Two common methods have been used to evaluate the in vitro bioactivity of bioceramics for the application of bone repair. One is to evaluate the ability of apatite formation by soaking ceramics in simulated body fluids (SBF); the other method is to evaluate the effect of ceramics on osteogenic differentiation using cell experiments. Both methods have their own drawbacks in evaluating the in vitro bioactivity of bioceramics. In this commentary paper we review the application of both methods in bioactivity of bioceramics and conclude that (i) SBF method is an efficient method to investigate the in vitro bioactivity of silicate-based bioceramics, (ii) cellular bioactivity of bioceramics should be investigated by evaluating their stimulatory ability using standard bioceramics as controls; and (iii) the combination of these two methods to evaluate the in vitro bioactivity of bioceramics can improve the screening efficiency for the selection of bioactive ceramics for bone regeneration.
The bioactivity of ceramics has been defined as “the bond ability with host bone tissue”.1 This includes enhancing the ability of apatite formation, osteoblast differentiation and bone matrix formation. Current bioceramics, such as hydroxyapatite, β-tricalcium phosphate (β-TCP), HAp/β-TCP and bioglass 45S5® have been widely used as bone repair materials, mainly due to their excellent bioactivity which makes them capable of bonding closely with the host bone tissue. The main disadvantage of these bioceramics is their relatively low mechanical strength, particularly low fracture toughness, which limits their application to only low-load bearing areas in the human body. To develop new bioactive ceramics for load bearing bone repair applications, it is important to understand the bonding of ceramics to living bone and methods to test bonding abilities.2 In order to avoid the high cost of in vivo experiment, several in vitro tests have been used to predict the in vivo bone bioactivity of bioceramics. However, there is still challenging to evaluate the in vitro bioactivity of bioceramics. Currently, two common methods have been used for testing the in vitro bioactivity of bioceramics. One method is to evaluate the apatite-formation ability of bioceramics in the simulated body fluids (SBF).2–4 The other method is to investigate in vitro bone cell response to bioceramics.5–7 To evaluate apatite formation, Kokubo and colleagues have established a method to examine the apatite formation on materials in SBF. This method is useful prior to doing in vivo bone bioactivity experiments and can significantly reduce the number of animals needed for in vivo evaluation.2 However, Bohner and colleagues recently published a study which showed that there is currently not enough scientific evidence to support Kokubo's claims that SBF is a useful tool to evaluate the in vitro bioactivity, and that the choice of SBF solution for testing the in vitro bioactivity of bioceramics is quite arbitrary.8 As for the cell experiment method, a large part of the scientific community has accepted the paradigm that in vitro cell testing can be used to test the in vitro bioactivity of bioceramics. This method has been widely used in testing the bioactivity of bioceramics. However, there are a number of cases indicating that using cell experiments to evaluate the in vitro bioactivity of bioceramics are not sufficient.9–12 The methods for evaluating the in vitro bioactivity of bioceramics are still not clear. Therefore, the aim of this commentary paper is to present our view of how best to evaluate in vitro bioactivity of bioceramics.
Comments for the In Vitro Bioactivity of Bioceramics
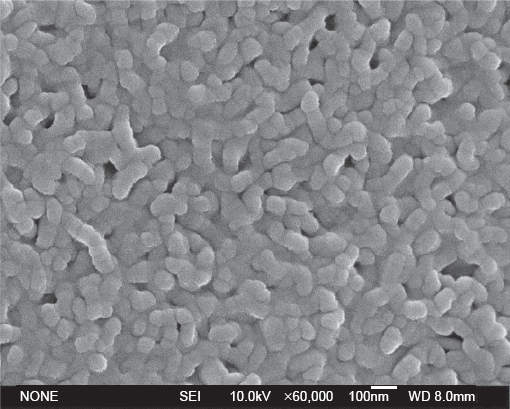
Firstly, the SBF method is a useful way to test the in vitro bioactivity of bioceramics for the assessment of the apatite formation potential. However, the reliability this method depends on the category of bioceramics tested. Silicate-based bioceramics, including silicate bioglass 45S5@,1 wollastonite (CaSiO3),4,13 akermanite (Ca2MgSi2O7) (See Fig. 1)3 and diopside (Ca2MgSi2O6)14 ceramics, have been shown to have excellent apatite forming abilities in SBF. Other studies also showed that these silicate ceramics possess good in vivo bioactivity,15–18 which indicates that SBF testing is an efficient method to evaluate their in vitro bioactivity. Phosphate-based bioceramics (HAp and β-TCP),19–21 carbonate-based bioceramics (coral, CaCO3), and sulfate-based materials (CaSO4), have no obvious apatite formation when soaked in SBF for a short time. They do, however, have excellent in vivo bone formation abilities,22,23 but this suggests that SBF alone is not sufficient to test the in vitro bioactivity for these three bioceramics. The SBF method, therefore, is useful for evaluating the in vitro bioactivity of silicate ceramics, but not for other types of bioceramics. The possible reason for this is that the biochemistry of in vivo bone formation of these bioceramics is significantly different. Silicate-based bioceramics bond with host bone via the formation of bone-like apatite layers due to the dissolution Ca2+ or other metal ions, followed by the deposition of Ca-P in the body1,17,24,25 The phenomenon of dissolution and deposition does in fact happen in the SBF solution for silicate-based bioceramics. Sintered HAp and β-TCP ceramics can also bond directly with host bone.15,21,26 Their apatite-formation ability mainly depends on their crystanillity and sintering property. Fully sintered HAp bulk ceramics are difficult to induce bone-apatite formation,19,20 and sintered β-TCP ceramics exhibit a poor ability of inducing apatite formation;27 however, HAp particles can induce apatite formation.28 CaCO3 and CaSO4 materials bond to living bone, which may be related to their high resorbability.2
Apatite formation on akermanite ceramics after soaking in SBF 10 days.
