
Abstract
Objectives
Hemoptysis is an alarming symptom of underlying lung disease. Clinicians are often unsure how to deal with and follow up patients who have had a single episode of hemoptysis, especially if the cause remains unknown despite thorough examination, because a second, more severe episode of hemoptysis might occur despite an apparently stable condition. Investigations were done, using multivariate analyses, to see whether several clinical factors present during an initial episode of hemoptysis could be used to predict a second episode.
Subjects and Methods
Eighty patients with an initial episode of hemoptysis who underwent both computed tomographic and bronchoscopic examinations from 2003 through 2005 were reviewed.
Results
The isolation of bacteria from bronchial lavage fluid (odds ratio 13.5, P = 0.001) and the failure to determine the cause of the initial episode of hemoptysis (odds ratio 7.0, P = 0.014) were significant independent predictors of a second episode of hemoptysis. Subset analysis showed that isolation of either Pseudomonas aeruginosa or Haemophilus influenzae increased the likelihood of a second episode of hemoptysis (P = 0.077), even if colonization, representing host-bacterial equilibrium, had occurred. Furthermore, the failure to determine the etiology of an initial episode of hemoptysis was associated with an increased risk of a massive second episode (P = 0.042), regardless of the volume of the initial episode.
Conclusions
In patients with bacterial colonization of the respiratory tract or an initial episode of hemoptysis of unknown etiology, there is an increased possibility of a second episode of hemoptysis.
Introduction
Hemoptysis is an alarming symptom of underlying lung disease. Problems in treating hemoptysis include the large number of possible causes and variations in the reported prevalence. 1 11 Another problem is the possibility of a second episode of hemoptysis after the initial active bleeding has been stopped with cause-specific treatment. Unfortunately, a second episode of hemoptysis may be severe despite the initial episode being an apparently isolated production of slightly blood streaked sputum.12,13 Therefore, clinicians are often unsure on how to deal with and follow up patients who have had a single episode of hemoptysis, especially if the cause remains unknown despite thorough examinations, including computed tomography (CT) and bronchoscopy. However, most published studies of hemoptysis deal with a wide range of possible causes with various rates of prevalence, diagnostic procedures, and methods of evaluating treatment.
In the present study, investigations were done using multivariate analyses, to see whether any of the several clinical factors present during an initial episode of hemoptysis are useful predictors of a second episode of hemoptysis.
Subjects and Methods
Medical records of patients presenting with an initial episode of hemoptysis at the university hospital were reviewed. Eighty consecutive patients who had undergone both chest CT and bronchoscopic examinations from January 2003 through December 2005 were evaluated. In this institution, high-resolution CT scans are routinely performed if a conventional CT scan suggests an abnormality. Furthermore, bronchial lavage for culture of micro-organisms, polymerase chain reaction of mycobacterium, and cytologic examinations are performed in association with bronchoscopic examinations. Endobronchial or transbronchial biopsy was performed in relevant cases. Chest angiography was indicated in a limited number of cases of severe hemoptysis requiring embolotherapy. Patients with bleeding from the upper airway were excluded from this study. The institutional review board of this hospital did not require its approval or patient informed consent for a retrospective study of case records.
The cause of hemoptysis was determined on the basis of all available clinical data, chest CT, and bronchoscopic findings. The isolation of bacteria from the bronchial lavage fluid, accompanied by respiratory signs and symptoms (increased sputum production or cough, fever, chest CT findings consistent with a new pulmonary process, or changes in chest sounds), was considered as infection, whereas a state in which host defenses limited the activity of bacteria and therefore such respiratory signs and symptoms were absent was considered as colonization (host-bacterial equilibrium). 14 Bronchitis was diagnosed when respiratory signs and symptoms consistent with the upper airway infection were present and when bleeding was absent on bronchoscopic examination. 8 Bronchiectasis was diagnosed when dilated distal airways larger than the accompanying pulmonary arteries were visualized on high-resolution CT images. Abnormalities were noted on chest CT images by consultant radiologists; abnormalities found on high-resolution CT images included focal bronchial abnormalities (wall thickening, bronchiectasis, and interruption), infiltration, cavitation, scattered acinar nodules, and hilar masses. Cases of hemoptysis for which a cause could not be determined were considered to be of unknown etiology, even if bacterial colonization was observed.
