
Abstract
A woman in her 50s was referred to our department with the chief complaint of nasal congestion and pharyngeal discomfort. The patient had been diagnosed with sleep apnea at the Department of Internal Medicine, and had undergone nasal continuous positive airway pressure (nCPAP) therapy, but her response to the treatment was poor. A cystic lesion occupying the nasopharynx, which was detected by nasopharyngeal fiberscopy, computed tomography, and magnetic resonance imaging, was thought to be the cause of the nasal congestion, pharyngeal discomfort, and obstructive sleep apnea syndrome (OSAS). Consequently, the patient underwent extirpation of the lesion under general anesthesia for the purpose of obtaining a definitive diagnosis as well as for treatment of the nasopharyngeal tumor. The diagnosis of intra-adenoid cyst was eventually made based on the pathological findings, which revealed lymphoid tissue accompanied by expansion of the crypt, as well as inflammatory cell infiltration with follicular hyperplasia. After the operation, the patient reported subjective improvement of her symptoms, and began to respond to the nCPAP therapy for her sleep apnea syndrome. Nasopharyngeal cysts, in particular adult intra-adenoid cyst, are relatively rare. The outcomes of the current case indicated that the presence of a nasopharyngeal cystic disease was hampering the nCPAP treatment of refractory OSAS.
Introduction
Differential diagnoses for the relatively rare nasopharyngeal cysts include Tornwaldt's disease, Rathke's cleft cyst, intra-adenoid cyst, branchial cysts, and pseudocysts. 1 Here we report a case in which the presence of nasopharyngeal cysts was indicated as hampering nasal continuous positive airway pressure (nCPAP) treatment of refractory obstructive sleep apnea syndrome (OSAS).
Nasopharyngeal cysts are comparatively rare, and most do not exhibit themselves but are found incidentally. However, various symptoms, such as nasal congestion, apnea, and hearing loss, may be exhibited depending on the developing site due to increasing cyst diameter. 1 Diagnosis is often difficult and is comprehensively determined by the site of occurrence, characteristics of the cyst surface, and tissue findings. Tornwaldt's disease, Rathke's cleft cyst, pharyngeal tonsil central fossa cyst, branchial cysts, and pseudocysts are raised as differential diagnosis. 2 The frequency of occurrence of nasopharyngeal cysts has not been previously mentioned, but in one report it was observed that this occurs in 1.4%–3.3% cases of Tornwaldt's disease by autopsy. 3 Moreover, according pathophysiological findings, nasopharyngeal cysts can be classified as congenital when occurring in the pharyngeal bursa vestigial remnant or Rathke's pouch, or as acquired as a result of infection or surgery. 4
We recently encountered a case that suggested nasopharyngeal cysts as the cause of treatment-resistant OSAS. Here, we report it including bibliographic considerations. The patient has given verbal consent for publication of this report.
Case Presentation
A woman in her 50s was referred to the Otorhinolaryngology Department, Kyorin University, with the chief complaint of nasal congestion and pharyngeal discomfort. Her past history included hypertension and sleep apnea syndrome (SAS). Her weight and height were 70.0 kg and 153 cm, respectively, with a BMI of 29.9 kg/m2. The patient had been experiencing nasal congestion for approximately 20 years, but had opted against seeking treatment. A local internist diagnosed the patient with SAS in June 2010, and initiated nCPAP therapy. However, this therapy was discontinued because of the lack of effectiveness. Consequently, the patient experienced exacerbation of her nasal congestion, and chose to visit a local otolaryngologist. A tumor lesion was discovered in the patient's nasopharynx, and the doctor referred her to our department.
The initial clinical findings following nasopharyngeal fiberscopy included the presence of an oval tumor with a grooved surface in the nasopharynx, which was not associated with the Eustachian orifice (Fig. 1A, B). The results of laboratory blood analyses revealed no evidence of an inflammatory reaction. In order to examine the cause of the hypertension, serum levels of thyroid-stimulating hormone (TSH), free thyroxine, free tri-iodothyronine, epinephrine, norepinephrine, dopamine, aldosterone, and renin were analyzed. However, these were all within normal limits. Cytological results of an aspiration biopsy indicated ciliated columnar epithelial cells with mildly enlarged nuclei. A culture of the cyst contents resulted in the detection of coagulase-negative Staphylococci of 1+, and Staphylococcus aureus (MSSA) of 1+.

Nasopharyngeal fiberscopic findings (at the initial examination). An oval tumor with a grooved surface occupied the nasopharynx, but did not cause an Eustachian orifice.
Noncontrast computed tomography (CT) imaging findings included the detection of a partially fluid-filled cystic lesion in the nasopharynx that had its base on the median part. A cystic lesion was detected by magnetic resonance imaging (MRI), the contents of which were hypointense and relatively hyperintense on the T1- and T2-weighted images, respectively (Fig. 2).

