
Abstract
The bony skeleton is one of the most common sites of metastatic spread of cancer and is a significant source of morbidity in cancer patients, causing pain and pathologic fracture, impaired ambulatory ability, and poorer quality of life. Animal cancer models of skeletal metastases are essential for better understanding of the molecular pathways behind metastatic spread and local growth and invasion of bone, to enable analysis of host-tumor cell interactions, identify barriers to the metastatic process, and to provide platforms to develop and test novel therapies prior to clinical application in human patients. Thus, the ideal model should be clinically relevant, reproducible and representative of the human condition. This review summarizes the current in vivo animal models used in the study of cancer metastases of the skeleton.
Introduction
Primary and secondary cancers are amongst the leading causes of morbidity and mortality. Along with the lung and liver, the bony skeleton is one of the most common sites for metastases, with most cases occurring in the spine.1–3 Skeletal metastases frequently originate from carcinoma of the breast, prostate, and lung, and if they continue to grow and destroy bone result in pain and pathologic fracture, impaired ambulatory ability and poorer quality of life.2–7 The process of cancer metastases following tumor growth at the primary site of origin involves intravasation and survival in the bloodstream, arrest, extravasation and finally establishment by invasion and angiogenesis at a distant site.2,3,8 The ability of metastatic cancer to grow within and invade bone is largely mediated by tumor-induced growth factors and cytokines that result in imbalance between the bone-forming osteoblasts and bone-degrading osteoclasts of bone marrow that normally regulate bone turnover.2,3,9
Animal models of cancer metastases are essential in order to better understand the molecular pathways behind metastatic spread and local growth and invasion at distant sites, enable analysis of host and cancer cell interactions, identify barriers to the metastatic process, and to provide potential platforms to develop and test novel therapeutic agents. The ideal model should be clinically relevant, reproducible and representative of the human condition. The broad approaches to animal model studies include spontaneous, chemically or genetically-induced, syngeneic, and xenograft cancer models. Although spontaneous models resemble what occurs when humans develop cancer, the spontaneous development of primary and metastatic cancer in animals is extremely rare. 10 Similarly, the metastasis rate of genetically-induced tumors, either by inducing expression of oncogenes or deletion of tumor suppressor genes, is generally very low and too variable and unpredictable in terms of spreading to bone to provide useful skeletal metastasis models. Therefore, animal models of skeletal metastases typically require physical introduction of cancer cells. Syngeneic models are those in which tumor cells and host are of the same origin and involve introduction of tumor cells isolated from spontaneously occurring rodent or small animal cancers, whereas xenograft models involve the introduction of human tumor cell lines into an immunodeficient host.
Important considerations include the host animal, method of inoculation of tumor cells, type of cancer for investigation, analysis of the developing tumors and clinical application of the model. This paper reviews these considerations, with a specific focus on in vivo animal models of cancer metastases to the bony skeleton.
Host Animal for Cancer Metastasis Models
Established
To date, the rodent has been the most popular host animal used in the study of bone metastases.
8
Rodents have a high degree of gene sequence homology with humans, similar anatomical organs, are easy to handle and maintain, readily available and relatively cheap, and can be manipulated for investigation of specific cancer pathways by generating knockout, transgenic, or over-expressing strains.11,12 Immune-deficient animals such as
One of the disadvantages of using immunodeficient animals in models of cancer metastases is that they preclude investigation into the important role of the immune system in combating cancer. 11 This may be overcome by the use of syngeneic models, in which cancer cell lines of the same species as the host are introduced into immunocompetent animals. Lelelakis et al described a mouse model of breast cancer metastases to bone using a clonal tumor cell line from a spontaneously arising murine mammary cancer, in which metastases to the femur and spine followed intracardiac and mammary pad inoculation of the cancer cells. 15 Another disadvantage of rodent cancer models includes the small size of rodent bone, potentially making direct implantation of cancer cells, as well as investigation of therapeutic modalities such as local drug delivery devices and invasive imageguided-therapies, more technically challenging.12,16,17
The use of rabbits may be less technically demanding for surgical procedures and may enable easier analysis and preclinical testing of skeletal metastases. However, experimental immunodeficient rabbits are currently not available; thus, species-specific cancer cell lines are required in rabbit syngeneic cancer models and these are extremely limited in availability.11,16,17 Despite this, VX2 carcinoma cells derived from a virus induced papilloma of the rabbit have been used in two rabbit models of spinal tumors to successfully replicate the clinical, radiological, and histopathologic characteristics of the human condition.16,17 Orthotopic implantation of the VX2 carcinoma cells into the third lumbar vertebra or the lower thoracic vertebra of healthy rabbits after surgical exposure led to lower limb paralysis in most rabbits by four weeks post-implantation.