The patient data collected included age, sex, smoking history, blood pressure, history of anticoagulant therapy, chest CT findings, type of bacteria isolated with bronchial lavage, etiology, time to recurrent hemoptysis, amounts of initial and recurrent hemoptysis, and treatment (Table 1). Hemoptysis was defined as recurrent when a second episode of hemoptysis had occurred after the initial episode had resolved spontaneously or with treatment. On the basis of the amount of active bleeding, cases were divided into three groups: trivial (blood-streaked sputum), moderate (<500 mL/24 hours), and massive (≥500 mL/24 hours). 8 Conservative treatment was attempted first in all patients when appropriate. Follow-up information of all the patients was updated in May 2007.
Patients’ characteristics for the prediction of recurrent hemoptysis.

Multivariate logistic regression analysis.
The relationships between categorical variables were assessed with Fisher's exact probability test or the Chi-square test as appropriate. The difference in mean between groups was evaluated with the Mann-Whitney U-test. Multivariate logistic regression analysis was performed to identify significantly independent risk factors for the second episode of hemoptysis. All calculations were performed with Stat View 5.0 J software (SAS Institute Inc., Cary, NC). Statistical significance was indicated by P values less than 0.05.
Results
The characteristics of the 80 patients are shown in Table 1. Active and inactive bacteria were isolated from bronchial lavage fluid in 13 (16%) cases. Despite further examination, no diagnosis was established in 21 (26%) cases. The initial treatment was conservative in 77 (96%) cases of trivial or moderate hemoptysis and embolotherapy was done in 3 (4%) cases of massive hemoptysis. During the follow-up period of 6.5 ∓ 9.5 months (mean ∓ standard deviation; range, 0.5-36.8 months), hemoptysis recurred in 21 (26%) cases. Multivariate logistic regression analysis showed that, of the 10 clinical factors examined (Table 1), isolation of bacteria from bronchial lavage fluid (odds ratio 13.5, P = 0.001) and an initial episode of hemoptysis of unknown etiology (odds ratio 7.0, P = 0.014) were significant independent risk factors for recurrent hemoptysis.
The most common causes of the initial episode of hemoptysis (Table 2) were, in descending order, bronchitis (22 cases, 27%), “unknown etiology” (21 cases, 26%), bronchiectasis (15 cases, 19%), and infection (pneumonia, abscess, aspergilloma, and tuberculosis: 11 cases, 14%). Other causes were primary squamous cell lung cancer (3 cases, 4%), hemorrhagic diathesis (3 cases, 4%), bronchial vascular abnormality (2 cases, 3%), bronchial atresia (1 case, 1%), pulmonary sequestration (1 case, 1%), and tracheal ulcer (1 case, 1%). The diagnosis of bronchial vascular abnormality was established in two cases when angiography and subsequent embolotherapy were performed in three patients with an initial episode of massive hemoptysis. The percentages of etiologies did not differ significantly between recurrent cases of hemoptysis with those who presented with only one episode.
Etiology of initial hemoptysis.
