
Abstract
Background
Metastatic cells from a primary tumor can occur before the primary cancer is detected. Metastatic cells can also remain in the patient for many years after removal of the primary tumor without proliferating. These dormant malignant cells can awaken and cause recurrent disease decades after the primary treatment. The purpose of this article is to review the clinical evidence for early dissemination and late recurrences in human malignant tumors. We used the following definitions: dormancy of cells may be defined as a nonproliferating state or an arrest in the cell cycle that results in a prolonged G0 phase. If one accepts the term “late metastases” to indicate a period exceeding 10 years from the removal of the primary tumor, then the two malignancies in which this occurs most frequently are cutaneous malignant melanoma (CMM) and renal cell carcinoma (RCC).
Methods
PubMed, Web of Science, and Scopus were searched with the keywords “metastases,” “early dissemination,” “late recurrences,” “inadvertently transmitted cancer,” “tumor growth rate,” “dormancy,” “circulating tumor cells,” and “transplantation of cancer.”
Results
Several case reports of early dissemination and late recurrences of various types of malignancies were found. Analyses of the growth rates of several malignant tumors in the original host indicated that the majority of cancers had metastasized years before they were detected. CMM, RCC, and malignant glioblastoma were the three most common malignancies resulting from an organ transplantation. CMM and RCC were also the two most common malignancies that showed dormancy. In several cases of transplanted CMM and RCC, the donor did not have any known malignancy or had had the malignancy removed so long ago that the donor was regarded as cured.
Conclusion
(1) Metastases can frequently exist prior to the detection of the primary tumor. (2) Metastatic cells may reside in organs in the original host that are not usually the site of detectable secondary tumors, for example, the kidneys and heart. (3) Metastatic cells remain dormant for decades after the primary tumor has been removed. (4) Dormancy might be reversible and lead to late recurrences.
Keywords
Introduction
Since the days of the German pathologist Rudolf Virchow (1821–1902), it has been assumed that the anatomic progression of a malignant cell population is a stepwise process from the primary tumor to the regional lymph nodes and from the regional nodes to more distant organs. For more than a century, this has been the rationale for removal of the draining lymph nodes as part of the primary treatment.
Converging evidence from studies on human tumor cell kinetics, human disease courses, and genetic analyses of patients indicates that dissemination from a primary tumor might be an early event in the malignant progression. Even small cancers (<5 mm in diameter) can have the capacity to generate multiple metastases 5–10 years before they are detected. This has occurred in most of the common solid malignancies in humans, including cancers of the breast, prostate, lungs, colon, kidney, and malignant melanomas among others.
The early disseminated cells might not grow into overt metastases immediately but can remain quiescent in a dormant state for long periods. Several publications on “early dissemination but late metastases” exist. Only some of the more recent and comprehensive of these articles are reviewed here.
The cases where organs have been transferred from a donor to a recipient, and a malignant cell population has been inadvertently transmitted, are reviewed in this article. These cases lend support to the concept “early dissemination and late metastases”.1–17
Inadvertently Transplanted Malignant Tumors
History
Inadvertent transmission of a malignant tumor has occasionally occurred concomitant with organ transplantation. The first known recipients were immunosuppressed, and the transplanted tumor was detected shortly after the transplantation when the tumor cells grew in several of the recipients' organs. Therefore, in the early days of transplantation surgery, it was recommended that donors with a history of malignant tumors should not be accepted as organ donors.
However, the demand for organs exceeds the supply, and donors with a history of malignancies could not always be excluded. In 2010, in the United States, there were more than 100,000 patients on the waiting list for an organ, but only some 30,000 organs were available. Donors with a history of a malignancy were, therefore, occasionally accepted provided that the disease-free period was so long that the patient was regarded as cured and his/her organs thus deemed free from metastases. However, clinical evidence proved that the transplanted organ could inadvertently transmit an undetected population of tumor cells even decades after the removal of the primary tumor in the donor.