Secondly, cell experiments have been used widely to investigate the in vitro bioactivity of bioceramics. It is known that Al2O3, ZrO2, TiO2, and Mg2SiO4 bioceramics have been considered as bioinert ceramics since they cannot induce apatite formation in SBF. They do, however, support bone cell attachment, proliferation and differentiation.9–12,29,30 There are therefore a number of ceramics which elicits excellent cell responses; however, this does not necessarily translate into good in vivo bioactivity. On the contrary, some ceramics, such as highly degradable CaSiO3 ceramics, are detrimental to the in vitro growth of human osteoblasts due to their high rate of dissolution which results in a high localized pH environment.7,31,32 On the other hand, recent studies have shown that CaSiO3 ceramics possess excellent in vivo bone-formation ability and their in vivo bioactivity is greater than that of β-TCP.17 Cell based experiments to evaluate in vitro bioactivity of bioceramics are therefore not completely reliable. In addition, if cell cultures are used to evaluate the in vitro bioactivity of bioceramics, one should also investigate if the same bioceramics have the ability to stimulate or enhance a cell response. The selection of positive control materials to compare the cellular response is therefore important. Previous studies have selected β-TCP ceramics as the control material to compare the osteoblast response to akermanite (CaMSiO) bioceramics.6,33 It is necessary to know that the standard β-TCP ceramics has been carefully prepared by a standardized method and procedure, since the β-TCP ceramics can be prepared by a number of methods and these will affect different cell responses. Other studies have used blank tissue culture plate as control and to show that the ionic products of bioglass,5 akermanite,3 Sr-CaSiO313 and hardystonite (Ca2ZnSi2O7)34 ceramics stimulate osteoblast proliferation. Tissue culture plate can therefore be regarded as one of the standard controls to evaluate in vitro bioactivity of bioceramics.
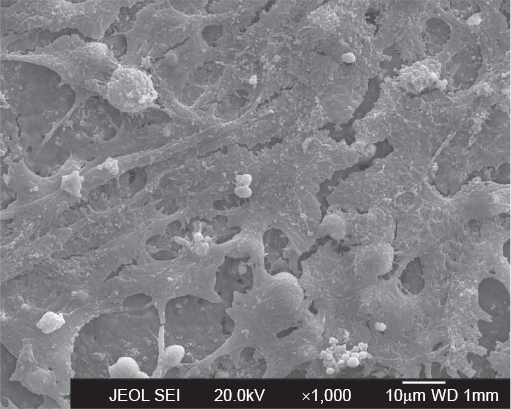
Thirdly, combining SBF and cell experiments to evaluate the in vitro bioactivity of bioceramics may be the better option. This is because if a novel bioceramic not only has the ability to induce apatite deposition in SBF, but also stimulates a cell response, such a bioceramic would most likely possess excellent in vivo bioactivity as well. Our own work has shown that akermanite ceramics has excellent apatite-forming abilities in SBF3 and significantly enhances in vitro osteoblast attachment (See Fig. 2), proliferation, differentiation and gene express compared to β-TCP ceramics,6 and in vivo experiments have confirmed that they also have excellent bone-forming abilities in animal tests.16 Another example is 45S5 bioglass, which possesses good apatite-formation ability35 and supports osteoblast attachment, furthermore, the ionic products released from 45S5 bioglass stimulate osteoblast proliferation, differentiation, mineralization and osteogenic gene expression.5,36–38 The in vivo experiment has also shown that 45S5 bioglass has excellent bone bond ability to be used as a bone repair material.1,15,39
Osteoblast-like cells growing on the surface of akermnaite ceramics after 7 days of culture.