Larger-sized animals that can potentially be used in cancer models include the cat and dog. Although the cat has not yet been established as a useful syngeneic or xenograft animal model for the study of skeletal metastasis, spontaneous metastases to the digits of the bony skeleton and in soft tissues of the proximal limbs in cats have been observed secondary to primary pulmonary adenocarcinoma.18,19 In a larger syngeneic orthotopic animal model, a dog model of prostate cancer metastasis, Anidjar et al demonstrated bone metastases following direct inoculation of DPC-1 poorly differentiated canine prostate adenocarcinoma cells into the prostate gland. 20 Histopathology of the mixed osteoblastic and osteolytic pelvic bone lesions showed similarities to human prostate cancer skeletal metastases. 20 A potential advantage of the larger canine model over rabbits or rodents is that dogs may be more amenable to diagnostic and surgical procedures with equipment used in human clinical practice; however, the cost and restricted availability of the animals and species-specific cancer cell lines remain limitations.
Inoculation of Cancer Cells
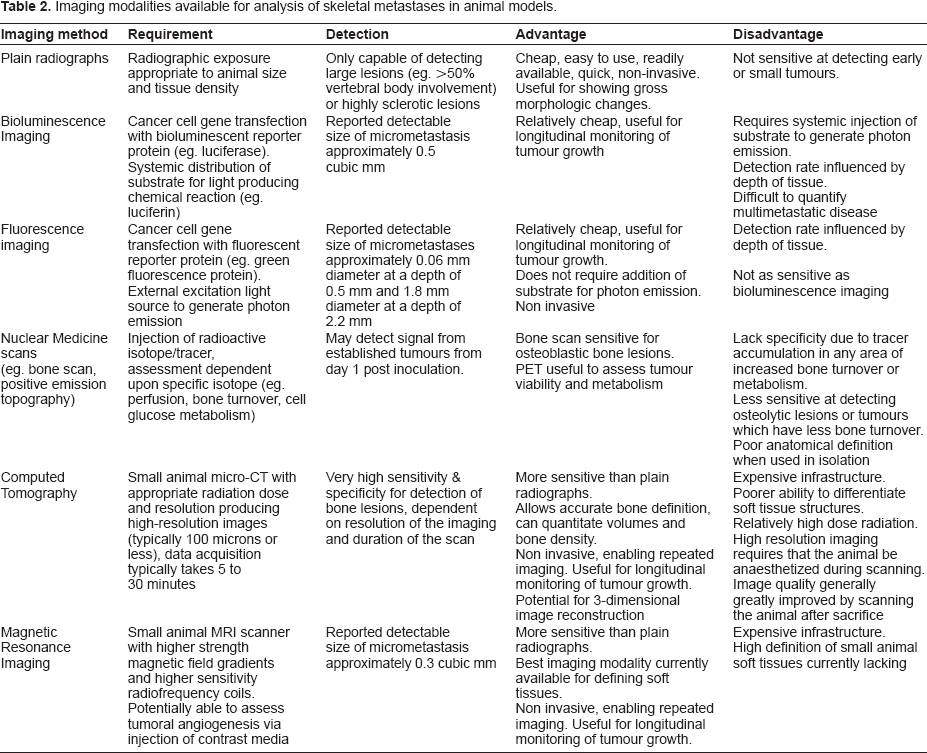
As described above, since the spontaneous development of metastatic cancer in animals is rare and unpredictable, animal models of skeletal metastases typically require physical introduction of cancer cells. Commonly used methods of cancer cell inoculation include systemic intracardiac or tail vein injection, injection into the arterial circulation, direct inoculation into the primary cancer site such as the mammary fat pad or prostate gland, or direct orthotopic inoculation into bone, reproducing the secondary skeletal deposit in isolation (Table 1).
