
Abstract
Gastrointestinal stromal tumors, previously referred to as leiomyomas and leiomyosarcomas, are one of the most common mesenchymal tumors of the gastrointestinal tract, predominantly located in the stomach (60%–70%), followed by the small intestine (20%–30%). They manifest at any age but more commonly in patients older than 50 years. Patients with gastrointestinal stromal tumors usually have vague and nonspecific symptoms. The diagnosis is sometimes challenging requiring multiple imaging modalities, including computed tomography and magnetic resonance imaging, used for diagnosis, staging, and surveillance. Treatment involves surgery and targeted therapy. Serious complications have been reported such as intussusception which is exceptionally rare due to the extraluminal growth pattern tendency of gastrointestinal stromal tumors. We present the case of a 77-year-old female with duodeno-duodenal intussusception secondary to a gastrointestinal stromal tumor. This case report contributes valuable insight into the diverse presentation and complications of gastrointestinal stromal tumors.
Introduction
Intestinal intussusception in adults is rare and often results from underlying pathology, which can be benign (such as familial adenomatous polyposis, lipoma, and Meckel’s diverticulum) or malignant (such as lymphoma, adenocarcinoma, or secondary lesions). 1
Intussusception caused by gastrointestinal stromal tumors (GISTs) is extremely uncommon but documented. Diagnosing adult intussusception is challenging due to its varied clinical presentation, potentially leading to delays in intervention. 1
