
Abstract
An atrial septal aneurysm (ASA) is a rare but well-recognized abnormality of uncertain clinical relevance. It is a localized bulging of the inter-atrial septum into either or both atria during the cardiac cycle. ASA has been reported as an unexpected finding during autopsy but may also be diagnosed in living patients by echocardiographic techniques.
We present a 37-year-old woman with a recurrent atypical chest pain of one-year duration. She was found to have a congenital atrial septal aneurysm on evaluation. The echocardiographic images mimicked a left sided cor triatriatum sinister. She had no other symptoms and had no co-morbidities. There was no audible murmur.
ASA can mimic cor-triatriatum and echocardiographic examination should be performed from multiple views before any echocardiographic diagnosis is made.
Introduction
The first report on atrial septal aneurysm (ASA) was published by Lang and Posselt in 1934. 1 Since then, several ASA cases and studies have been published in the literature. An ASA is a congenital abnormality that is characterized by a localized bulging of the atrial septum into either or both atria during the cardiac cycle. ASA formation can be secondary to interatrial pressure differences, but may also be a primary malformation involving the region of the fossa ovalis or the entire septum. ASA may be an isolated abnormality but is often found in association with other structural cardiac abnormalities like mitral valve prolapse or atrial septal defects.
Initially, ASA was considered a rare congenital anomaly, but with the advancement of two-dimensional echocardiography, and more recently, broader use of trans-esophageal echocardiography (TEE), detection of this abnormality has become easier and more frequent.
To the best of our knowledge, the only previous report of an ASA mimicking a cor triatriatum sinister was by Ramazan and colleagues. 2 Studies using transesophageal echocardiography (TEE) have shown a prevalence of 2% to 10% for ASA.3,4 Most ASAs are clinically silent, found incidentally in 1% of the general population. 5
Case Report
A 37-year-old African female was referred to the cardiology outpatient clinic with complaints of unresolved atypical recurrent chest pain of one-year duration. The chest pain is non-ischemic and non-dyspeptic in character. No history of palpitations, dyspnoea, cough or syncope was reported. Systemic review revealed no significant findings. She was not known to be hypertensive or diabetic and did not smoke cigarettes or drink alcohol. She did not have any past history of transient ischemic attacks (TIAs). She denied usage of any medications and was not aware of the presence of heart disease among her family members.
On general examination, she was a normal young lady with a body mass index of 24 Kg/m2. Cardiovascular and respiratory systems were examined and found to be normal. Other systemic examinations were essentially normal.
The patient has had several investigations including electrocardiograms, chest radiograph and cardiac enzymes, which were all normal. Laboratory findings were within the normal reference range.
Echocardiography revealed a thickened and myxomatous anterior mitral valve leaflet; however, no definite mitral valve prolapse was seen. In the parasternal long axis view (PLAV), a membrane was seen across the left atrium (LA), extending anteroposteriorly from the base of the anterior mitral valve leaflet to the base of the posterior valve leaflet (Fig. 1). This membrane was not demonstrable within the LA in the apical four chamber and apical two chamber views.
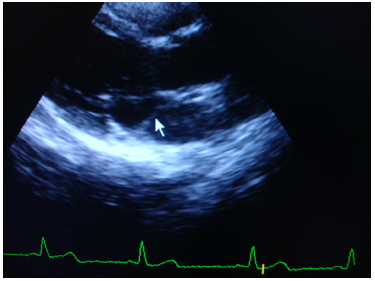
Parasternal long axis view (PLAV) of the LV showing a membrane was seen across the left atrium (LA), extending antero-posteriorly from the base of the anterior mitral valve leaflet to the base of the posterior valve leaflet.
The apical four-chamber view revealed a hypermobile inter-atrial septum with at least a 12 mm excursion in either direction (Figs. 2 and 3). Multiple parasternal long- and short-axis views, an apical four chamber view and modified echocardiographic evaluations including sub-costal views revealed that the membrane bisecting the LA in the PLAV (described earlier) was a cross section of the hypermobile interatrial septum atrial septal aneurysm). We categorized the patient as having a type 5 atrial septal aneurysm (bi-directional and equidistant to the right as well as to the left during the cardio-respiratory cycle; see Figs. 2 and 3).

Apical four chamber view showing hyper mobile inter-atrial septum with 12.3 mm bulging into the left atrium (into both atria; type 5 ASA).
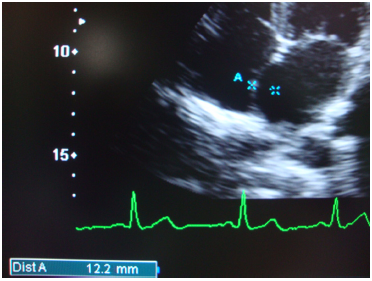
Apical four chamber view showing hyper mobile inter-atrial septum with 12.2 mm bulging into the right atrium (into both atria; type 5 ASA).