Models involving systemic dissemination of tumor cells permit investigation of the key elements of the metastatic cascade from survival within the bloodstream, to selection of a distal site, and eventually to extravasation, establishment and growth of distant metastases, thus allowing analysis of the molecular mechanisms involved in growth and proliferation, migration, invasion and angiogenesis of metastatic cancer cells.11,15 Intracardiac injection into the left ventricle results in systemic arterial circulatory dissemination of tumor cells, with the potential of generating widespread metastases. Arguello et al described a reproducible murine model of skeletal vertebral and long bone metastasis following intracardiac injection of B16 (sub-line G3.26) murine melanoma cells. 21 However, the sites of metastatic deposition and number and size of the metastases were unpredictable, extremely variable, and dependent on the amount of cancer cells administered. The quantity of resultant bone metastases increased with increasing number of cells injected.
Tail vein inoculation similarly results in hematogenous dissemination of cancer cells, although cells may be filtered and cleared by the pulmonary system during the first passage through circulation. 22 Passineau et al described tail vein injection of A20 murine lymphoma cells to generate a syngeneic mouse model to mimic disseminated human B cell lymphoma, with bony deposits to the femur, pelvis and vertebral column, eventually leading to bone destruction and nerve compression. 23 Biesalski et al described intraarterial injection of Walker 256 mammary carcinoma cells directly into the circulation of the hindlimbs in rats via the superficial caudal epigastric artery, a branch of the femoral artery, resulting in metastases to the distal femur or proximal tibia/fibula in 9 of 11 animals at 3 weeks post-inoculation. 24 Limitations of systemic administration of tumor cells include variability and unpredictability in site, size, number, and time to development of metastasis.10,11 This may also lead to excessive tumor burden and morbidity in the experimental animal, therefore precluding the ability to investigate potential therapeutic interventions.
Direct inoculation of tumor cells into primary sites such as the mammary fat pad also has the potential to create a complete model of the metastatic process, since the tumor must first establish in the primary site before seeding to distant sites. 15 Schubert et al described a mouse model of breast cancer metastasis to the femur and lung after MDA-MB-435 human breast cancer cells were injected into the mammary fat pad of nude mice. 25 The ability of gonadotropinreleasing hormone (GnRH) analogs to significantly reduce formation and growth of breast cancer metastases in this model suggested the multi-focal role of GnRH throughout the metastatic process of breast cancer, including epithelial-mesenchymal transition, migration, invasion, and biology of circulating cells.
Direct orthotopic inoculation into bone has the potential to produce reproducible, efficient, and site-specific models of cancer and metastasis since a known quantity of cancer cells can be directly administered into the target bone of choice. Direct inoculation into bone bypasses the metastatic cascade and is not a true model of metastases, nevertheless it permits targeted investigation of the cellular processes involved within a particular anatomical site and the local effects of the tumor itself. Mann et al described a mouse model of tumor-induced osteolysis following orthotopic injection of F10 human breast cancer cells into the distal femoral metaphysis to assess the ability of non-invasive imaging and computational techniques for predicting the strength of bones with osteolytic lesions.
4
Choi et al used direct orthotopic inoculation of VX2 carcinoma tissue fragments into the tibial shaft of rabbits to create a model for magnetic resonance imaging (MRI) and histopathologic evaluation of the evolution of metastatic bone tumor.
