
Abstract
Cor triatriatum sinister (CTS) is a rare congenital cardiac malformation. In CTS, a fibromuscular membrane subdivides the left atrium into 2 chambers. The communication between the 2 chambers is through 1 or more orifices in the dividing membrane. We present an interesting case of a 2-month-old infant with obstructed CTS membrane who first presented on account of poor feeding and failure to thrive. Echocardiography showed a persistent levoatrial cardinal vein (LACV) connecting the left atrium and the innominate vein. This allowed the proximal left atrial chamber to decompress its blood volume into the innominate vein and subsequently the superior vena cava. There was minimal prograde blood flow across the Cor triatriatum membrane, so the majority of pulmonary venous blood ultimately returned to the heart by way of the decompressing vertical vein into the systemic venous circulation. Surgical repair was performed with an uneventful postoperative course. The specific anatomical variant of Cor triatriatum found in our subject has rarely been reported.
Keywords
Background
Cor triatriatum sinister (CTS), also known as left cor triatriatum (LCT), is a rare congenital cardiac malformation. It accounts for 0.1% of all congenital cardiac malformations. 1 It was first described by Church in 1868. 2 In CTS, the left atrium (LA) is subdivided into 2 chambers by a fibromuscular membrane. The proximal chamber is where the pulmonary veins typically return. The distal chamber is the true left atrial cavity. The communication, if present, between the 2 chambers is through 1 or more orifices in the dividing membrane.3-5 Patients with CTS might present early on in infancy and childhood or stay asymptomatic until adulthood. This varies based on the morphology of the malformation and the presence of other associated cardiac malformations.6,7 Here, we report a case of unusual association of obstructed CTS membrane with persistent levoatrial cardinal vein (LACV) and we include a discussion and short comparison with other similar reported cases.
Case Report
A 9-week-old former full-term male infant was referred to our cardiology service by his pediatrician for failure to thrive, poor feeding, and a heart murmur. His oxygen saturation was 97% in room air while resting. However, the patient would desaturate when feeding or crying. Pulse was 142 bpm. Blood pressure was 89/71. His weight was 4.22 kg (<5th %tile). On physical examination, he was pale and small for his age. The patient had evidence of mild respiratory distress with a respiratory rate in the 40s and occasional grunting respirations. Distress was more pronounced when agitated. On cardiac examination, a grade 2/6 low-pitched continuous murmur at the right upper sternal border and a 2/6 systolic ejection murmur at the right sternal border were appreciated. Abdomen was soft with a palpable liver edge. Laboratory evaluation revealed normal electrolytes. Renal function was normal with blood urea nitrogen (BUN) 16 mg/dL and creatinine 0.17 mg/dL. The alanine aminotransferase (ALT) was mildly elevated at 44 U/L. Venous blood gas was unremarkable, with pH of 7.37 and pCO2 of 44 mm Hg. Chest radiograph showed mild cardiomegaly with a prominent mediastinum and symmetrical pulmonary vascular congestion.
An echocardiogram was performed, which demonstrated LCT with a tiny jet of prograde flow across the CTS membrane from the proximal to distal LA chambers (Figures 1 and 2). There was a decompressing LACV draining to a dilated innominate vein (Figures 3 and 4). Gradient across the membrane fenestration was 10 to 12 mm Hg by echocardiography. There was mild right atrial enlargement and mild tricuspid regurgitation. Right ventricular pressure was elevated based on tricuspid regurgitation gradient, estimated at 92% of systemic pressure. Left ventricular systolic function was normal. The right ventricle was dilated but maintained normal systolic function (see Figures 1 and 2).

Schematic diagram. (Reproduced with permission from Tutschek et al. 8 Copyright John Wiley and Sons.)