CT (noncontrast). A cystic lesion that had its basal part on the median in the nasopharynx was detected. A part of the lesion was fluid-filled. In MRI, a cystic lesion was detected, the contents of which were hypointensive and relatively hyperintensive on the T1- and T2-weighted images, respectively.
Extirpation of the lesion was performed under general anesthesia. Because no clear contents of the tumor lesion could be aspirated by centesis, the anterior wall of the tumor was dissected by forceps to allow removal of the contents. After debridement using a KTP laser to control the bleeding, the cyst was totally extirpated.
The histopathological findings following hematoxylin– eosin (H…E) staining included the detection of lymphoid tissue accompanied by expansion of the crypt, as well as inflammatory cell infiltration and follicular hyperplasia (Fig. 3A, B). The expression of CD4, CD8, CD20, BCL-2, and CKAE1AE3 was evaluated using immunohistochemistry, and the results indicated the presence of CD20-positive B cells in the follicles, CD4-positive helper T cells in the interfollicular region, and cytokeratin in the lymphoepithelial symbiosis aspect of the crypt. Also, the expression of CD8 and BCL-2 was detected, which indicated continued immune function of the pharyngeal tonsils in an individual over the age of 50 (Fig. 3C, D, E, F, and G). Nonetheless, the association with the sacculation was unclear.
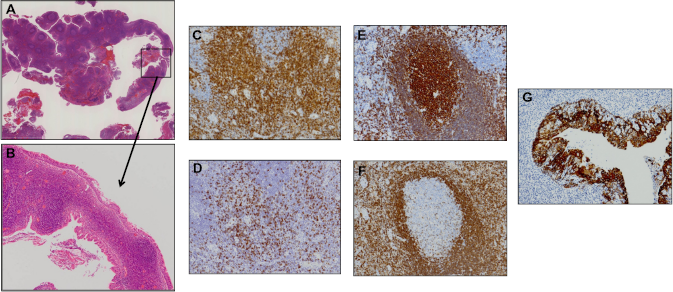
Histopathological findings. H…E staining under (
Thirty-three months following the operation, the patient's nasal congestion disappeared and she was able to get sound sleep. Further, nasopharyngeal findings confirmed the disappearance of the nasopharyngeal cyst. In addition, the patient's systolic blood pressure improved from 140–160 to 120–140 mmHg. However, her body weight and BMI increased to 72.3 kg and 30.9 kg/m2, respectively. A polysomnography (PSG) showed an Apnea Hypopnea Index (AHI) of 26.6 before the operation. It meant that the patient had moderate disorder. PSG was conducted again 12 months after the operation. However, AHI was still 26.4, and we could not see any improvement.
Discussion
Nasopharyngeal cysts are comparatively rare, and most do not exhibit themselves but are found incidentally. However, various symptoms, such as nasal congestion, apnea, and hearing loss, may show up depending on the developing site due to increasing cyst diameter. 1 Diagnosis is often difficult and comprehensively determined by the occurring site, characteristics of the cyst surface, and tissue findings. 2 Differential diagnoses for nasopharyngeal cysts include Rathke's cleft cysts, pseudocysts, Tornwaldt's disease, branchial cysts, intra-adenoid cyst, abscesses, and retention cysts (Table 1). 2
Character, pathology, and radiological findings of nasopharyngeal bursae and cysts.

A Rathke's cleft cyst is a benign growth in the Rathke's pouch, which is the opening of the craniopharyngeal duct to the pharynx during the embryonic period. Rathke's cleft cyst is usually completely occluded by the second month of embryonic development. In most cases, the site of development is localized to the intrasellar region of the sella turcica, or the intrasellar and suprasellar regions, of which the latter accounts for 70%. Further, the development of a Rathke's cleft cyst in the suprasellar region is rare. CT findings have shown low attenuation areas in a majority of the cysts and capsular enhancement in nearly half of the cysts. However, calcification of the cysts is rare. MRI findings have indicated that two-thirds of the cysts are hyperintensive, while the remaining one-third are hypointensive on the T1-weighted image, whereas about 50% are hyperintensive on T2-weighted images. Gadolinium (Gd) contrast agents are said to bring about the contrast effect. However, many cases are asymptomatic, and the overall incidence is approximately 0.4%. 5
Pseudocysts are caused by brain hernias, teratomas, and meningiomas that escape from the persistent craniopharyngeal duct. Pseudocysts can be differentiated from other cysts by using diagnostic imaging to confirm the contents. No specific site of development is apparent with pseudocysts.
