatic failure secondary to neoplastic infiltration of the liver includes: 1) hepatic ischemia and/or infarction, in the absence of shock, due to increased susceptibility of tumor cells to milder degrees of hypotension or hypoxemia; 2) parenchymal infarction due to vascular occlusion of portal vein by tumor thrombi, and 3) shock-liver due to sepsis or heart failure.5–7 Typically, the degree of aminotransferase elevation is well below that associated with acute hepatocellular necrosis. 5
Fulminant hepatic failure carries an extremely high risk of mortality. Liver transplantation is not indicated if malignant infiltration of the liver is present and alternative therapies may be available.3,4 In the patient described herein, fulminant hepatic failure was secondary to massive infiltration of the liver by metastases, probably originating in the recently resected GIST. This assumption is supported by the massive infiltration of the liver by tumoral tissue as well as by exclusion of etiologies other than neoplasia, the fast clinical deterioration, and the relatively moderate degree of aminotransferase elevation that was below that associated with acute hepatocellular necrosis. The clinical context and distribution of metastases are consistent with metastatic GIST. Indeed, the vast majority of GIST metastases at presentation are intra-abdominal, involving the liver; metastatic spread to lymph nodes and to other regions is rare. 8 Treatment with imatinib mesylate, 400 mg daily, was started but fulminant liver failure precluded a favorable response.
Matsushita et al 9 reported a case of GIST of the ampulla of Vater; the patient died of hepatic failure 2 months after the onset of jaundice. The time interval from onset of jaundice to encephalopathy in that latter case is not consistent with fulminant hepatic failure, also the pathogenetic mechanisms involving extrahepatic cholestasis in this case may be different from mechanisms operative in fulminant hepatic failure due to metastatic carcinomatosis.
Factors negatively influencing disease free survival of GIST are mitotic index >5/50 high-power field, primary tumor size >5 cm, male sex; 10 all three risk factors were present in our patient. Therefore, and in retrospect observing the postoperative course in this patient, the question arises whether a different management may have avoided the unfavorable outcome. Definitive expert surgery remains the mainstay of treatment for patients with primary localized GIST. However, GIST can exhibit a high risk for recurrence and ultimately may become a life-threatening condition. 8 In contrast with this view, others proposed that surveillance for recurrence is unnecessary based upon the follow-up of a cohort of patients with gastric GISTs. 11 In addition to close post-operative surveillance, this case illustrates the importance of adjuvant chemotherapy in high risk cases. In fact, it was clearly demonstrated in a recent RCT that imatinib improved recurrence-free survival in high risk GIST patients and imatinib is now approved for adjuvant treatment. 12 Unfortunately, imatinib treatment was of no avail in the patient treated by us.
Conclusion
Metastatic tumors to the liver resulting in fulminant hepatic failure are a rare occurrence and have not been previously described in patients with GIST. Massive liver metastases can, even though infrequently, be responsible for fulminant hepatic failure. To avoid such complication, persistent clinical and radiological follow-up are crucial in patients with GIST even after surgical resection.
Competing Interests
The authors declare that they have no competing interests.