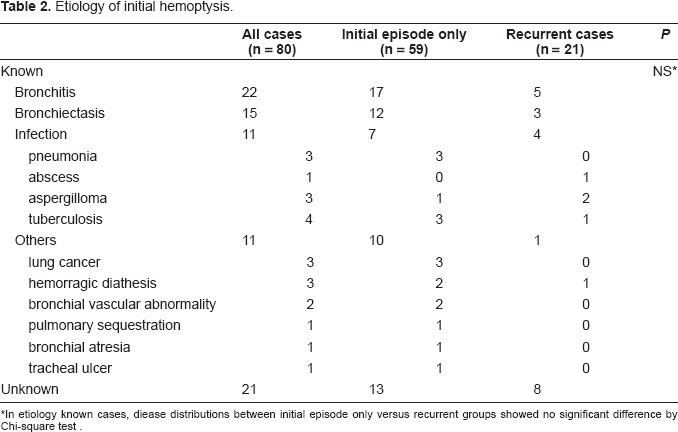
In etiology known cases, diease distributions between initial episode only versus recurrent groups showed no significant difference by Chi-square test
Fifteen species of bacteria were isolated from bronchial lavage fluid in 13 (16%) cases (Table 3). Patients with recurrent hemoptysis were more likely to have P. aeruginosa or H. influenzae in bronchial lavage fluid than were patients with a single episode of hemoptysis (Fisher's exact probability test, P = 0.077). Recurrent hemoptysis was attributed to one case each of bronchitis and lung abscess where bacterial infection was present, and to one case each of bronchiectasis and to tuberculosis, to aspergillosis in two cases, and to an unknown cause in two cases when bacterial colonization was present.
Bacteria isolated from bronchial lavage fluid.
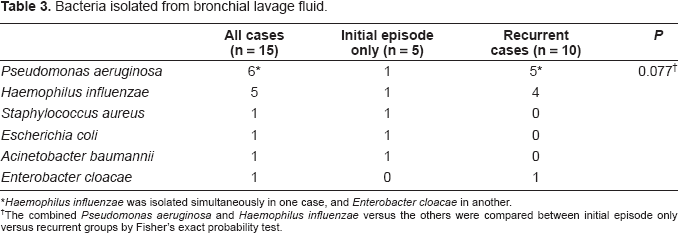
Haemophilus influenzae was isolated simultaneously in one case, and Enterobacter cloacae in another.
The combined Pseudomonas aeruginosa and Haemophilus influenzae versus the others were compared between initial episode only versus recurrent groups by Fisher's exact probability test.
Details of the second episode of hemoptysis are shown in Table 4. In these 21 cases, the mean time to recurrence was 3.9 ∓ 8.3 months (range, 0.5-36.6 months). Although massive bleeding did not occur during the first episode in these cases, massive bleeding requiring embolotherapy occurred with the second episode in three cases of unknown etiology. When each variable was compared between cases of recurrent hemoptysis of known and unknown etiology, neither time to recurrence nor the amount of initial bleeding differed significantly (Mann-Whitney's U-test and Fisher's exact probability test, respectively). However, massive bleeding in the second episode of hemoptysis and subsequent embolotherapy were significantly more common when the etiology was unknown (Fisher's exact probability test, P = 0.042 and P = 0.042, respectively). The final diagnoses after the second episode were squamous cell lung cancer arising from a segmental bronchus in one case and bronchial vascular abnormality in two cases.
Details of the second episode of hemoptysis according to initial etiology.
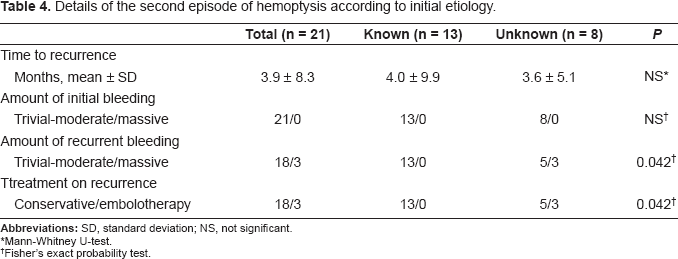
Mann-Whitney U-test.
Fisher's exact probability test.
Discussion
The present study with multivariate analysis has demonstrated that isolation of bacteria from bronchial lavage fluid and an initial episode of hemoptysis of unknown etiology are independent predictors of a second episode of hemoptysis. Furthermore, subset analysis has shown that isolation of either P. aeruginosa or H. influenzae from bronchial lavage fluid tends to increase the risk of recurrent hemoptysis, even in cases of colonization. In addition, episodes of hemoptysis of unknown etiology, regardless of the amount of bleeding, were more likely to recur as massive bleeding. The results of this analysis are credible because the series included patients with a single episode of hemoptysis who were followed-up for an average of 6.5 months at a single institution.
