
Abstract
Objective
To explore the diagnostic value of liquid-based cytology (LBC) of bronchoalveolar lavage fluid (BALF) combined with bronchial brushing (BB).
Methods
One hundred patients with pulmonary masses or nodules found by chest computed tomography (CT) or X-ray before bronchoscopy or other diagnostic biopsy examinations were selected consecutively for this retrospective study. BALF and BB were performed for all patients. After conventional smear via BB, we mixed the BALF and BB samples in a prepared thin-layer bottle.
Results
The sensitivity of LBC of BALF combined with BB was noticeably higher than that of BB alone in the total sample group (65.15% vs. 32.84%, respectively). Similarly, in both the bronchoscopically visible group and invisible group, a higher sensitivity for LBC of BALF with BB vs BB alone (68.89% vs. 39.13%, respectively; 57.14% vs. 19.05%, respectively) was observed. Additionally, the negative predictive value of LBC of BALF with BB was higher than that with BB alone (58.56% vs. 42.31%; 61.29% vs. 44.73%; 53.47% vs. 37.83%; total sample vs visible vs invisible groups, respectively).
Conclusion
Regardless of whether lesions or nodules are bronchoscopically visible or invisible, LBC of BALF combined with BB may increase the diagnostic value over BB alone in lung cancer diagnosis.
Keywords
Introduction
Bronchoscopy is the most commonly used method in the diagnosis of lung cancer. 1 Cytological and histological methods for diagnosing lung cancer are routinely used during bronchoalveolar lavage (BAL) and bronchial brushing (BB) because these procedures are minimally invasive and easy to use.2,3 Liquid-based cytology (LBC) is a technique that avoids poor cellular preservation caused by smear thickness, overlap, mucolytic substances, blood, and inflammatory cells. Therefore, LBC has been used to increase the diagnostic value of respiratory material, including bronchoalveolar lavage fluid (BALF) and BB. 4 There have been several studies of the diagnostic yield of LBC in BALF and BB.5–9 These studies showed that BALF and BB cytology are valuable tools for lung cancer diagnosis, 3 and LBC of BALF has higher diagnostic accuracy than that of a conventional direct smear. 5 For other respiratory materials, including BB, LBC can be a replacement for a conventional smear. 7 However, these methods will not work if samples and cells are scanty or sample concentration is not optimal. Our study group has proven that LBC of BALF combined with BB can increase the diagnostic value over BALF alone. 10 To increase the number of specimens for increasing the diagnostic value over BB alone, in the current study, we used the same method as in our previous study of mixing BB and BALF samples in an LBC-prepared bottle after completing the specimen sampling. To our knowledge, this method has not been reported previously. In summary, in this study, we compared the diagnostic value of LBC of BALF combined with BB to that of a BB smear alone.
Materials and methods
Patients and specimens
In this retrospective study, with verbal consent from the patients or their caregivers, 100 patients with pulmonary masses or nodules found by chest computed tomography (CT) or X-rays before bronchoscopy or other diagnostic biopsy examinations were consecutively enrolled from May 2015 to May 2016 in the Department of Respiratory and Critical Care Medicine of Ningbo First Hospital. The bronchoscopically visible group was defined as a mass or nodule that can be seen under bronchoscopy, and the invisible group was defined as a nonvisible mass or nodule. The patient’s information and clinical characteristics were derived from their medical records and the hospital’s registries. The diagnoses of the patients’ lesions were confirmed via histological samples obtained via bronchoscopy, surgery, or percutaneous lung biopsy. This study was performed in accordance with the National Comprehensive Cancer Network Clinical Practice Guidelines in Oncology for Lung Cancer. 1 Approval for this study was obtained from the Ningbo First Hospital Ethics Committee (No. 2021RS009). All patients’ details have been de-identified. The reporting of this study conforms to the STROBE guidelines. 11
BALF and BB
These procedures have been described in our previous studies.10,12,13 First, a straight brush (BC-202D-2010; Olympus, Tokyo, Japan) for BB was used for smearing the slides. Then, we put the brush into a BD CytoRich™ Red preservative (Cytyc Corporation, Boxborough, MA, USA) bottle. Finally, a BALF sample in 0.9% saline was added to fill the bottle.
Statistical analysis
Clinical data, namely age, smoking years, and body mass index, were presented as mean ± standard deviation (SD). Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated to evaluate the diagnostic value in the total sample group, visible group, and invisible group. The statistical analyses were performed using GraphPad Prism 5.0 (GraphPad Software Inc., San Diego, CA, USA).
Results
Patient characteristics
Data for 100 patients (77 men and 23 women; age: 63.13 ± 8.88 years) were analyzed in this study, and the clinical characteristics of these patients are summarized in Table 1. Using cytological and histological information, 67 patients were diagnosed with malignant lesions (29 squamous cell carcinomas, 25 adenocarcinomas, 8 small-cell lung cancers, and 5 other types of cancer), and 33 patients were diagnosed with benign lesions.
Clinical characteristics of the recruited participants.

