
Abstract
Overview
The purpose of this study was to evaluate the role of Tumor Necrosis Factor-α (TNF-α) in insulin resistance (IR) during normal pregnancy.
Approach
This cross sectional study was carried out on 86 healthy pregnant women including 26, 23 and 37 individuals in the 1st, 2nd and 3rd trimesters, respectively, and in 21 healthy non pregnant women. Serum TNF-α concentration was measured by Enzyme Linked Immunosorbent Assay (ELISA) method.
Results
There were significant differences between serum TNF-α and IL-6 levels in pregnant women as compared with maternal healthy controls. There was significant correlation between gestational age and Body Mass Index (BMI) (r = 0.28,
Conclusion
In conclusion, our findings suggest that TNF-α and IL-6 are not greatly contributed to pregnancy induced insulin resistance in normal pregnancy.
Introduction
Pregnancy is related to glucose metabolism disorders and insulin resistance.1–3 Insulin resistance may facilitate supply of appropriate nutrients particularly of glucose to the fetus for growth and metabolism. The mechanism responsible for insulin resistance has not been clearly established. Recent research shows that adipokinins including leptin 4 resistin 5 interleukin-6 (IL-6) 6 and TNF-α7–10 play an important role in insulin resistance. TNF-α is one of the most widely studied cytokinins produced by adipose tissue. This cytokinin is also secreted by placenta.11,12 TNF-α has an important role in obesity-induced insulin resistance and diabetes.7,10,13,14 A few studies suggest that TNF-α may play a role in insulin resistance in normal and diabetogenic pregnant women8,13,15 Interleukine-6 is another cytokinine produced by immune and non immune cells.16–18
There are reports regarding its role in the pathogenesis of insulin resistance.7,19–21 Insulin sensitivity changes from an enhanced state during early pregnancy to an insulin resistant state in late pregnancy.3,8,22 Therefore, it is suspected, subsequent to increase in IR during pregnancy, its related factors change too. However, at the time of our study we did not find any research had been done about changes in serum IL-6 and TNF-α levels during different trimesters of normal pregnancy and their relationships to insulin resistance. Therefore, the aim of this study is to determine the association of insulin resistance with serum interleukin-6 and TNF-α levels during normal pregnancy.
Methods
This study was conducted at the Department of Obstetrics and Gynecology of Honary Clinic, Jahrom, Iran. Subjects were 86 pregnant women with different gestational ages (first trimester: 26, second trimester: 23, third trimester: 37, and 21 non pregnant women similar in age and body mass index (BMI)). All subjects met the following criteria: no history of pregestational diabetes; no history of liver, respiratory, thyroid or other illness or any current infectious condition. They were not on any drug therapy.
Body mass index (BMI, Kg/m2) was calculated according to the maternal height and prepregnacy weight. Serum samples were analyzed for concentrations of IL-6, TNF-α, insulin and glucose. Blood sugar was measured by glucose oxidase/ peroxidase (GOD-POD) method. Serum insulin was determined by ELISA (Diaplus; based on the direct sandwich technique in which two monoclonal antibodies are directed against separate antigenic determinants on the insulin molecule. During incubation insulin in the sample reacts with enzyme (HRP) conjugated anti-insulin antibody and anti-insulin antibody bound to micro-titration well. A sample washing step removed unbound enzyme labeled antibody. In the insulin ELISA, the bound HRP complex is detected by reaction with TMB substrate. The reaction is stopped by adding acid to give a colorimetric end-point that is read using ELISA reader). Serum TNF-α was assayed by ELISA (Bendermed, Austria Ref NO: BMF 223; It is based on the direct sandwich technique with biotin-Streptavidin, in which two monoclonal antibodies are directed against human TNF-α. Human TNF- present in the sample or standard binds to antibodies adsorbed to the microwells. A biotinconjugated anti-human TNF- antibody is added and binds to human TNF- captured by the first antibody. Following incubation unbound biotin-conjugated anti-human TNF- antibody is removed during a wash step. Streptavidin-HRP is added and binds to the biotin-conjugated anti-human TNF- antibody. Following incubation unbound Streptavidin-HRP is removed during a wash step, and substrate solution reactive with HRP is added to the wells. A coloured product is formed in proportion to the amount of human TNF- present in the sample or standard. The reaction is terminated by addition of acid and absorbance is measured at 450 nm. A standard curve is prepared from 7 human TNF- standard dilutions and human TNF- sample concentration determined). Serum IL-6 was measured by ELISA (Bendermed, Austria Ref NO: BMS213HS;). Insulin resistance value were calculated using the homeostasis model assessment, HOMA- IR, as (fasting insulin IU/L) × (fasting glucose mmol/L)/22.5 as previously reported by Matthows. 23
The study was approved by the ethical committee of Jahrom University of Medical Sciences. All participants in the study filled and signed informed consent letter.
All results are displayed as mean ± SD (standard devation of mean). Insulin resistance (IR), BMI and body weight data were analyzed with One Way analysis of Variance (ANOVA). Serum IL-6, TNF-α and insulin concentration data were analyzed with non-parametric kruskal-wallis test followed by Mann Whitney U-test. Correlations were calculated using liner correlation (Pearson). Statistical analysis was performed using SPSS 11 for Windows.