26
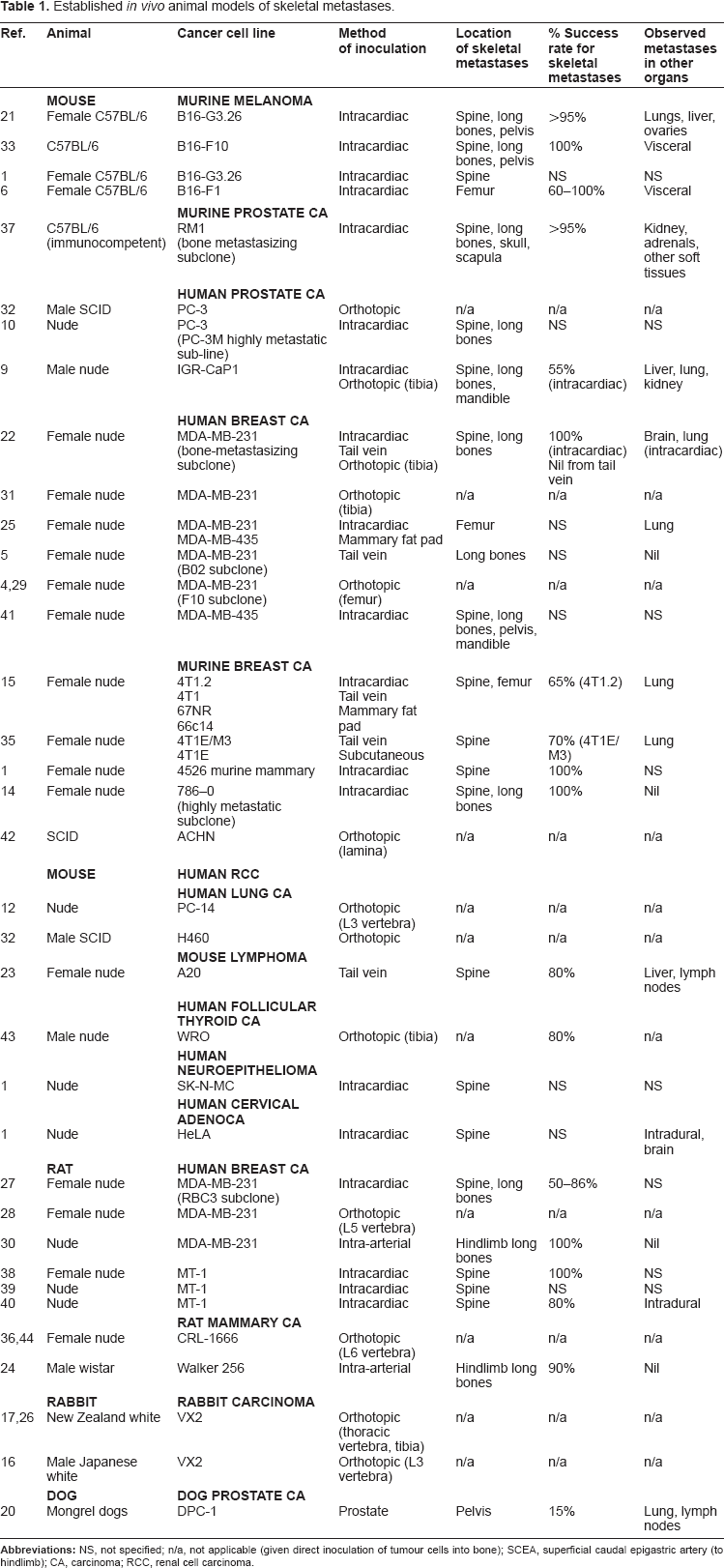
Orthotopic inoculation may be a relatively straightforward procedure if prominent and subcutaneous bones are selected, such as the distal femur or proximal tibia, which are also common sites for primary and secondary bone cancers. In our own laboratory, we recently established a novel in vivo model of spinal cancer that causes a reproducible, evolving paraplegia following orthotopic inoculation of MDA-231 human breast cancer cells or PC-3 human prostate cancer cells into the vertebral body at the thoracolumbar junction of Representative images of established spinal cancer (arrows) following orthotopic injection of PC-3 human prostate cancer cells in the vertebral body of the thoracolumbar junction in a nude mouse. A) Dissected spine specimen; B) Sagittal, and C) axial micro-CT images demonstrating lytic bony lesion and cortical destruction; D) Histological cross-section showing tumor invasion of vertebral bone marrow and encroachment onto the spinal cord (SC); E) Control histological cross-section.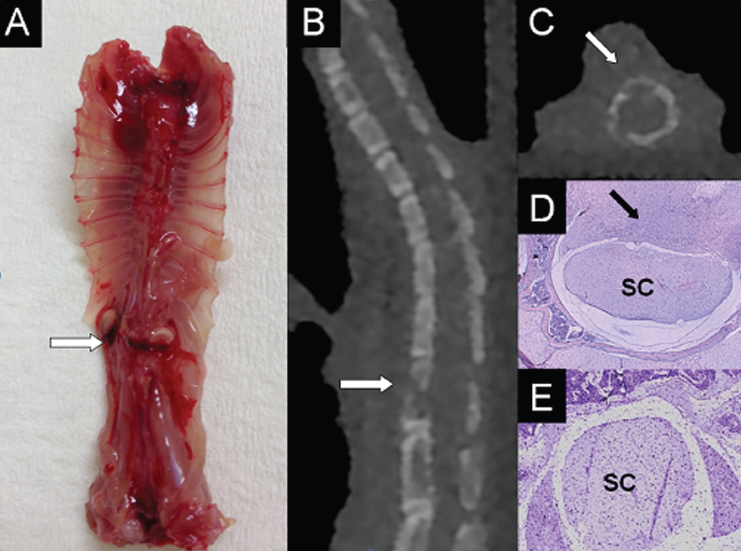
Cancer Cell Lines
Amongst the commonest primary cancers that metastasize to bone are breast, prostate, lung, and renal, carcinoma. Since the biological behavior and response to therapy of bone metastases is largely dependent on the primary cancer type, there is a need to develop investigative models of varying cell lines. For example, prostate cancer bone metastases in humans are generally more osteoblastic or sclerotic in nature, while renal cell carcinoma bone metastases are often more lytic and vascular compared with other cancer types.2,3,14 Indeed, a sub-line of the 786-O human renal cell carcinoma cell line with increased bone metastatic potential showed higher expression of the pro-angiogenic factors VEGF and basic fibroblast growth factor (bFGF) compared with the parental cell line. 14
Immortalized cancer cell lines that are generated through isolation of tumor cells from these spontaneously occurring primary or secondary cancer types in humans or animals are ideal for use in in vivo cancer models as they have already demonstrated ability to form, grow, invade, and spread within the primary organ or metastatic site of choice. Human cancer cells lines with a propensity for localization to bone and that are well-established for use in animal cancer metastasis models of metastases include the MDA-MB-231 human breast cancer cell line isolated from the