SD, standard deviation; BMI, body mass index.
Diagnostic value of BALF combined with BB vs BB alone
Using the final cytology and histology pathology results, the sensitivity, specificity, PPV, and NPV were calculated, and the results are presented in Table 2, Table 3, and Table 4. Table 2 shows that the sensitivity of LBC of BALF with BB was obviously higher than that with BB alone in the total sample group (65.15% vs. 32.84%, respectively). Similarly, in the visible group and invisible group, Table 3 and Table 4 show a higher sensitivity of LBC of BALF with BB than that with BB alone (68.89% vs. 39.13%; 57.14 vs. 19.05%, respectively). Regardless of whether the lesions were visible or invisible, and compared with the total group, the NPV of LBC of BALF with BB was higher than that with BB alone (BALF with BB vs BB alone, respectively: 58.56% vs. 42.31%; 61.29% vs. 44.73%; 53.47% vs. 37.83% for total vs visible vs invisible groups, respectively). The specificity and PPV for LBC of BALF with BB were both 100% for all groups.
Diagnostic value of bronchoalveolar lavage fluid (BALF) with bronchial brushing vs. bronchial brushing alone.

PPV, positive predictive value; NPV, negative predictive value.
Diagnostic value of bronchoalveolar lavage fluid (BALF) with bronchial brushing vs. bronchial brushing alone in visible lesions.
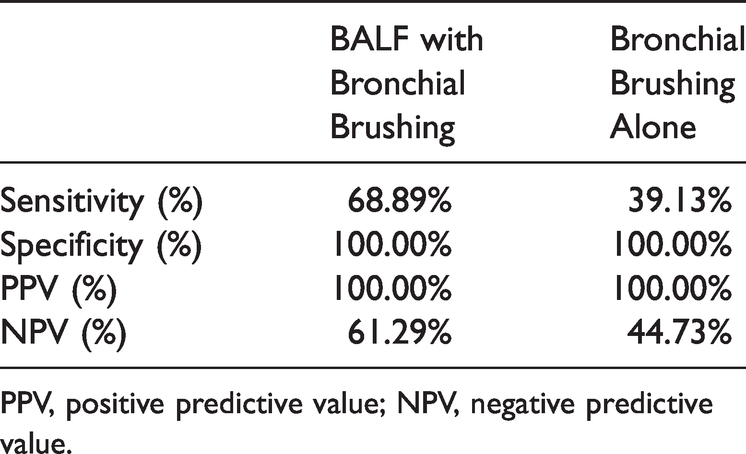
PPV, positive predictive value; NPV, negative predictive value.
Diagnostic value of bronchoalveolar lavage fluid (BALF) with brush vs. brush alone in invisible lesions.

PPV, positive predictive value; NPV, negative predictive value.
Discussion
Cytological and histological methods are used with BAL and BB in patients with lung cancer. LBC is used routinely in BALF or BB because LBC helps remove exudates that contain mucus, blood, and inflammatory cells, 14 as shown in previous studies.4,5,7,9 Although samples are easily obtained with BALF or BB, and the procedures are minimally invasive, the diagnostic value of these methods for cancer is low.3,15 In previous studies, the sensitivity of BALF for the diagnosis of lung cancer ranged from 29% to 57.3%,16–19 and the sensitivity of diagnosis was higher for lesions visible under bronchoscopy. The diagnostic yield of BB varies widely between studies, with a range of 18% to 87%. 20 Our study group previously mixed BALF and BB samples in a thin-layer prepared bottle to increase the diagnostic yield of BALF and BB. The results were published in a paper that demonstrated that the diagnostic value of LBC of BALF combined with BB was higher than that with BALF alone. 10 Therefore, we used the same method to compare the value of LBC of BALF with BB with that of BB alone, in this study. We concluded that LBC of BALF combined with BB may increase the diagnostic value of BB alone, regardless of whether the lesion is visible or invisible.
The main advantage of LBC is that cells spread in a thin layer without obscuring elements or resulting in cell overlap.21,22 This characteristic helps improve the diagnostic yield of the cytological and histological samples. LBC of BALF has been confirmed to provide higher diagnostic accuracy than that with conventional direct smears of samples obtained with BB alone. 5 LBC combined with BB has been used routinely for samples obtained via bronchoscopy, and LBC can be considered a replacement for a conventional smear.4,7 Similarly, our results confirmed that LBC of BALF combined with BB can improve the diagnostic value over BB alone.
Previous studies have shown that the diagnostic yield of BALF is similar to the yield with BB when lesions are bronchoscopically invisible.23–25 However, data from our results revealed that LBC of BALF combined with BB may improve the diagnostic yield for both visible and invisible lesions. BB increased the cell yield if BAL failed to wash or recycle enough fluid. Furthermore, the thin layer of LBC maintains the cell morphology and removes interfering elements. Therefore, considering the results of our previous 10 and current studies, we conclude that LBC of BALF combined with BB improves the diagnostic value over BB or BALF alone.
The following limitation should be considered: BALF and BB with or without LBC are unsuitable for patient screening compared with using samples for gene detection. Deficient target cytological or histological samples is the main disadvantage in BALF with BB; therefore, in patients requiring further diagnostics or treatments, physicians should choose other biopsy procedures or methods.
Conclusion
Regardless of whether lesions or nodules are bronchoscopically visible or invisible, LBC of BALF combined with BB specimens may increase the diagnostic value over BB alone in lung cancer. Considering the results of our previous and current studies, LBC of BALF combined with BB may be a replacement for BALF or BB alone.
Research Data
Research Data for The usefulness of liquid-based cytology of bronchoalveolar lavage fluid combined with bronchial brush specimens in lung cancer diagnosis
Research Data for The usefulness of liquid-based cytology of bronchoalveolar lavage fluid combined with bronchial brush specimens in lung cancer diagnosis by Shanni Ma, Xuechan Yu, Xiaoyan Jin, Feng Qiu, Xueqin Chen, Ran Wang and Chao Cao in Journal of International Medical Research
Footnotes
Data availability statement
All data used in this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The Authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.