Previous studies have shown that the most common causes of hemoptysis are lung cancer, bron-chiectasis, bronchitis, and infection.1,2 However, the frequencies of these causes vary with the characteristics of the patient population, the geographic location, and the date of study. A review by Fidan et al. of nine series which included 1297 cases of hemoptysis has shown that the mean rates of these common causes are as follows: lung cancer 25% (range, 3%-48%); bronchiectasis 15% (range, 1%-29%); bronchitis, 15% (range, 5%-37%); pneumonia,10% (range, 1%-16%); tuberculosis, 7% (range, 1%-18%); unknown etiology, 11% (range, 1%-25%); and other causes 17% (range, 2%-28%). 10 In this study, the rate of lung cancer was extremely low (4%) and was similar to that (3%) reported by Souders and Smith, 3 whereas the rate of unknown etiology was extremely high (26%) and was similar to that (25%) reported by Abal et al. 9 This result might be explained, in part, by the inclusion in this study, only of those patients with a single episode of hemoptysis and being concerned with the etiology of only this episode. In contrast, previous studies have included as high as 40% of patients with recurrent hemoptysis and have based their analyses on final diagnoses.9,10–12 Furthermore, in three cases in the present study, hemoptysis was diagnosed as being of unknown etiology after the initial episode, but was found to be due to squamous cell lung cancer or bronchial vascular abnormality after recurrence. Herth et al. have also reported that lung cancer was later found to be present in 6% of patients with an initial episode of hemoptysis of unknown etiology. 15 Therefore, a relatively high rate of cases with unknown etiology, despite thorough investigation without routine angiography, is quite plausible.
Among cases in which the etiology could be determined, no significant differences were seen in the frequencies of diagnosed causes between patients with only one episode of hemoptysis and those with recurrent hemoptysis (Table 2); in contrast, Fidan et al. have found that recurrent hemoptysis occurred at a significantly higher rate only in patients with bronchiectasis. 10 In contrast, in this study, an initial episode of unknown etiology was an independent predictor of recurrent hemoptysis. The validity of this finding is supported by the following reasons. If the etiology is determined at the initial episode of hemoptysis, appropriate treatment would be given. However, if the cause is not established at the initial episode, appropriate treatment would not be given and a second episode might be inevitable as the underlying disease progresses; for example, occult lung cancer and potential vascular abnormality might not be diagnosed and treated without cause-specific modalities.
The second independent predictor for recurrent hemoptysis is the presence of bacteria in the bronchial lavage fluid during the first episode of hemoptysis. Bacteria were present at this initial phase in 8 of the 21 cases with recurrent hemoptysis. Bacteria could not be isolated again in all recurrent cases during a second episode of hemoptysis because bronchoscopy for bronchial lavage was not always available for all patients with recurrent hemoptysis. The aim of this study was to investigate whether, the several clinical factors present during the initial episode of hemoptysis are useful predictors of a second episode of hemoptysis.
Fifteen species of bacteria were isolated from bronchial lavage fluid. However, in most cases colonization by either H. influenzae or P. aeruginosa was only found. The bacteria that most often colonize the diseased lung are H. influenzae (22%) in chronic bronchitis, 16 H. influenzae (22%) and P. aeruginosa (16%) in bronchiectasis, 17 S. aureus (18%) and P. aeruginosa (15%) in tuberculosis, 18 and H. influenzae (35%), Streptococcus pneumoniae (13%), and P. aeruginosa (9%) in lung cancer. 19 Therefore, colonizing H. influenzae and P. aeruginosa were the bacteria most frequently isolated in this study; however, the numbers of positive cultures of bacteria other than H. influenzae and P. aeruginosa were too small to draw definite conclusions about the relative likelihood of recurrent hemoptysis on the basis of species of bacteria (Table 3, P = 0.077).