pleural effusion of a patient following breast cancer metastasis to the lungs,5,22,27–31 and PC-3 human prostate cancer cells derived from a bone metastasis.8,9,32 The use of cancer cell lines of human origin ensures that molecular and histologic analysis is as comparable to the human condition as possible; however, one important limitation is the requirement for use of an immunocompromised animal, which precludes investigation of the host immune response to the development of cancer and metastases. 11 The B16 murine melanoma cell line, derived from a melanoma from the skin of a C57BL/6 strain mouse,6,21,33 and the VX2 rabbit carcinoma cell line, originated from a carcinoma induced by the Shope cottontail rabbit papilloma virus,16,17,26 are common animal cell lines used in models of skeletal metastasis models that exhibit similar molecular characteristics to human cancer cells.
Cell sub-lines with site-specific metastatic properties, such as the propensity to metastasize to the skeleton, are often generated from primary cell lines through serial culture and repeated injection of cells cultured from metastatic lesions at the site of interest. For example, Zadnik et al derived a novel cell sub-line, RBC-3, from human MDA-MB-231 breast cancer metastatic spinal lesions in a rat. 27 Parent MDA-MB-231 human breast adenocarcinoma cells were introduced by intracardiac injection into rats to induce metastatic spinal lesions that caused neurologic deterioration and were confirmed on imaging. Affected animals were then euthanized, tumor tissue was excised, and tumor cells were harvested through a process of tissue digestion, cell filtration, centrifugation, and incubation. The selected cell sub-line (RBC-3) was observed to have a growth pattern consistent with that of the parent line, and following intracardiac injection into a host animal, resulted in a statistically significant increase in tumor burden in comparison to the parent MDA-MB-231 breast cancer cells. 27 Similar findings were observed in a mouse model of human breast cancer metastasis, whereby the selected cell sub-line (B02) injected into the tail vein demonstrated a propensity to form rapidly growing osteolytic hindlimb bone metastases. 5 These cancer cell lines may potentially be investigated in vitro to identify molecular events important in cellular proliferation, survival, paracrine, and autocrine factors involved in angiogenesis and bone breakdown as well as response to treatment.
