
Abstract
We present the case of a 65-year-old female who presented to our hospital with nodular swelling in her breast that first appeared in the right upper quadrant 10 months earlier, followed by involvement of the left upper quadrant along with nodular swelling in the right inguinal region for the past six months. She was also complaining of breathlessness on exertion and right-sided pleuritic chest pain for the past one year. Her chest X-ray showed well defined consolidation in the right lower lobe of the lung with pleural effusion. Further pleural tap showed malignant cells with squamous differentiation. Fine needle aspiration cytology (FNAC) from breast lumps was suggestive of malignant cells with morphology of cells likely to be squamous. CT-guided biopsy of the lung mass showed moderately differentiated squamous cell carcinoma of the lung. She succumbed to her illness following severe respiratory distress. Breast lump secondary to lung malignancy is very rare. Squamous cell carcinoma presenting as breast metastasis is a very rare presentation and reported in few cases. No previous case reporting bilateral breast lumps as a presentation of squamous cell carcinoma of the lung could be found in the literature.
Introduction
Breast metastasis secondary to extramammary neoplasms are rare, with an incidence of only 0.5–3%.1,2 Most such cases are hematological malignancies including leukemias and lymphomas.3,4 Carcinoma of the lung is a very rare cause of breast metastasis. Breast metastasis often simulates primary breast malignancy. Prompt differentiation of metastatic breast carcinoma from primary breast carcinoma is important because the treatment and prognosis differ significantly. Small cell carcinoma and adenocarcinoma of the lung are reported to rarely manifest as metastatic breast lumps but no case has been reported of squamous cell carcinoma presenting as bilateral breast metastasis. This case highlights the possibility of the breast lump as a presenting manifestation of metastatic lung carcinoma. The authors have obtained specific informed written consent of the patient's relative in regard to the publication of the case report, as the patient is deceased. Every care has been taken in the photography and description to avoid personal identification of the patient.
Case Presentation
A 65 year old female presented to our hospital with complaints of breathlessness on exertion and right sided pleuritic chest pain lasting for one year. There was also a history of off-and-on low grade fever and dry cough but no hemoptysis. She also had significant loss of appetite and weight loss of around 10 kg in the past one year. Her symptoms had increased in severity in the past three months. Ten months earlier she noticed a nodular swelling in the right upper quadrant of her breast followed by involvement of the left upper quadrant. Swelling was painless, non-tender, and mobile. This was followed by the appearance of cutaneous nodules in the inguinal region. In the course of time, the breast lesions turned hard and the overlying skin ulcerated. On examination of the breast, a serosanguinous type discharge was present at the ulcer site. The patient was a non-smoker and non-diabetic. There was no history of tuberculosis or any other illness in her past. However, the patient's daughter died of endometrial cancer at the age of 42 years. There was no other history of malignancy in the family.
On examination, the patient's general condition was poor. General physical examination revealed mild pallor. There was no icterus, cyanosis, clubbing, lymphadenopathy, or edema. Local examination of the breast revealed bilateral enlarged breasts along with ulcerating lesion over the right and left upper quadrants with serosanguinous discharge and underlying mass 3 × 3 cm in size. Mass was fixed to the overlying skin and was non-tender on palpation. There was no axillary lymphadenopathy. There was another 2 × 2 cm painless non-tender nodule present in the midline below the umbilicus in the right inguinal region fixed to the skin and the surrounding skin was puckered. Chest examination revealed decreased air entry with few crepitations present on the right side. Cardiovascular system and abdominal examination revealed no abnormality.
Complete blood counts revealed: hemoglobin – 8.4 gm%, total leukocyte count –19280 cells/cumm, differential leukocyte count – polymorphs 92%; lymphocytes 6%; monocytes 1%; eosinophils 1%, and platelets – 3.77 lakhs per cumm. Ertyhrocyte Sedimentation Ratio (ESR) was high at 113 mm in the 1st hour. Kidney function tests and liver function tests were within the normal limit.
Chest X-ray was suggestive of a well defined consolidation of the right lower lobe with pleural effusion.
The patient was carrying an extrahospitalary PET-CT scan, which revealed a soft tissue density mass with increased Fluorodeoxy Glucose (FDG) uptake and central necrosis involving the lower lobe of the right lung, 4.6 × 2.8 cm in size, abutting the oblique fissure. Contiguous thickening with mild FDG uptake was seen extending along the oblique fissure to the periphery. An irregular pleural based consolidation with interspersed air bronchogram showing mild peripheral uptake and central necrosis was seen in the right lower lobe adjacent to the mass lesion. A few irregular infiltrates were also seen in the adjacent lung parenchyma with mild right sided pleural effusion.