With regard to the relationship between bacterial colonization and bronchial inflammatory response, Angrill et al. have demonstrated through studies of patients with clinically stable bronchiectasis that the active neutrophilic bronchial inflammatory response is enhanced by bacterial colonization in a bacterial load-dependent manner but is apparently compartmentalized and cannot be accurately detected with hematologic studies. 17 Moreover, Wilson et al. reviewed previous studies of H. influenzae and P. aeruginosa and found that colonization readily progresses to infection if host defenses are impaired. 20 Furthermore, Chan et al. have shown that lung permeability is increased by bacterial colonization of the respiratory tract. 21 Therefore, in patients with underlying respiratory disease, the enhanced bronchial inflammatory response to bacterial colonization or infection can cause hemoptysis. In fact, Shirai et al. and Faulkner et al. have reported that superimposed bacterial colonization or infection usually accompanies episodes of hemoptysis in patients with tuberculosis and pulmonary aspergilloma, respectively.18,22 These findings suggest that treating bacterial colonization or infection might reduce the odds ratio for the development of the second episode of hemoptysis. This possibility is consistent with the conclusion of Angrill et al. 17
In this study, the mean time to recurrence was approximately four months in patients with recurrent hemoptysis regardless of etiology. Similarly, Ayed has reported that hemoptysis recurs within six months. 12 However, it is amazing that lung emboli (up to 26% have hemoptysis) and heart and vascular diseases of any type did never cause hemoptysis within the three year observation period. This might be due to the high number of unknown causes. In two patients in whom the etiology of the initial episode was unknown but later turned out to be bronchial vascular abnormality, the time to recurrence was 2.7 months and 4.3 months.
In these patients with recurrent hemoptysis, none had had a previous episode of massive hemoptysis as Ayed has reported that most initial episodes of hemoptysis are mild. 12 Furthermore, massive bleeding during the second episode of hemoptysis was significantly more common in patients in whom the etiology of the initial episode, was unknown regardless of the amount of bleeding,. No known previous study has determined the causes of an initial episode of hemoptysis that are most often associated with a massive second episode of hemoptysis; however, massive initial episodes of hemoptysis were most often caused by bronchiectasis and tuberculosis, and 10% were of unknown etiology.12,23 In this study, patients with a massive second episode of hemoptysis following an initial episode of unknown etiology, final diagnoses were lung cancer in one patient and bronchial vascular abnormality in two patients. These conditions can be life threatening through both progression and massive bleeding. 23 Therefore, if the etiology of hemoptysis remains unknown after bronchiectasis and infection have been ruled out, the possibility of occult lung cancer or vascular malformation might be considered.
Finally, to date, the prediction of recurrent hemoptysis has also been addressed by several other authors. 24 26 Jeong et al. have reported the CT findings to predict recurrent hemoptysis in 58 patients who underwent bronchial artery embolization due to massive hemoptysis. By multivariate analysis, the total number of dilated bronchial and nonbronchial systemic arteries was a significant CT variable associated with the recurrence of hemoptysis. Ozgul et al. have reported the clinical findings to predict recurrent hemoptysis in 203 patients with hemoptysis. By univariate analysis, hemoptysis lasting more than five days was a significant predictive factor for a second episode of hemoptysis. However, multi-variate analysis indicated no positive risk factors. Instead, lung cancer was shown to be a negative risk factor. Furthermore, Serasli et al. have reported the observational results, in terms of etiology, for recurrent hemoptysis in 20 patients who underwent bronchial artery embolization due to massive hemoptysis. In patients with bronchiectasis, aspergillomas, tuberculosis, malignancy, and cystic fibrosis, the relapse was due to aspergillomas, lung cancer and tuberculosis. The originality of this report, is based mainly on the method of examining clinical factors and the bacterial colonization with multivariate analysis. Therefore, it is believed that this report will be useful as well, when clinicians deal with and follow-up patients who have had an initial episode of hemoptysis.
In conclusion, there is evidence that isolation of bacteria from bronchial lavage fluid and an initial episode of hemoptysis of unknown etiology are independent risk factors for a second episode of hemoptysis. However, the relatively small number and retrospective nature of the study might limit the conclusions and require further clinical studies.
Conflict of Interest
All authors of this study, declare that there is no financial or personal relationships with other people or organizations that could inappropriately influence (bias) this work.