The first two cases of inadvertently transplanted malignant tumors were published in 1965.9,18 A registry for transplanted malignancies was started by the American surgeon Israel Penn: The Israel Penn International Transplantation Tumour Registry (IPITTR) in the 1960s, and its first report appeared in 1971. 19 Similar registries have since been established in Great Britain, 20 Australia/New Zealand, 21 and Scandinavia22–25 among others. These registries have been the source of several publications on the transmission of malignancies via transplanted organs, and some of these are summarized in this review.26–30
A 2007 review presented more than 160 cases 27 that had occurred out of an estimated 1,000,000 organ transplants (the authors' estimate) over the last 50 years.
Frequency and Histopathological Types of the Most Common Malignancies of Donor Origin among Patients with a Transplanted Organ
The most frequent types of donor-derived malignant tumors.
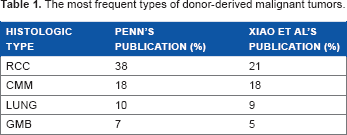
The similarity between the two groups of patients is remarkable, despite the fact that the two groups of donors had highly different medical histories and ethnicity.
All the transplanted cancers became detectable in several of the recipients' organs within a few months after the transmission, and they grew in several of the recipients' organs including the bone marrow, lungs, liver, and lymph nodes. The tumor cell populations were all of donor origin as shown by sex chromosomes or other markers. 27 For example, if the donor was a female (chromosomes XX) and the recipient a male (chromosomes XY), karyotyping of the tumor cells indicated the origin.
The 13 most frequent cancers in the US in 2007 out of a total of 930,000 cases (derived from AACR Cancer Facts & Figures, 2007).
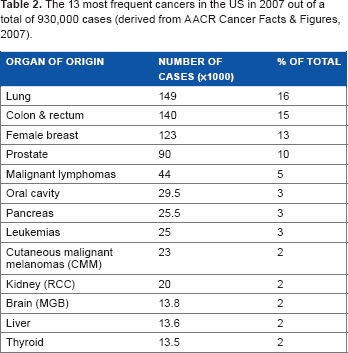
A comparison between Tables 1 and 2 shows that there is a significant difference between the frequency of inadvertently transplanted malignancies and those occurring in the “normal” population. The most commonly transplanted malignancy is cutaneous malignant myeloma (CMM), which is the ninth most common cancer in the normal population. The second most transplanted cancer is renal cell carcinoma (RCC), which is the tenth most common cancer on the frequency list.
CMM Transmitted via Transplanted Organs
In several of these cases, the donor did not have any known CMM or had had a CMM removed such a long time before organ donation that the donor was regarded as cured. The disease-free interval was 10 years or more, and the donors' organs were considered free of tumor cells. The IPITTR published the first of these cases.26,29 Organs from 13 patients who had had a CMM more than 10 years before organ donation were transplanted into 28 recipients. Twenty-one of the recipients (75%) developed generalized CMM, and 13 of them succumbed to CMM. The metastases in the recipients had grown to a diagnostic level by about 10 months after the transplantation (range: 2.5–42 months). In the eight survivors, the transplanted organ was surgically removed, the immunosuppression was discontinued, and the remaining malignant cells were rejected by the recipient (a regular host versus graft rejection).
Two of these cases where CMM was transferred are particularly interesting. In the first case, the donor had no known CMM. 31 She had died from a cerebral hemorrhage, and her liver, heart, and both kidneys were transferred to four individual recipients. All the four recipients developed generalized CMM within a year, and all of them died from the malignancy. In the second case also, the female donor had no known CMM. 32 Her liver, heart, and both kidneys were also transferred to four recipients. The recipients of the kidneys and liver developed and died from generalized CMM, but the recipient of the heart did not. A third case was published by MacKie et al. 33 The donor had undergone surgery for a CMM 16 years prior to transplantation. She had not had a local reoccurrence or metastasis, and she died from cerebral hemorrhage. Her two kidneys were transplanted to two recipients. Both developed generalized CMM and died from that malignancy. A recent review of transmission of donor CMM by organ transplantation is found in Strauss and Thomas. 34
RCC Transmitted via Transplanted Organs
The second most common unintentionally transplanted malignancy is RCC. In these cases, the donor had no known RCC or had had the primary tumor removed such a long time prior to organ donation that he/she was regarded as cured. In the first two cases published, the donors did not have a known RCC at the time of donation and their malignancies were detected later. In the recipients, the tumor cell population had grown to diagnostic size before the primary malignancy was detected in the donors. Thus, the tumor cell population grew faster in the foreign recipient than in the original host. The chronological sequence of the expansion of the tumor cell populations in the donors versus the recipients is remarkable. A summary of inadvertently transplanted RCC was reported in 2004. 26 In 70 cases, the donors had suffered from RCC but so long ago that they were regarded as cured. Forty-three of the recipients (61%) developed RCC.
