
Abstract
A 60-year-old female experienced the gradual onset of left hip pain without any triggering event. Radiographs showed vertical sclerosis in the center of the femoral head and the lesion inside the boundary demonstrated diffuse bony sclerosis. No collapse was observed at the weight-bearing portion on radiograph. However, computed tomography showed a subchondral collapse at the medial lesion. On T2-weighted magnetic resonance imaging, the necrotic lesion showed diffuse high-intensity signals that indicated a prominent repair process. Bone biopsy diagnosed osteonecrosis with associated prominent appositional bone and vascular granulation tissue.
Introduction
Osteonecrosis of the femoral head (ONFH) is a debilitating disease that can often lead to mechanical failure, with collapse of the articular surface and structural joint deformity.1,2 However, some cases of ONFH remain asymptomatic if the necrotic lesion undergoes no collapse.
The prognosis of ONFH largely depends on the location and width of the necrotic lesion. When this lesion involves over two-thirds of the weight-bearing area of the femoral head, the rate of collapse has been reported to be around 94%. 3 On the other hand, necrotic lesions occupying less than the medial two-thirds of the weight-bearing area have low risk of collapse around 19%. 3
We herein describe a case of medially located ONFH with an associated collapsed medial lesion. The patient was fully informed that her data would be submitted for publication, and she consented.
Case Presentation
A 60-year-old female (height, 158 cm; weight, 58 kg; BMI, 22) presented with gradually worsening left hip pain. There was no history of antecedent trauma, corticosteroid usage, or alcohol intake. Hip range of motion was not restricted. A T-score for bone mineral density based on the lumber spine was –-1.5 SD, indicating the normal bone mass.
A radiograph obtained 12 months after the onset of pain showed vertical sclerosis in the center of the femoral head, and the lesion inside the boundary demonstrated diffuse bony sclerosis (Fig. 1). No collapse was observed at the weight-bearing surface of the femoral head, but joint space narrowing was recognized in the medial portion. T1-weighted magnetic resonance imaging (MRI) showed a vertical low-intensity band corresponding to the sclerotic rim on the radiograph (Fig. 2A). On fat-saturated T2-weighted images, a diffuse high-intensity area was observed within the medial lesion (Fig. 2B).

Radiograph of the left hip joint at 12 months after the onset of pain. The anteroposterior view shows vertical sclerosis running from the top of the femoral head to the femoral neck (black arrow). A lesion inside the boundary demonstrates diffuse sclerosis. Medial joint space narrowing is also apparent (white arrow).

MRI images at 12 months after the onset of pain. (
Computed tomography (CT) showed a subchondral collapse at the medial lesion (Fig. 3A, 3B).

CT images (2-mm slices) at 12 months after the onset of pain. (
A biopsy specimen (Fig. 4) was obtained to confirm the diagnosis, using a 6-mm diameter biopsy needle that was advanced from the distal portion of the greater trochanter to the medial lesion of the femoral head. Histologically, osteonecrotic bone trabeculae covered by appositional bone formation were seen within the lesion (Fig. 5), and the bone marrow tissue contained vascular-rich fibrous tissues. Based on these findings, the diagnosis of ONFH was made.

A biopsy specimen obtained using a 6-mm diameter biopsy needle. The (
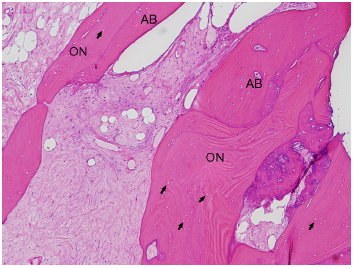
Histological appearance of the femoral head (hematoxylin and eosin staining, 40×). Osteonecrotic bone trabeculae (ON) show empty lacunae (black arrows) and are surrounded by vascularized fibrous tissue in combination with appositional bones (AB).
The patient was treated with celecoxib 200 mg/day for 4 months, and her hip pain gradually decreased. The latest radiograph 9 months after biopsy showed neither progression of collapse nor joint space narrowing.
Discussion
A high signal intensity on fat-saturated T2 images generally suggests a lesion with a rich vascularity or an edematous area including bone tumor. The possible tumor developing within the femoral head may include chondroblastoma and osteoid osteoma. Chondroblastoma is a rare bone tumor, arising from the secondary centers of ossification of long bones. The proximal femur is reported to be a common site of developing the tumor. Since a lytic lesion surrounded by sclerotic border is considered to be diagnostic features, some cases may be confused with ONFH. 4 Osteoid osteoma usually occurs near the metaphysis rather than the epiphysis, and appears as a radiolucent nidus showing high signal intensity on T2 images, accompanied by bone marrow edema. 5 Although the imaging findings of our cases seemed to be less similar to those of the tumors, we were unable to make a diagnosis of ONFH due to the atypical imaging findings. Then, we decided to perform the bone biopsy to clarify a diagnosis of our case. Microscopically, the high-intensity area consisted of abundant vascularized fibrous tissue in combination with thickened trabeculae, indicating the reparative condition of the necrotic lesion.
Osteonecrotic lesions involving the medially located non-weight-bearing area generally remain asymptomatic. It has been reported that necrotic lesions occupying less than the medial two-thirds of the weight-bearing area have low risk of collapse to be around 19%. 3 In addition, such osteonecrotic lesions generally tend to be repaired over time if they do not undergo collapse, 6 and repaired necrotic lesions show osteosclerotic changes. 7 In our case, most of the necrotic lesion was repaired by prominent appositional bone formation. However, collapse was observed at the medial non-weight-bearing portion.
Motomura et al. 8 reported that collapse consistently involved fracture at the lateral boundary of the necrotic lesion, at the junction between the thickened trabeculae of the reparative zone and the necrotic bone trabeculae. In the current case, on the other hand, an axial CT slice showed a fracture at the anteromedial junction between the thickened trabeculae and the necrotic bone trabeculae, against the anterior edge of the acetabulum. We speculated that collapse might have been caused by the repetitive mechanical stress between the anterior edge of acetabulum and the anteromedial necrotic lesion adjacent to the thickened trabeculae of the reparative zone.
Regarding the mechanisms of collapse in ONFH, Kenzora and Glimcher 9 reported that a fracture may begin in the region of the resorbed necrotic subchondral plate at the lateral junction between necrotic and viable bone. In our case, CT showed some degree of bone resorption around the collapsed lesion, whereas diffuse bony sclerosis was seen in the necrotic area, indicating that osteonecrotic area has been repaired. Further studies are necessary to conclude whether subchondral bone resorption antedates the collapse in ONFH.10,11
Regarding the distribution of the necrotic area in ONFH, several studies have suggested the importance of vessels feeding the femoral head.12–15 The superior retinacular artery is known to be the principal source of blood to a large area of the femoral head, including the weight-bearing area of the superior portion.12,13 On the other hand, the inferior retinacular artery (IRA) has also been reported to contribute to the vascularity of the femoral head.14,15 Boraiah et al. reported that the IRA feeds 62% of the medial half of the femoral head. 14 Furthermore, Liu et al. 15 reported that necrotic lesions tended to occupy the medial two-thirds or less of the weight-bearing area when the IRA was damaged. The medial location of the necrotic area in our case might have resulted from a disturbance of the IRA.
Author Contributions
Wrote the first draft of the manuscript: KK. Contributed to the writing of the manuscript: KK, TY, GM, RY. Agreed with manuscript results and conclusions: KK, TY, GM, YN, AS, RY, YI. Jointly developed the structure and arguments for the paper: KK, TY, GM, YN, AS, RY, YI. Made critical revisions and approved final version: KK, TY, GM. All authors reviewed and approved the final manuscript.