Various imaging modalities, such as ultrasonography, computed tomography (CT), magnetic resonance imaging (MRI), and endoscopy, are essential for diagnosis. This article presents the case of a 77-year-old female with duodeno-duodenal intussusception secondary to a GIST and details the clinical and radiological characteristics, therapeutic options, and prognosis. 2
Case report
A 77-year-old female with no significant medical or family history of malignancy presented with intermittent epigastric abdominal pain for over a month, without vomiting or signs of obstructive jaundice. Physical examination revealed only abdominal tenderness. Laboratory assessments were within normal limits, and tumor markers were negative.
An abdominal ultrasound revealed dilatation of the intrahepatic and extrahepatic bile ducts. Magnetic resonance cholangiopancreatography (MRCP) was performed to identify an obstruction, revealing duodenal intussusception associated with a tissue-enhanced mass telescoped within the third segment of the duodenum. The distal segment of the bile duct was entrapped within the intussusception (Figure 1). Further CT imaging showed a target-like appearance in axial sections, with D1 and D2 segments invaginated within the D3 segment and an enhanced intraluminal duodenal tissue mass post-contrast injection. The common bile duct and the head of the pancreas were retracted and entrapped within the intussusception, leading to upstream dilation of the intrahepatic and extrahepatic bile ducts (Figure 2).
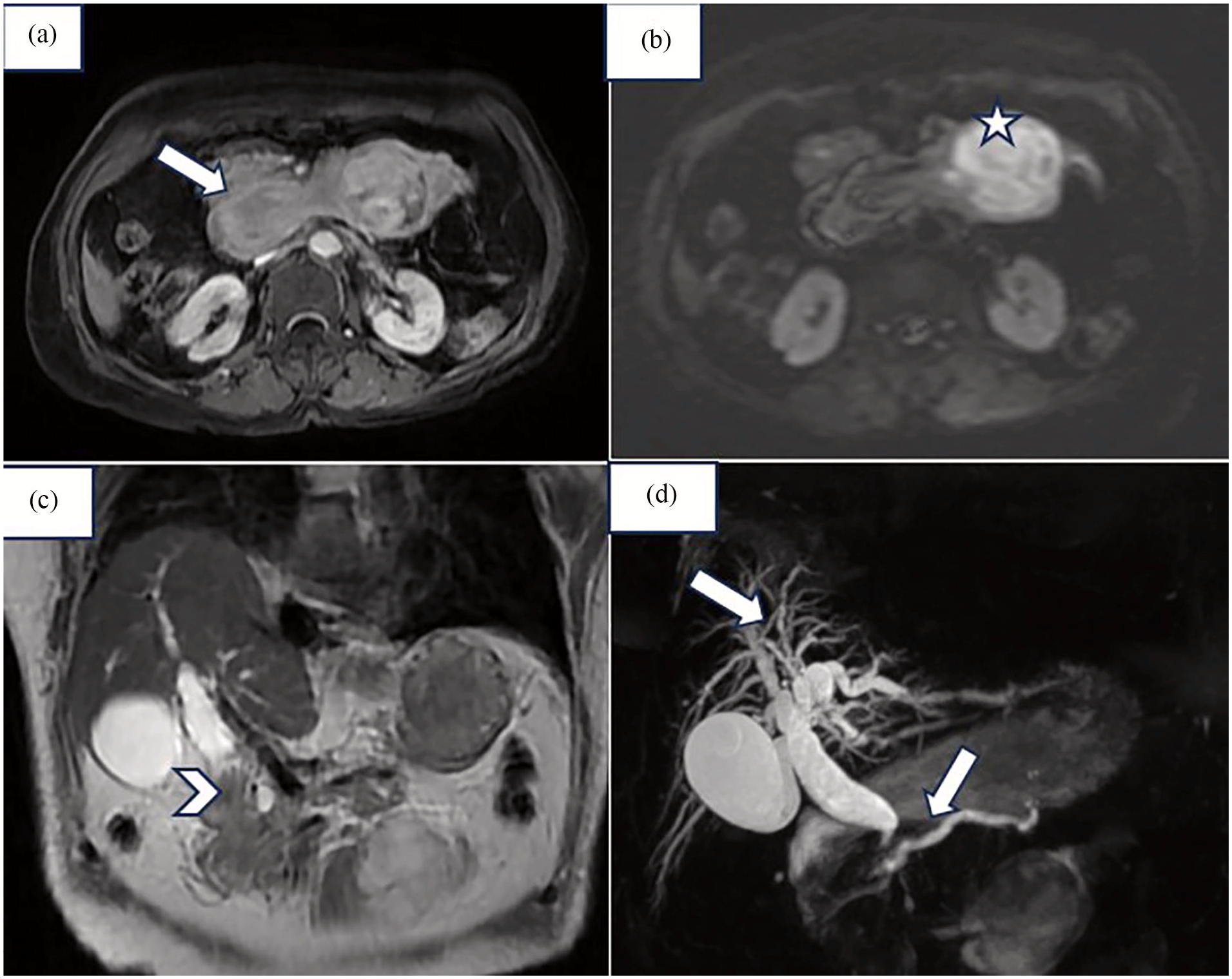
Magnetic resonance cholangiopancreatography (MRCP): (a) Axial section T1 sequence after administration of gadolinium. (b) Axial section Dwi: duodenal intussusception (white arrow) associated with a tissue-enhanced mass with restricted diffusion that appeared to be telescoped within the third segment of the duodenum (white star). (c) The