Malignant Glioblastoma Transmitted via Transplanted Organs
Malignant glioblastoma (MGB) in adults rarely gives rise to metastases outside the central nervous system (CNS) unless there is a shunt from the brain to the abdomen. 35 In cases with an existing shunt, the tumor cells grow in several of the hosts' abdominal organs, indicating that these tumor cells can survive and grow outside the CNS. Without a shunt, extracerebral metastases occur in only 0.5%–2.3% of cases, almost exclusively in patients younger than 18 years of age. 36 Because metastases to distant organs were so infrequent with this malignancy, it was considered safe to transplant organs from these patients in the early days of transplantation surgery. However, several of the recipients of these organs developed MGB in numerous peripheral organs, such as the bone marrow, lungs, liver, and lymph nodes, but not in the CNS. As of today, about 20 such cases have been published.37–39 The interval between the transplantation and the detection of the transferred malignancy has been short, only a year or two. In the cases where the donor was examined postmortem, no metastases were detected in the peripheral organs. The existence of metastases outside of the CNS in the donor might indicate that the diagnostic biopsies from the primary MGB provided access to other organs.
The Occurrence of Late Metastases in Cancer Patients
Introduction
In the clinical setting, the majority of metastases from malignant tumors are detected within five years of the initial diagnosis of the primary tumor. However, “late metastases” do occur. In the medical literature, “late” is usually defined as >10 years from the removal of the primary tumor and without evidence of a local recurrence at the site of the primary tumor. To explain this latency, it has been assumed that tumor cells can enter a dormant state.
Definition of Dormancy
The term “dormant” was introduced by the Australian pathologist Rupert Willis, 40 but there is no universally accepted definition of the term “dormancy”. Dormancy of cells may be defined as a nonproliferating state or an arrest in the cell cycle that results in a prolonged G0 phase. It has also been termed “a temporary mitotic arrest.” 41 Quiescence, which is induced via different mechanisms such as withdrawal of growth factors and loss of adhesion mechanisms, is simply not equivalent to exit from the cell cycle. Quiescence includes suppression of differentiation and, unlike senescence, is reversible. Dormancy is a reversible state and is not to be mistaken for senescence, which is irreversible. 42 If one accepts the term “late metastases” to indicate a period exceeding 10 years from the removal of the primary tumor, then the two malignancies in which this occurs most frequently are CMM and RCC.
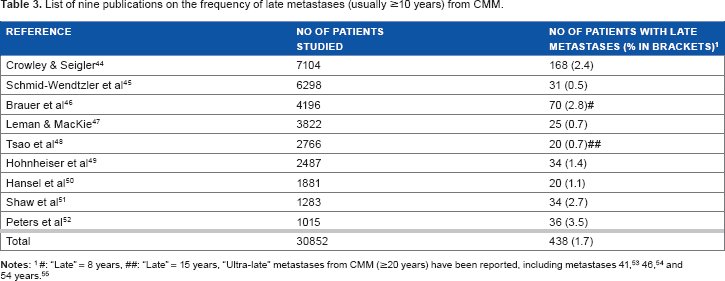
Late Metastases from CMM
Late Metastases from RCC
RCC is a heterogeneous group of malignant tumors, the growth rates of which are highly variable. Most metastases, however, occur within 10 years after removal of the primary tumor. Approximately 75% of the afflicted patients die from their disease and 25% are “cured” by surgery (the word “cure” here denotes patient survival after five years, which is not a true cure). Late metastases can occur; McNichols et al 56 found in their analysis of 506 patients that 78% of the metastases occurred within five years and 11% (18 patients) occurred after more than 10 years. 56 Of these 18 patients, 15 died of metastatic disease within one month to two years after the metastases were diagnosed, which is indicative of fast-growing tumor cell populations. This growth rate is in contrast to the long latency period in the original host.