Tornwaldt's disease is characterized by the presence of inflammation or an abscess of the embryonic remnant cyst in the area between the front end of the notochord and the nasopharyngeal epithelium between the bilateral anterior vertebral muscles on the posterior median nasopharyngeal wall. According to previous reports, Tornwaldt's disease is more prevalent in individuals aged between 20 and 30 years, with overall incidence ranging from 0.2% to 5.0%. 3 The lesion is located on the medial aspect of the nasopharynx and has a smooth surface. CT scans of the lesion reveal high attenuation areas because the cyst's contents often include blood and an elevated protein concentration. The lesion is hyperintensive on T1- and T2-weighted MRI images, but Gd contrast agents show no contrast effect. Histopathologically, the lesion is covered with a respiratory epithelium without lymphoid tissue, and ranges in size from 2 to 30 mm in diameter. 2
Branchial cysts develop from remnants of the second branchial groove and are usually unilateral but occasionally bilateral. The difference between branchial cysts and other nasopharyngeal cysts is latter's development on the lateral nasopharyngeal wall. Bailey classified the cysts into four types based on the relative position of the cyst: sternocleidomastoid muscle, internal jugular vein, jugular vein, and the pharynx. Among the different classes of branchial cysts, type IV is designated as a nasopharyngeal cyst. 6 Histopathologically, the lesions exhibit lymphocytic infiltration and the formation of lymph follicles. CT scans reveal low attenuation areas. Further, the lesion is hypointensive and hyperintensive on the T1-and T2-weighted MRI images, respectively, but Gd contrast agents show no contrast effect.
Intra-adenoid cysts are caused by mechanical or inflammatory occlusion of an embryonic groove (central fossa) on the pharyngeal tonsil before lymphoid tissues appear. Their prevalence is 6%, 1 and they develop on the posterior nasopharyngeal wall. They are characterized by grooved surfaces. Histopathologically, crypts possess lymphoid tissue, and are characterized by columnar as well as squamous and columnar epithelium.
In MRI without contrast, the crypts appear hypointensive and hyperintensive on the T1- and T2-weighted images, respectively, whereas Gd contrast agents exhibit no contrast. Nevertheless, in many cases the intra-adenoid cysts are difficult to distinguish from Tornwaldt's disease. For that reason, Tornwaldt's syndrome, including intra-adenoid cyst and Tornwaldt's disease, was proposed in a previous report. 7
Different types of nasopharyngeal cysts can be ascertained from the site of their development (Fig. 4). Rathke's cleft cysts are located in the cranial area. Beneath them are intra-adenoid cysts, followed by Tornwaldt's disease, and branchial cysts are located in the lowermost area among them.

Position of cysts in the nasopharyngeal area.
The cysts are characterized by their development on the medial wall of the nasopharynx, except for branchial cysts which develop on the lateral wall.
In the present case, because the lesion was nasopharyngeal and cystic, and the contents were hypointensive on the T1- weighted MRI images and relatively hyperin-tensive on the T2-weighted images, we ruled out Rathke's cleft cysts. Branchial cysts were also excluded because the basal portion of the cyst was located on the median of the nasopharynx, and a grooved surface was present according to the nasopharyngeal fiberscopy and CT findings. Pseudocysts, Tornwaldt's disease, and retention cysts were eventually ruled out because, according to the histopathological findings, the lesion possessed lymphoid tissue with follicular hyperplasia. Therefore, we diagnosed the lesions as crypts in the nasopharynx.
Regarding the relationship between SAS and nasopharyngeal tumors, the latter are detected at a rate that is approximately four times more frequent in SAS patients than in the general population. Furthermore, according to a previous report, a tumor or cystic disease causes complications in the upper respiratory tract in 0.24% of SAS patients. 8 As a clinical condition of hypertension accompanying sleep apnea, sympathetic nerve stimulation due to hypoxemia is considered to be related, 9 but no abnormality was observed in the preoperative serum hormone concentration (E and EN). However, since blood pressure decreased postoperatively, a cystectomy was performed for nCPAP function, and this is thought to have contributed to a decrease in blood pressure.
However, SAS was caused not only by obstructions but also by a central nervous system factor. In addition, AHI unfortunately did not improve in our patient because there was no change in her body weight. Investigation of a possible nasopharyngeal lesion is considered particularly useful for the nCPAP treatment of refractory OSAS.
Conclusions
We treated a case in which a cyst occupied the nasopharyngeal space and caused nasal congestion. The symptoms improved after the surgical removal of the cyst. Histopathologically, the cyst was located on the median of the nasopharyngeal space and showed hyperplasia of lymph follicles. Therefore, we diagnosed it as an intra-adenoid cyst, which resulted in continued immune function of the pharyngeal tonsils in an individual over the age of 50. Finally, the presence of a nasopharyngeal cystic disease was determined as the cause that hampered nCPAP treatment of refractory OSAS.
Author Contributions
Conceived and designed the experiments: HY. Analyzed the data: YM, HY, TI, MF, HK. Wrote the first draft of the manuscript: YM, HY. Contributed to the writing of the manuscript: HY, HK, NK. Agree with manuscript results and conclusions: YM, HY, TI, MF, HK, NK. Jointly developed structure and arguments for the paper: YM, HY, TI, MF, HK, NK. Made critical revisions and approved final version: YM, HY, TI, MF, HK, NK. All authors reviewed and approved of the final manuscript.