There was no demonstrable color jet across the inter-atrial septum. Our patient did not consent to have a TEE, so we commenced on prophylactic aspirin 300 mg daily, which was later reduced to a maintenance dose of 75 mg daily.
Discussion
An ASA usually involves the area of the fossa ovalis.5,6 It is a localized bulging of the inter-atrial septum and the diagnostic criteria is usually a protrusion > 6 mm into the right atrium (RA) or LA or both atriums. 7 Bulging of the entire atrial septum or localized bulging protruding less than 6 mm is not usually considered to be a true aneurysm, since such bulging might be seen in the absence of a true aneurysm. 6 Furthermore, a small pocket 3–6 mm long, extending anteriorly and to the left of the limbus fossae ovalis, has been described anatomically in normal subjects. 8 An aneurysm affecting the entire interatrial septum has never been documented pathologically. Other authors have used a protrusion of the aneurysm > 10 mm beyond the plane of the atrial septum measured by TEE. 3 Our patient had a bulging of at least 12 mm into either atria during different phases of the cardio-respiratory cycle.
The pathogenesis of atrial septal aneurysm might be explained by an abnormal structure of the interatrial septum, by a change in the normal inter-atrial pressure gradient, or by both. 9 Atrial septal aneurysm may also result from bulging of the septum primum tissue through the fossa ovalis. 5
ASA is mostly a benign entity. The septal bulge can be static or dynamic. It could swing into the LA, RA, and back to the LA or vice versa.
A variety of patterns of sac motion have been revealed in the literature.10,11 Atrial septal aneurysm motion was determined according to the classification introduced by Olivares-Reyes and colleagues. 4 The aneurysm is classified as type 1 right (R) if the bulging is in the RA only, type 2 left (L) if the bulging is in the LA only, type 3 RL if the major excursion bulges to the RA and the lesser excursion bulges toward the LA, type 4 LR if the maximal excursion of the atrial septal aneurysm is toward the LA with a lesser excursion toward the RA, type 5 if the atrial septal aneurysm movement is bidirectional and equidistant to both atria during the cardiorespiratory cycle. We categorized our patient to have type 5 ASA.
The association of ASA and mitral valve prolapse (MVP) suggests that a myxomatous degeneration might be responsible for both abnormalities. 12 Our patient had a myxomatous anterior mitral valve leaflet; however, definite prolapse was not detected. Inability to obtain consent for a TEE makes it impossible for us to confidently exclude MVP. Other authors have observed that a developmental abnormality affecting the tissue of the interatrial septum and mitral valve can be supposed.13,14 Atrial septal aneurysm is frequently associated with other atrial septal defects (ASDs), in particular ASD-ostium secundum type, and patent foramen ovale (PFO). 15 If it occurs in isolation it usually does not result in any shunting. These defects were not demonstrable in this study but we acknowledge the limitations of the trans-thoracic echocardiography (TTE) in detecting a small PFO or ASD as opposed to a TEE, which could not be completed due to lack of consent. TEE has been shown to be more sensitive than TTE in detecting ASAs. 3 Associations between ASAs and atrial fibrillation has been documented, 16 but our patient did not present with palpitations and we did not document any arrhythmia on the resting electrocardiography. ASA has been documented to act as an arrhythmic focus, generating focal atrial tachycardia. It also tends to aggravate stasis of LA blood flow and predispose individuals to minute LA clots and systemic thromboembolisms. Our patient did not have history of TIAs or other evidence of thromboembolic phenomena.
Some authors have observed that an ASA aneurysm may mimic a right atrial cyst or tumor. 17
Our patient was commenced on anti-platelet therapy without any anticoagulation. This is in keeping with the findings of Homma and colleagues, 18 who showed that when anticoagulation therapy (warfarin) was compared with aspirin in patients with ASA and PFO, no significant differences were noted in regard with the appearance of thromboembolic events. The most appropriate treatment therapy for asymptomatic patients with no significant associated cardiac lesions who are amenable to surgery is uncertain. Until more is known about the natural history of this lesion, all management decisions are probably best made on an individual basis.
Conclusion
ASA mimicking a cor triatriatum remains a rare clinical condition that is usually asymptomatic, but may occasionally present with unresolved atypical chest pain. In the investigation of unresolved chest pain, two-dimensional echocardiographic scanning should be performed from multiple windows, and multiple images should be acquired from conventional and modified views before any echocardiographic diagnosis is made. In addition, associated lesions such as MVP are not uncommon in ASA and a TEE remains an invaluable modality of investigation for accurate evaluation; however, this should not be a limiting factor to diagnosis especially when consent is not given or in a resource-poor setting.
Author Contributions
AOT was involved in the conception of the report, the literature review, and manuscript preparation and editing. OO was involved in the clinical care of the patient. MUS was involved in manuscript drafting, editing, review and submission. All authors proof-read, reviewed and approved of the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.