Conclusions
Selection of methods for the evaluation of in vitro bioactivity of bioceramics depends on the composition of bioceramics and the mechanism of their bone formation. The synthetic body fluid method is a useful approach to evaluate the in vitro bioactivity of silicate-based bioceramics. Cell based experiments is also a valuable test for bioactivity of bioceramics, but relevant standard materials should be considered as positive control. We recommend the combination of SBF and cell testing methods to evaluate the in vitro bioactivity of bioceramics, an approach which will improve the efficiency of screening bioceramics for further in vivo evaluation of bone repair.
Footnotes
Acknowledgements
The authors would like to acknowledge the Queensland University of Technology Vice-chancellor's Research Fellowship 241402-0120/07 (Dr. Wu) for funding our research relative to this commentary paper. We would also like to thank Mr. Thor Friis for proofreading of the manuscript.
The authors report no conflicts of interest.
References
1.
HenchL.L.Bioceramics: from concept to clinic.J Am Ceram Soc.1991; 74: 1487–510.
2.
KokuboT., TakadamaH.How useful is SBF in predicting in vivo bone bioactivity?Biomaterials.2006; 27(15): 2907–15.
3.
WuC., ChangJ., NiS., WangJ.In vitro bioactivity of akermanite ceramics.J Biomed Mater Res A.2006; 76(1): 73–80.
4.
LiuX., DingC., ChuP.K.Mechanism of apatite formation on wollastonite coatings in simulated body fluids.Biomaterials.2004; 25(10): 1755–61.
5.
ValerioP., PereiraM.M., GoesA.M., LeiteM.F.The effect of ionic products from bioactive glass dissolution on osteoblast proliferation and collagen production.Biomaterials.2004; 25(15): 2941–8.
6.
SunH., WuC., DaiK., ChangJ., TangT.Proliferation and osteoblastic differentiation of human bone marrow-derived stromal cells on akermanite-bioactive ceramics.Biomaterials.2006; 27(33): 5651–7.
7.
WuC., RamaswamyY., SoepartoA., ZreiqatH.Incorporation of titanium into calcium silicate improved their chemical stability and biological properties.J Biomed Mater Res A.2008; 86(2): 402–10.
8.
BohnerM., LemaitreJ.Can bioactivity be tested in vitro with SBF solution?Biomaterials.2009; 30(12): 2175–9.
9.
WebsterT.J., SiegelR.W., BiziosR.Osteoblast adhesion on nanophase ceramics.Biomaterials.1999; 20(13): 1221–7.
10.
ManiconeP.F., Rossi IommettiP., RaffaelliL.An overview of zirconia ceramics: basic properties and clinical applications.J Dent.2007; 35(11): 819–26.
11.
ManiconeP.F., Rossi IommettiP., RaffaelliL., PaolantonioM., RossiG., BerardiD.Biological considerations on the use of zirconia for dental devices.Int J Immunopathol Pharmacol.2007; 20(12 Suppl 1): 9–12.
12.
PopatK.C., ChatvanichkulK.I., BarnesG.L., LatempaT.J.Jr, GrimesC.A., DesaiT.A.Osteogenic differentiation of marrow stromal cells cultured on nanoporous alumina surfaces.J Biomed Mater Res A.2007; 80(4): 955–64.
13.
WuC., RamaswamyY., KwikD., ZreiqatH.The effect of strontium incorporation into CaSiO3 ceramics on their physical and biological properties.Biomaterials.2007; 28(21): 3171–81.
14.
IwataN.Y., LeeG.H., TokuokaY., KawashimaN.Sintering behavior and apatite formation of diopside prepared by coprecipitation process.Colloids Surf B Biointerfaces.2004; 34(4): 239–45.
15.
HenchL.L.Biomaterials: a forecast for the future.Biomaterials.1998; 19(16): 1419–23.
16.
HuangY., JinX., ZhangX., SunH., TuJ., TangT.In vitro and in vivo evaluation of akermanite bioceramics for bone regeneration.Biomaterials.2009.
17.
XuS., LinK., WangZ., ChangJ., WangL., LuJ.Reconstruction of calvarial defect of rabbits using porous calcium silicate bioactive ceramics.Biomaterials.2008; 29(17): 2588–96.
18.