Results
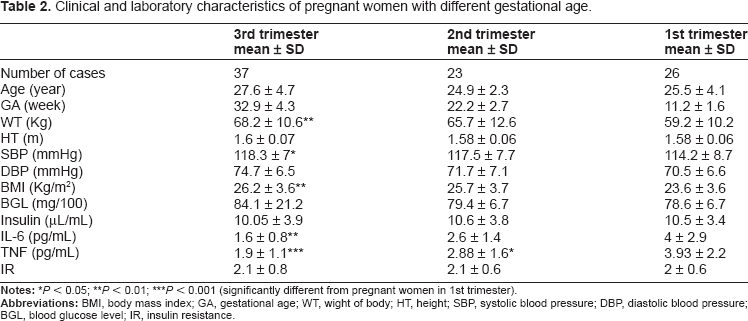
A total of 86 pregnant women and 21 non pregnant subjects participated in the study. Clinical and laboratory characteristics of subjects are summarized in Table 1. Body mass index was significantly different in the third trimester as compared with non pregnant and women with first trimester of pregnancy (Fig. 1A, Table 2). In terms of systolic pressure, subjects in the second and third trimester of pregnancy were significantly different compared to non pregnant women (Fig. 1B). There was statistical difference in serum IL-6 concentration between the non pregnant women and subjects in first, second and third trimester of pregnancy (Table 2, Fig. 1C). TNF-α level was also significantly higher in patients in all gestational age as compared to non pregnant women (Fig. 1D). However, during pregnancy TNF-α level decreased by increasing in the gestational age (Table 2). Pregnant women exhibited higher score of HOMA IR compared to non pregnant subjects group, however, there was no difference in this score between pregnant subjects in different gestational age (Tables 1 and 2). There was significant correlation between gestational age and BMI (r = 0.28,
Clinical and laboratory characteristic of subjects.


A) BMI in patients in different trimesters of pregnancy and non pregnant subjects. BMI were significantly higher in 3rd trimesters compared with the control (**
Clinical and laboratory characteristics of pregnant women with different gestational age.
Discussion
Glucose metabolism disorder is a common complication during pregnancy and its pathology is associated with IR and deficiency of insulin secretion. 2 This study showed that insulin resistance was significantly different in pregnant group in general compared to non pregnant subjects. In spite of a previous report we did not found correlation between gestational age and insulin resistance. Our finding was in contrast to the results of Kirwan et al, 8 Melczer et al 9 and Consultant et al 3 in which they showed insulin resistance was significantly increased in the late pregnancy compared with either non pregnant or early pregnancy. This difference may be due to differences in dietary composition, life style between western and eastern societies, 24 variability between insulin assays in different experimental researches, 25 differences in the population study and sampling time during pregnancy.
A number of studies have reported concentrations of IL-6 in pregnant subjects. 21 ,26–28 Our data are inconsistent with several pervious observations that found an increase in IL-6 level in pregnant compared to non-pregnant subjects. 26 IL-6 is a pro inflammatory cytokine that has important role in on-time parturition and success of pregnancy.27,29 There are limited and partially contradictory reports concerning the pattern of IL-6 secretion during normal pregnancy.26–28 In the present study, maternal serum IL-6 has decreased with further increasing in pregnancy period. In this regard, our results were in contrast with Doria et al and Curry et al.29,30 We speculate, that this discrepancy was probably caused by different biochemical assays for determination of serum IL-6, 28 and differences in survey population. 30 In addition, several other variables may influence cytokine levels during pregnancy including maternal age, prepregnancy body mass index and prior preterm delivary status. 31 In the present study, we did not find any correlation between maternal IL-6 and insulin resistance.
Our results are in agreement with several previous observations that found an increase in TNF-α level in pregnant as compared to non pregnant subjects9,15,32 but in contradiction with these studies, we found a negative correlation between gestational age and TNF-α level. Explanations accounting for this finding may be related to lifestyle of our subjects. Clapp et al reported that regular weight bearing exercise during pregnancy suppressed the usual pregnancy- associated changes in the circulating level of TNF-α. 33 In our study most of pregnant subjects lived in a rural area with a high level of physical activity. In addition, pregnancy is associated with changes of several hormones such as estrogen, progesterone, cortisol and 1,25 dihydroxyvitamin D3.34–36 Some of these hormones, for instance cortisol and catecholamines and 1,25 dihydroxy D3, are potent inhibitors of TNF -α production by monocyte/macrophage.37–40 Plasma concentration of cortisol was more elevated during late pregnancy than early pregnancy. 8 Therefore, it is possible to increase production of these hormones during pregnancy to be responsible for reducing maternal TNF-α production.
In conclusion, our findings suggest that TNF-α and IL-6 do not greatly contribute to pregnancy induced insulin resistance in normal pregnancy.
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.
Footnotes
Acknowledgements
This work was supported by the research project of the Jahrom University of Medical Sciences. Authors thank the staffs of Honary Clinic, Motahary Hospital particularly, Miss Neda Abaszade and Mr Shadman. Authors are grateful to subjects who accepted to enter this study.