coronal section of the T2 sequence shows a distal segment of the bile duct and the head of the pancreas entrapped within the intussusception (white arrowhead). (d) MRCP sequence shows dilatation of the intrahepatic biliary duct and the common bile duct as well as the Wirsung canal (white arrow).
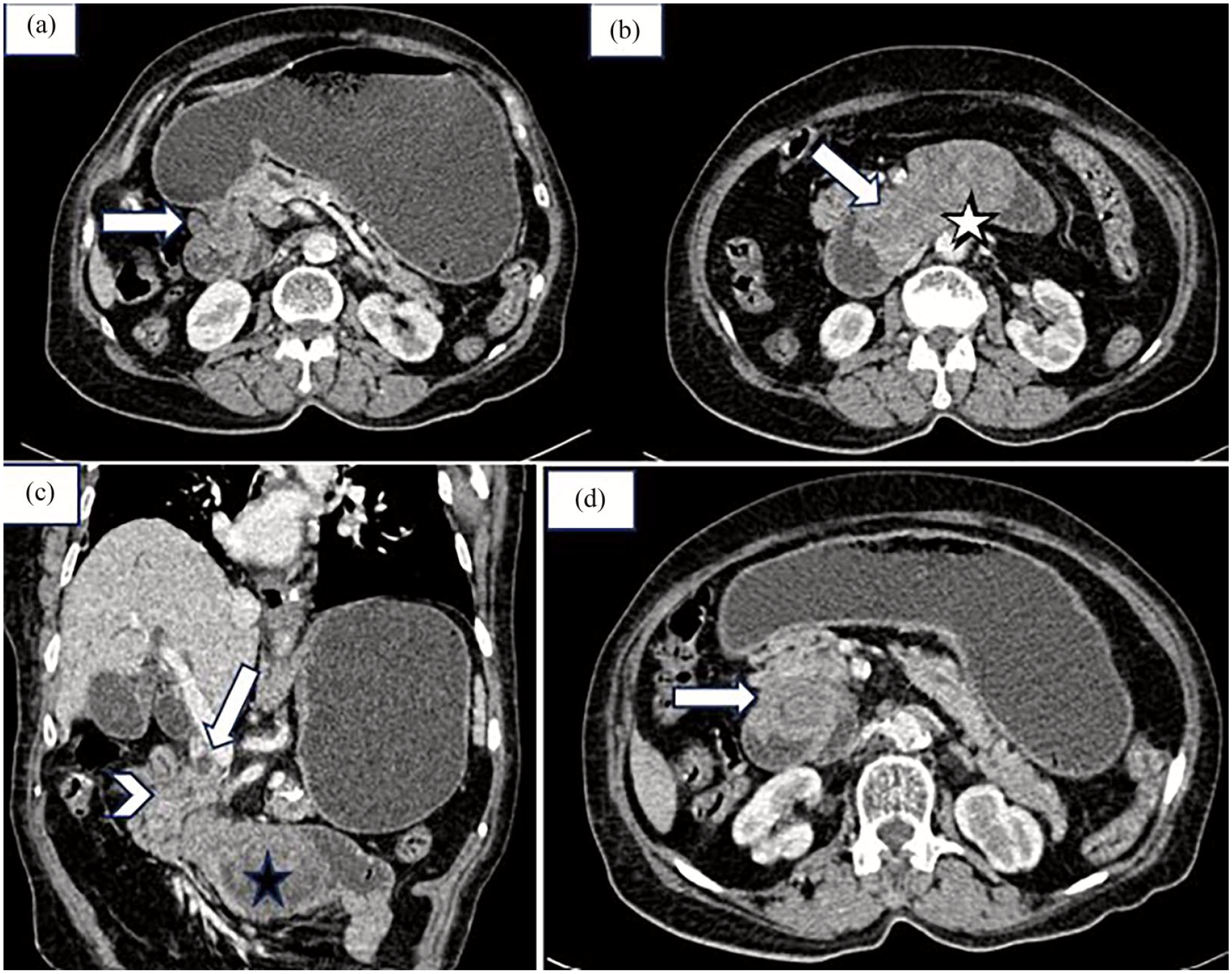
Abdominal computed tomography (CT) with contrast: (a) CT axial section: duodeno-duodenal intussusception (White arrow). (b) Axial CT section shows D1 and D2 segments invaginated within the D3 segment (white arrow) and an enhanced intraluminal duodenal tissue mass after contrast injection (Black star). (c) Coronal CT section: The common bile duct (white arrow) and the head of the pancreas (white arrowhead) appeared to be retracted and entrapped within the intussusception, leading to dilation of the intrahepatic and extrahepatic bile ducts upstream. (d) CT axial section: target-like appearance of duodeno-duodenal intussusception.
The patient underwent surgical intervention, including reduction of the intussusception, resection of the D1 segment and proximal D2, excision of the mass, and termino-terminal gastro-duodenal anastomosis (Figure 3). Surgical exploration revealed a mass at the pyloro-duodenal junction with histopathological examination confirming a GIST. The tumor resection margins were clear, and no neoadjuvant radiation or chemotherapy was recommended. The postoperative course was uneventful, with no complications. The patient was advised to have annual follow-ups for 5 years, the first follow-up was favorable.

Resected specimen (white arrow: resected GIST implantation site on D1 segment, white arrowhead: resected gastrointestinal stromal tumor, white star: resected duodenal segment).