Almost 50 case reports of “late” metastases from RCC have been published. “Late” has usually been arbitrarily defined as ≥10 years after radical nephrectomy. Thirteen cases with late metastases and a disease-free survival (DFS) of more than 20 years have been published, with the longest being 31, 57 38, 58 45, 59 and 50 years. 60 Two recent reviews of these cases have been published.61,62 In these clinical cases, late metastases are usually attributed to dormant tumor cells. However, some RCCs are very slow growing with tumor volume doubling times of 300 days or more. With such a slow growth rate, it may take decades–-not years–-for a single cell to reach the diagnostic level (0.2–1.0 cm in diameter). Thus, some of these late metastases may not depend on dormancy.
When do Malignant Tumors in Humans Start to Metastasize?
Summary of seven publications on the estimated time point of the first dissemination of human malignant tumors.
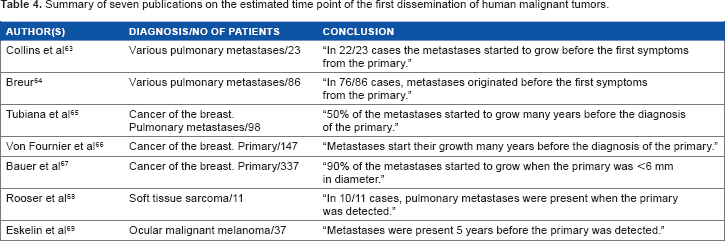
The conclusions from these seven publications are converging, and it appears that the majority (>75%) of human malignant tumors are already disseminated when the primary tumor is detected.
Discussion
Medical professionals, including biologists and researchers, might have initially been skeptical of these cases of inadvertently transmitted malignant tumors. Most malignant tumors that metastasize do so within five years after the primary tumor has been detected, so this raises the question of how one can explain “dormancy” among tumor cells for decades. One consequence of this skepticism is that some of these “late” recurrences may have been classified as “tumors of unknown primary.” In Australia, where CMM is a common malignancy, cancer of unknown primary is the seventh most common oncologic diagnosis. 70 The truth may be, in fact, that some of these cases were actually late metastases from a CMM that had been removed decades earlier, and this could be a potential error in mortality registers.
Cases with long tumor-free intervals between the removal of the primary and the detection of the secondary tumors in the original host, and cases where a transplanted organ has transferred a malignant tumor to the foreign recipient, point to the existence of control mechanisms that can block the proliferation of disseminated tumor cells. However, once transferred to another host, this block can be removed and the tumor cells can start to proliferate, sometimes at a higher rate than that in the original host. As described above, the two cases reported by Stephen et al 31 and Morris-Stiff” et al 32 are most thought-provoking; neither of the two donors had a known CMM, but seven of the eight recipients of their organs developed generalized CMM and died from the malignancy. The one recipient who did not develop CMM had received the donor's heart.
In the cases where the organ donor had succumbed to MGB, it must have been assumed that there were no disseminated tumor cells in the donor's peripheral organs. However, such cells were present in quite a number of the donor's organs because several of the recipients developed the donor's malignancy regardless of whether the transplanted organ was a heart, a kidney, or a liver. The diagnostic and/or therapeutic efforts against the tumor while it was still within the donor must have opened up the communication between tumor cells and non-CNS organs. Thus, one may ask why such generalized metastases from MGB are so rare. The American neuropathologist EC Alvord 71 offered an answer. MGB is frequently multifocal,72,73 and the biopsy is usually taken from the largest of these foci for diagnostic purposes. This focus is later removed as part of the primary therapy. If generalized metastases are shed during the biopsy or the removal of the largest focus, they might not have reached diagnosable size in other organs before the patient succumbed to the remaining foci in the brain. Thus, generalized metastases existed in the patient but remained undetected at the postmortem examination. The donor succumbed to the MGB before the metastatic cells had grown to a diagnosable level.
The two most frequent unintentionally transplanted malignancies–-CMM and RCC–-pose a paradox. They are two of the most malignant tumors that exist in humans, and both are almost 100% fatal once generalized. Death also comes quite rapidly, especially in the case of CMM. Paradoxically, however, both of these malignancies can have clones of cells that can remain dormant for decades only to start proliferating again once transferred to a foreign host. Not infrequently, the transplanted tumor cell population grew faster in the recipient than in the original host despite the fact that they are growing against the immune barrier–-albeit weak–-of the recipient. No matter how careful the selection of the donor has been to match the antigens of the recipient, a transplantation barrier always remains.