Analysis of Animal Cancer Metastasis Models
Real-time imaging is useful for the detection, quantification, staging, and longitudinal monitoring of established tumors and response to treatment in in vivo cancer models.10,27 However, accurate delineation of tumor shape, size, and relationship to surrounding tissues remains a challenge due to the relatively small size of the subject matter. Plain radiographs are cheap, easy to use, and readily available, but can only detect large osteolytic lesions within bone. 16 Nuclear medicine bone scans are sensitive for detecting osteoblastic bone metastases, but may miss small lesions less than one centimeter in diameter and lack specificity due to tracer accumulation in any area of increased bone turnover. 33 Optical imaging is a popular imaging modality currently used in in vivo cancer models and is based on the detection of photon emissions from within living tissues. Prior to inoculation, cancer cells are transfected with genes encoding fluorescent or bioluminescent reporter proteins; however, these differ in generating light emitting photons. Fluorescent sources emit light at a particular wavelength in response to an external excitation light source, whereas bioluminescent sources produce light as a result of a chemical reaction between a systemically distributed substrate, such as injection of luciferin, and the enzyme activity of a reporter protein encoded into cancer cells, such as the Firefly luciferase protein.10,34 In a mouse model of breast cancer skeletal metastases following intracardiac injection of luciferase transfected MDA-231-B cells, bioluminescence imaging detected bone metastases of approximately 0.5 mm3 in volume. 22 Real-time identification of tumors at their early stages of growth potentially enables monitoring of disease progression and investigation of efficacy of therapeutic interventions.
Imaging modalities available for analysis of skeletal metastases in animal models.
Histopathologic assessment may be used in analysis of skeletal metastases models to complement the clinical and radiological imaging observations and to better understand the pathogenesis of metastasis by more specifically defining the location and extent of tumor growth, morphologic changes of bone and alterations in gene and protein expression.12,28–30 Histopathologic correlation can be utilized to confirm similarities between animal and human cell lines with regards to cytologic appearance of tumor cells and progression of tumor growth.9,20,23 Furthermore, the mechanisms by which cancer metastases cause clinical symptoms in the experimental animals may be determined through histologic correlation. Vertebral histologic cross-sections in a rat model of intraosseous spinal metastases showed aggressive infiltration and marked osteolytic activity of the tumor cells invading through the vertebral body and compressing the spinal cord, consistent with the clinically observed progressive neurological dysfunction. 36 In a rabbit model of paraplegia caused by spinal tumors, histologic analysis of spine tumor cross-sections from animals with complete paralysis showed a marked reduction in both grey matter and blood vessels to the spinal cord, suggesting that paraplegia may be caused by both direct compressive and ischemic vascular effects to the spinal cord. 16
Immunohistochemistry and immunotyping through methods such as enzyme-linked immunosorbent assay (ELISA), flow cytometry and polymerase chain reaction may be used to identify markers that contribute to the metastatic potential of tumor cells.14,30,35 In the development of a mouse model of renal cell carcinoma bone metastases, ELISA analysis of the selected cell subline with increased bone metastatic potential demonstrated greater production of chemokines and growth factors such as vascular endothelial growth factor (VEGF) involved in tumor progression and osteoclast activation than the parent cell line. 14 Further detailed molecular analysis of tumor sections at the metastatic site will provide improved understanding of the temporospatial pattern and pathological mechanisms behind cancer spread to bone and its subsequent growth and invasion into surrounding soft tissues.