Discussion
Intestinal intussusception in adults is rare, accounting for less than 5% of all intestinal obstructions. Entero-enteric and gastroduodenal intussusceptions due to a GIST are particularly uncommon, they only occur in less than 5% of cases. Generally, ileocolic intussusception is the most common, while ileo-ileal is the least frequent.1,2
Intussusception involves the telescoping of an intestinal loop, along with its mesenteric fold, into the lumen of an adjacent intestinal segment due to peristalsis. Two types are distinguished: with and without a lead point. In adults, it is usually attributed to an underlying pathology, unlike in pediatric cases. 3
This report focuses on intussusception with a lead point secondary to a GIST, the most common mesenchymal tumor of the digestive tract. 4 These tumors typically affect individuals over 50 years of age and can occur anywhere along the digestive tract, including the mesentery, omentum, and retroperitoneum. 4 The stomach is the most commonly affected organ, followed by the small intestine, rectum, esophagus, colon, and anus. Surgical treatment is necessary for adult intestinal intussusception. 5
Clinically, intussusception due to a GIST can present with abdominal pain, nausea, gastrointestinal bleeding from mucosal ulceration, and vomiting. These symptoms can be subacute or chronic. Physical examination may reveal abdominal tenderness or a palpable mass.5,6
Multiple imaging modalities can confirm the diagnosis. CT typically shows a target-like or sausage-shaped mass on axial sections with a characteristic “bowel within bowel” appearance and a causal soft tissue mass, usually appearing intraluminal in intussusception cases but typically exhibits an exophytic pattern. MRI demonstrates intestinal intussusception and a solid component mass that is hypointense on T1-weighted images and hyperintense on T2-weighted images, showing heterogeneous enhancement predominantly in the arterial phase, and restricted diffusion with low apparent diffusion coefficient values associated with higher-grade tumors.5,6
Reviewing available literature indicates that duodenal intussusception is rare due to the retroperitoneal location and immobility of the duodenum as well as the fixation of the duodenal wall to the retroperitoneum. 7 Reported cases of duodeno-duodenal intussusception are typically caused by adenomas, hamartomas, and Meckel’s diverticulum.7,8 Entero-enteric intussusception secondary to GISTs is exceedingly rare and the prognosis is mainly correlated with the malignancy of the GIST that is primarily defined by size and proliferation index (Ki-67 marker), with a median survival of 5 years for non-metastatic forms and 15 months for metastatic forms. Secondary locations of GISTs are predominantly mesenteric and omental, less commonly hepatic, and rarely lymph nodes. 9
Surgery remains the only curative treatment option, and lymphadenectomy is not always performed. However, the development of CD117 receptor antagonists (such as Imatinib) shows promise, particularly for inoperable patients and metastatic cases. Adjuvant therapy with Imatinib is suggested for high recurrence or metastasis risk, defined by tumor size, location, and mitotic changes. It is also recommended postoperatively to reduce recurrence risk. Radiotherapy and chemotherapy are less effective. There are reported cases where GISTs lead to surgical emergencies, such as massive hemorrhage, obstruction, perforation, or, exceptionally, intussusception, as reported in this case.9,10
Conclusion
Adult intestinal intussusception, particularly when attributed to GISTs, represents a rare yet clinically significant condition requiring meticulous diagnosis and management. This case of duodeno-duodenal intussusception in a 77-year-old female highlights the diagnostic challenges due to atypical presentations and the pivotal role of advanced imaging techniques in achieving accurate assessment. Surgical intervention remains the mainstay of treatment and targeted therapy has had a substantial impact on decreasing the risk of recurrence. Additionally, bile duct obstruction can result from duodeno-duodenal intussusception caused by a GIST, making it an important differential diagnosis to consider.
Footnotes
Acknowledgements
The authors thank his professors and colleagues who helped in the completion of this work.
Author contributions
B.K. contributed to conception or design, contributed to acquisition, analysis, and interpretation, drafted the manuscript, critically revised the manuscript, and agreed to be accountable for all aspects of work ensuring integrity and accuracy; B.I. contributed to conception or design, contributed to acquisition, analysis, and interpretation, drafted the manuscript, and agreed to be accountable for all aspects of work ensuring integrity and accuracy; P.I. contributed to conception or design, contributed to acquisition, analysis, and interpretation, drafted the manuscript, and agreed to be accountable for all aspects of work ensuring integrity and accuracy; N.I. critically revised the manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy; I.K. authorized the author to use the case, critically revised the manuscript, gave final approval, and agreed to be accountable for all aspects of work ensuring integrity and accuracy; M.B.N. critically revised the manuscript, gave final approval, and agreed to be accountable for all aspects of the work ensuring integrity and accuracy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from the patient for their anonymized information to be published in this article.