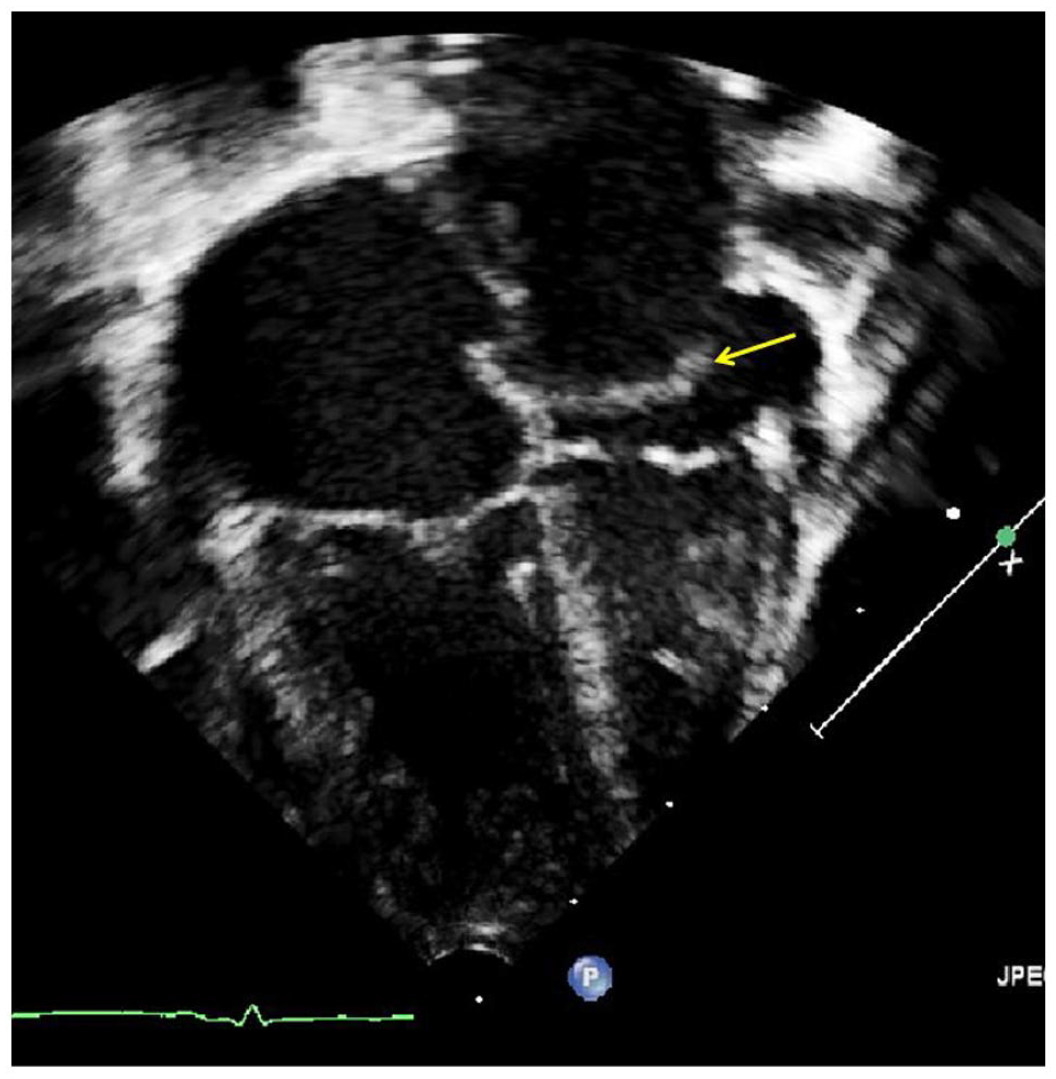
Apical 4-chamber echocardiographic view showing cor triatriatum membrane (yellow arrow) in the left atrium.
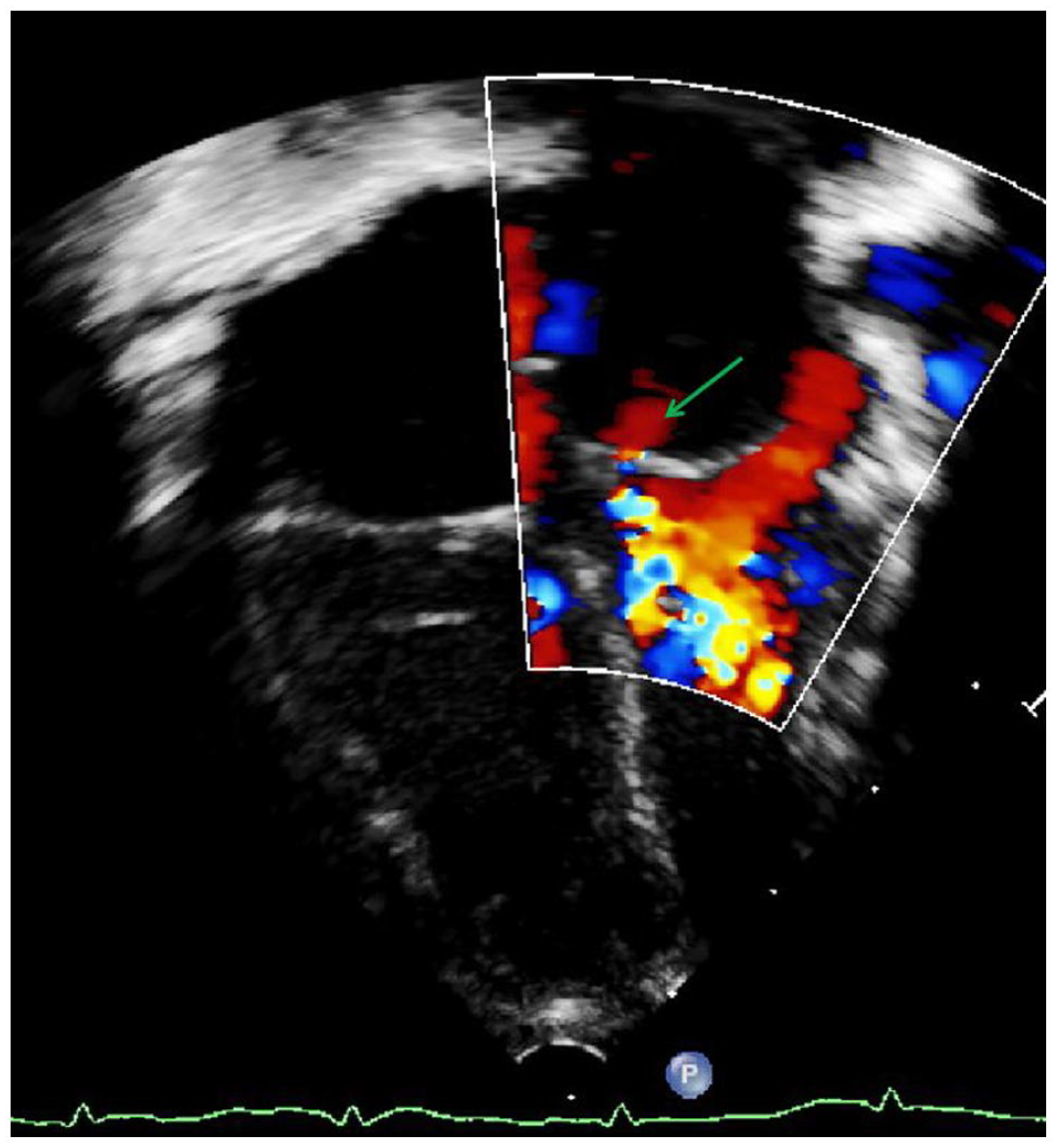
Apical 4-chamber view with color Doppler, showing severely restricted flow across the cor triatriatum membrane (green arrow).

Large decompressing levoatrial cardinal vein (green arrows) arising from left atrium (labeled LA) and draining to the innominate vein superiorly (not shown).
The patient was initially admitted to the pediatric intensive care unit and then transferred to a surgical center for repair. He underwent successful resection of a very thick cor membrane, ligation of the decompressing LAC vein, and closure of atrial septal defect. A patent ductus arteriosus was identified during the procedure and was also ligated. The patient tolerated the surgery well, with an uneventful postoperative course. He was discharged home in good condition on postoperative day 12.
Discussion
Patients with CTS differ in clinical presentation based on the size of the connection between both left atrial chambers. The inflow obstruction produced by the membrane can be severe, and lead to early symptoms of heart failure, cardiogenic shock, and death.9,10 Classically, CTS mimics the presentation of mitral valve stenosis due to restriction of left atrial flow to the left ventricle. This in turn restricts pulmonary venous flow and causes pulmonary vascular congestion. Development of symptoms and timing of presentation of cor triatriatum are also dependent upon the presence of associated congenital cardiac malformations. Cor triatriatum sinister has been reported to be associated with many congenital cardiac malformations. 6 Common associations include atrial septal defect (including patent foramen ovale), anomalous pulmonary venous drainage, and patent ductus arteriosus.11-13 If the cor membrane obstructs flow significantly, then an atrial-level communication is the means to provide adequate filling for the left ventricle (through right-to-left flow into the distal LA chamber). This was the scenario for our patient.