Induced sputum for acid fast bacilli tested negative. Fine needle aspiration cytology from the breast lesion showed clusters of malignant cells with the morphology not very clear. Further marker for breast cancer, the CA-15–3 level was normal at 30.08 [normal range: 0–35].
Pleural fluid analysis was done, which showed 80 cells, P60 L40, sugar – 7 mg%, proteins – 3.6 gm%, and Adenosine Deaminase (ADA) – 34. Cytology revealed atypical cells with squamous differentiation in the necrotic background.
Later an excisional biopsy of the breast lesion showed moderately differentiated squamous cell carcinoma, likely metastatic in origin (Fig. 1). A decision regarding CT guided lung biopsy was made and it revealed moderately differentiated squamous cell carcinoma of the lung (Fig. 2).
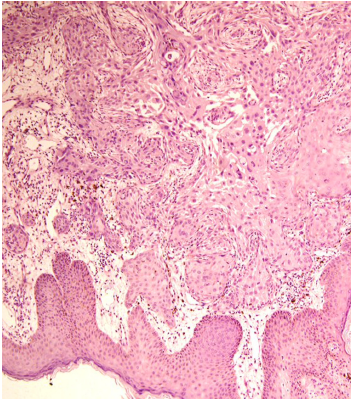
Shows the section of breast tissue infiltrated by a moderately differentiated squamous cell carcinoma. The overlying epidermis is focally infiltrated by the tumor (H & E stain 100×).

Shows the section of lung tissue infiltrated by a moderately differentiated squamous cell carcinoma, morphology similar to breast tissue.
Ultrasonography of the abdomen revealed an enlarged liver 17.5 cm in size, two hypoechoic lesions of 1 × 1 cm noted in segment III of the left lobe of the liver, another 2 cm hypoechoic lesion noted in segment VI, and two 1 cm hypoechoic lesions in segment VII. Ultrasound of the thyroid gland showed that there is evidence of multiple heterogenous hypoechoic nodules in the right lobe of the thyroid with one of them showing peripheral calcification, the largest measuring 1.7 cm in size, with peripheral vascularity. An excisional biopsy of the inguinal nodular lesion was also done and it was suggestive of moderately differentiated squamous cell carcinoma.
The patient was started on conservative treatment including oxygen inhalation via mask, injectable antibiotics, and general care of nutrition. A decision regarding her transfer to the oncology department was made but the patient's condition was deteriorating. Finally, owing to severe respiratory distress and cardio-respiratory collapse, she succumbed to her illness.
Discussion
Metastatic breast lumps secondary to extramammary neoplasms are very rare. Most cases are hematological malignancies including leukemias and lymphomas. Other malignancies including ovary, prostate, stomach, malignant mesothelioma, and rhabdomyosarcoma have been reported in patients with breast metastasis.1–5
Lung carcinoma is an uncommon source for breast metastasis. The incidence of metastasis from non-small cell lung cancer ranges from 11 to 36%. Common metastatic sites are the liver, adrenal glands, brain, bone, kidney, and abdominal nodes.6,7 Other uncommon metastatic sites are the stomach, pancreas, small bowel, arteriovenous hemangioma, choroids plexus, muscle, umbilicus, and penis. Very few cases have been reported where breast metastasis was found secondary to lung malignancy.8–10
To the best of our knowledge, there has been no case report where bilateral breast lumps are the presenting manifestation of underlying squamous cell lung carcinoma of lung. Fine-needle aspiration cytology has been reported to successfully identify both primary and metastatic malignancy in the breast. 11 Although radiology can provide some information to distinguish primary breast cancer from metastatic disease, excisional or core biopsy is usually needed for final diagnosis.
Conclusion
Secondary malignancy metastatic to the breast is uncommon; however, this entity exists and in view of the therapeutic implication, as the treatment and prognosis differ significantly, a metastatic breast lesion should not be mistaken for a primary breast carcinoma. A detailed history regarding concurrent or previous malignancy combined with the clinicoradiological assessment and pathological evaluation is essential to diagnose breast metastasis secondary to other malignancy. Only with the awareness of such a possibility one can make the diagnosis and achieve prompt management.
Author's Contribution
PD and AJ are the treating residents and mainly responsible for the conception and drafting of the case report. AG helped in working up the patient in ward. NG gave conclusive guidance regarding the management of the patient and guided us in the making of this case report.
SK reported the histopathological diagnosis of the lung and skin biopsies.
Author Contributions
Conceived and designed the experiments: PD. Analyzed the data: PD, AJ. Wrote the first draft of the manuscript: PD, AJ. Contributed to the writing of the manuscript: NG. Agree with manuscript results and conclusions: PD, AJ, AG, NG, SK. Jointly developed the structure and arguments for the paper: PD, AJ, NG. Made critical revisions and approved final version: PD, NG. All authors reviewed and approved of the final manuscript
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.