The kidneys and heart pose another paradox. Metastases to these two organs are seldom encountered clinically,40,74 which is surprising because 25% of the heart's minute volume is filtered through the narrow mesh of the glomeruli. Billions of circulating cancer cells face the fate of being trapped in the kidney, but clinical metastases to the kidney are still very rare events. However, transplanted kidneys show that metastatic tumor cells can not only exist in these organs but also survive there for decades without proliferating. In autopsy studies, however, the picture is different from the clinical one. Here, where patients have died from their widespread malignancies, the kidneys are the fifth most common site of metastases, occurring in up to 20% of the cases. 75 The heart is another organ considered to be a very rare localization for metastases. However, it turns out that the heart is frequently involved in malignancies (up to 50% in autopsy series). The most common type is–-again–-CMM.76–79 Some of the publications cited above dealing with inadvertently transplanted tumors have been criticized: “based on single observations,” “small numbers,” “selected populations,” “shifting immunosuppression over the years,” “inexact risk estimates,” and so forth. These objections notwithstanding, the cases described above allow some important conclusions to be drawn.
Dormancy is often regarded as an uncommon phenomenon. On the contrary, it is so common that it has been appointed as one of the two prerequisites for life. 80 Species that have not had the capacity to retreat into dormancy (torpor) whenever faced with unfavorable or dangerous environments (lack of oxygen, lack of nutrients, unfavorable temperature, light, moisture, pH, etc) have been eliminated during evolution. Dormancy has been shown to occur in viruses, bacteria, fungi, plants, amphibians, insects, fishes, reptiles, birds, and mammals. If human malignant tumors follow the same rules that apply to evolutionary processes in other organisms, then a state of dormancy in the tumor cells may be a rescue path from hostile microenvironments. 81 Evidence indicates that dormant, microscopic tumors not only are common in cancer patients but also can exist in otherwise healthy individuals. Due to their small size and noninvasive nature, these dormant tumor cells remain asymptomatic and, in most cases, undetected. However, the dormant state is labile, and a number of factors can trigger proliferation. Several mechanisms that induce or reverse dormancy in malignant tumor cells have been discovered, and these have been explained in many extensive and excellent reviews.82–92 These mechanisms can operate separately or in collaboration, and they can be genetic as well as epigenetic. Not infrequently, the epigenetic factors have been dietary ingredients, such as the curry spice (Curcumin), soybean extract, or vegetables (Broccoli).93–96
Dormant cancer cells share numerous characteristics with cancer stem cells, and the two may represent two sides of the same coin. 97 They constitute a lifelong threat to the patient's life. The term “cancer without a disease” is appropriate. 98
The cases with inadvertent transmission of human malignant tumors support the results from experiments with molecular genetics and mathematical models/simulations that point to early dissemination.99–102
The risk of an inadvertently transmitted malignancy from a donor to an organ recipient might seem alarming and has received some attention in the media. However, that risk is overestimated. Today, that risk is actually very small (0.01%–0.05.). The risk of dying during the first year while on the waiting list for a life-saving organ is considerably larger and ranges from 2% for kidney candidates to 17% for lung candidates, according to Desai et al. 103
Israel Penn, 12 the founder of the first transplantation registry, stated that, “Transplantation surgery has contributed to our knowledge of cancer,” in which we concur.
Conclusion
Disseminated tumor cells frequently exist in the original host prior to the detection of the primary tumor.
Metastatic cells can reside in organs that are not usually the site of secondary tumors, that is, the kidneys and the heart.
Metastatic cells in the original host can remain dormant for decades after the primary tumor has been removed.
The mechanisms capable of inducing dormancy may be reversible, leading to late recurrences.
Author Contributions
Conceived and designed the experiments, analyzed the data, and wrote the first draft of the manuscript: SF. Contributed to the writing of the manuscript, agreed with manuscript results and conclusion, jointly developed the structure and arguments for the paper, and made critical revisions and approved final version: SF and AN. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgment
Karolinska Institutet is gratefully acknowledged for the generous support of this work.