NonamiT., TsutsumiS.Study of diopside ceramics for biomaterials.J Mater Sci Mater Med.1999; 10(8): 475–9.
19.
RamilaA., PadilaS., MunozB., Vallet-RegiM.A new hydroxyapatite/glass biphasic material: In vitro bioactivity.Chem Mater.2002; 14: 2439–43.
20.
BalasF., Perez-ParienteJ., Vallet-RegiM.In vitro bioactivity of silicon-substituted hydroxyapatites.J Biomed Mater Res A.2003; 66(2): 364–75.
21.
OhtsukiC., KokuboT., NeoM., KotaniS., YamamuroT N.T.Bone-bonding mechanism of sintered 3CaO-P2O5.Phos Res Bull.1991; 1: 191–6.
22.
CuiL., LiuB., LiuG., ZhangW., CenL., SunJ.Repair of cranial bone defects with adipose derived stem cells and coral scaffold in a canine model.Biomaterials.2007; 28(36): 5477–86.
23.
MacNeillS.R., CobbC.M., RapleyJ.W., GlarosA.G., SpencerP.In vivo comparison of synthetic osseous graft materials. A preliminary study.J Clin Periodontol.1999; 26(4): 239–45.
24.
XueW., LiuX., ZhengX., DingC.In vivo evaluation of plasma-sprayed wollastonite coating.Biomaterials.2005; 26(17): 3455–60.
25.
MiakeY., YanagisawaT., YajimaY., NomaH., YasuiN., NonamiT.High-resolution and analytical electron microscopic studies of new crystals induced by a bioactive ceramic (diopside).J Dent Res.1995; 74(11): 1756–63.
26.
KotaniS., FujitaY., KitsugiT., NakamuraT., YamamuroT., OhtsukiC.Bone bonding mechanism of beta-tricalcium phosphate.J Biomed Mater Res.1991; 25(10): 1303–15.
27.
KimH.M., HimenoT., KawashitaM., KokuboT., NakamuraT.The mechanism of biomineralization of bone-like apatite on synthetic hydroxyapatite: an in vitro assessment.J R Soc Interface.2004; 1: 17–22.
28.
XinR., LengY., ChenJ., ZhangQ.A comparative study of calcium phosphate formation on bioceramics in vitro and in vivo.Biomaterials.2005; 26: 6477–86.
29.
MendoncaG., MendoncaD.B., SimoesL.G., AraujoA.L., LeiteE.R., DuarteW.R.Nanostructured alumina-coated implant surface: effect on osteoblast-related gene expression and bone-to-implant contact in vivo.Int J Oral Maxillofac Implants.2009; 24(2): 205–15.
30.
NiS.Y., ChouL., ChangJ.Preparation and characterization of forsterite (Mg2SiO4) bioceramics.Ceram Int.2007; 33(1): 83–8.
31.
RamaswamyY., WuC., Van HummelA., CombesV., GrauG., ZreiqatH.The responses of osteoblasts, osteoclasts and endothelial cells to zirconium modified calcium-silicate-based ceramic.Biomaterials.2008; 29(33): 4392–402.
32.
WuC., RamaswamyY., BoughtonP., ZreiqatH.Improvement of mechanical and biological properties of porous CaSiO3 scaffolds by poly(D,L-lactic acid) modification.Acta Biomater.2008; 4(2): 343–53.
33.
LiuQ., CenL., YinS., ChenL., LiuG., ChangJ.A comparative study of proliferation and osteogenic differentiation of adipose-derived stem cells on akermanite and beta-TCP ceramics.Biomaterials.2008; 29(36): 4792–9.
34.
RamaswamyY., WuC., ZhouH., ZreiqatH.Biological response of human bone cells to zinc-modified Ca-Si-based ceramics.Acta Biomater.2008; 4(5): 1487–97.
GoughJ.E., JonesJ.R., HenchL.L.Nodule formation and mineralisation of human primary osteoblasts cultured on a porous bioactive glass scaffold.Biomaterials.2004; 25(11): 2039–46.
37.
GoughJ.E., NotingherI., HenchL.Osteoblast attachment and mineralized nodule formation on rough and smooth 45S5 bioactive glass monoliths.J Biomed Mater Res.2004; 68: 640–50.
38.
XynosI.D., EdgarA.J., ButteryL.D., HenchL.L., PolakJ.Gene-expression profiling of human osteoblasts following treatment with ionic products of bioglass 45S5 dissolution.2001; 55: 151–7.
39.
MartinV., ChristianV., GrossU.M., Muller-MaiC.In vivo comparison of bioactive glass particle in rabbits.Biomaterials.2001; 22: 357–62.