Clinical Application of Animal Cancer Metastasis Models
Animal models are essential for investigating the important molecular mechanisms involved in the metastatic spread of cancer to bone and the testing of promising novel therapies prior to clinical application in human patients.10,37 The bone marrow microenvironment, incorporating local tissue and tumor-expressed factors, is known to be important in the initial establishment and proliferation of cancer cells in bone.10,15 Factors involved in physiological and pathological bone turnover and angiogenesis such as parathyroid hormone-related protein (PTHrP), receptor activator of NFκB ligand (RANKL), VEGF, tumor necrosis factor-α, transforming growth factor β, prostaglandins, and interleukins, have been shown to be expressed in many primary and secondary cancers and have been extensively investigated in animal models of skeletal metastases.11,14,15 Lelekakis et al found high expression of PTHrP in both primary tumors and bone lesions in a murine breast carcinoma model. 15 Bone metastases induced by parental MDA-231 human breast cancer cells in a xenograft mouse model were shown to highly express bone resorbing and pro-angiogenic factors such as PTHrP, macrophage colony stimulating factor, and VEGF, highlighting the importance of these factors in the bone metastatic cascade. 22 Consequently, the angiogenesis and osteoclastic bone-degradation pathways are effective targets for current and emerging therapies for skeletal metastases.
An important pro-osteoclastogenic factor required for the development and function of bone-resorbing osteoclasts is RANKL. Blocking RANKL has been shown to inhibit breast and prostate cancer-induced osteoclastogenesis and tumor development, growth and progression in bone. 14 Bisphosphonates have also been shown to potently inhibit osteoclast-mediated bone resorption and can reduce skeletal tumor burden and inhibit the formation of bone metastases in vivo, as well as demonstrating clinical application in the treatment of patients with osteolytic bone metastases.31,34,38,39 Photodynamic therapy, which causes oxygen toxicity and tumor cell necrosis by light activation of an administered photosensitizer accumulated in tumor tissue, has been shown to inhibit tumor growth in several rat models of human breast cancer vertebral metastases, with additional improvement in the structural integrity of vertebral bone when used in conjunction with bisphosphonates.38–40
In a metastatic mouse breast cancer model, Takahashi et al demonstrated that expression of the chemokine CCL2 negatively regulated bone metastasis and that CCL2 may act as a negative upstream regulator of intracellular adhesion molecule-1 expression, which is important for determining the capacity for growth, invasion, and metastasis. 35 Overexpression of the avβ3 integrin, a transmembrane protein that integrates intra- and extra-cellular activities and induces tumor cell migration, proliferation and differentiation has been observed in several experimental models of bone metastasis.30,34 Treatment with cilengitide, a small molecule inhibitor of avβ3 and avβ5 integrins, resulted in pronounced anti-resorptive and anti-tumor effects in a rat model of breast cancer bone metastasis. 30 , Further development and characterization of animal models of skeletal metastasis are necessary to provide suitable platforms on which to identify and test novel therapies.
Conclusion
Metastatic spread of cancer to the skeleton has the potential to cause severe morbidity, deterioration in function and mobility, and impaired quality of life. To date, there are many established in vivo animal models of skeletal metastasis, varying in host animal, type of cancer investigated, method of tumor inoculation and metastatic potential. Further characterization of these models and development of new, novel animal models focusing on specific cancer types and metastatic sites are essential for better understanding the mechanisms behind why and how particular cancers metastasize to, establish within, and invade bone. Ultimately, the identification of key targets for therapeutic intervention, development of novel therapies, and testing of these agents in clinically relevant animal models may be translated into improved treatment, quality of life, and survival of patients with metastatic cancer.
Author Contributions
Wrote the first draft of the manuscript: CH, GQ. Contributed to the writing of the manuscript: CH, DC, GQ. Agree with manuscript results and conclusions: CH, DC, GQ. Jointly developed the structure and arguments for the paper: GQ, CH. Made critical revisions and approved final version: CH, DC, GQ. All authors reviewed and approved of the final manuscript.
Funding
This work was supported by the National Health and Medical Research Council of Australia (Fellowship No. 558418), the Austin Health Medical Research Foundation and the Victorian Orthopaedic Research Trust.
Competing Interests
Authors disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests. Provenance: the authors were invited to submit this paper.