The association of CTS with LACV has been reported in cases presented in older ages, including adults. 14 The LACV is an embryologic connection, which may persist in the setting of high left atrial pressures. This allows for egress of blood from the LA.8,15 The presence of the decompressing vein (LACV) can delay presentation of the disease. In our patient’s case, the pulmonary veins returned normally to the LA (proximal chamber), and then the majority of pulmonary venous blood flow drained through the decompressing vertical vein into the innominate vein and ultimately back to the right atrium by way of the superior vena cava. In this manner, our patient’s lesion was physiologically identical to that of supracardiac total anomalous pulmonary venous return.
Conclusion
Cor triatriatum is an extremely rare congenital abnormality usually diagnosed in childhood. These cases have a high risk of life-threatening complications if missed in childhood. Early complications might include failure to thrive as seen in the discussed case. Some other long-term complications may include cardioembolic disease, cerebrovascular events, and arrythmias. This case highlights the need for a high index of suspicion in pediatric cases where usual modalities of treatment have failed. Patients diagnosed with this pathology require close monitoring and, in most instances, surgical intervention.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed Consent
Verbal informed consent was obtained from the guardian for their anonymized information to be published in this article.
Prior Presentation of Abstract Statement
Abstract has been accepted to be presented at the American College of Cardiology National Conference to be held at New Orleans, Louisiana, USA on March 4-6, 2023.