
Abstract
Every year numerous individuals develop the morbid condition of sepsis. Therefore, novel biomarkers that might better inform clinicians treating such patients are sorely needed. Difficulty in identifying such markers is in part due to the complex heterogeneity of sepsis, resulting from the broad and vague definition of this state/condition based on numerous possible clinical signs and symptoms as well as an incomplete understanding of the underlying pathobiology of this complex condition. This review considers some of the attempts that have been made so far, looking at both the pro- and anti-inflammatory response to sepsis, as well as genomic analysis, as sources of potential biomarkers. Irrespective, for functional biomarker(s) of sepsis to successfully translate from the laboratory to a clinical setting, the biomarker must be target specific and sensitive as well as easy to implement/interpret, and be cost effective, such that they can be utilized routinely in patient diagnosis and treatment.
What is Sepsis?
Sepsis refers to the presence of a serious infection that correlates with systemic and uncontrolled immune activation. 1 Patients die as a result of organ failure as the disease elicits an exacerbated and damaging immune response with approximately 250,000 cases leading to fatalities in the USA annually.2,3 As of 2009, the Centers for Disease Control and Prevention listed sepsis as the 11th leading cause of death in the United States.4,5 The treatment of sepsis is also costly. The total hospital cost for patients with severe sepsis increased from $15.4 billion in 2003 to $24.3 billion in 2007. 6 While sepsis has been described for centuries, a formal definition was not established until 1992 at the Consensus Conference of the American College of Chest Physicians and the Society of Critical Care Medicine. 7 Sepsis was defined as the host's immune response (systemic inflammatory response syndrome, SIRS) to injury and/or infectious stimuli in the presence of a known (or strongly suspected) infection. This same consensus group also defined criteria to qualify SIRS, which schematized the host inflammatory response to infection, trauma, ischemia–reperfusion injury, and burns. In 2001, this same conference modified the SIRS definition by expanding the list of signs and symptoms of sepsis to reffect clinical bedside experience. 8
Traditionally, the host immune response to sepsis was thought to be characterized by two sequential stages: The first stage is an initial hyperinflammatory response, sometimes referred to as a cytokine storm, where the innate immune system releases proinflammatory cytokines to combat infection, while also recruiting members of the adaptive system to mount an intense immune response. This initial response is then thought to be followed by compensatory anti-inflammatory response syndrome (CARS), which is defined as a systemic deactivation of the immune system tasked with restoring homeostasis from an inflammatory state. 9 However, this process can be dysregulated leading to persistent immune suppression and high risk for reoccurring infections.10,11 Recent data suggest that both aspects of the proinflammatory and anti-inflammatory stages of the host immune response to severe injury and/or sepsis often occur concurrently. 10 However, while there are numerous cellular processes involved in sepsis, finding a reliable diagnostic biomarker specific for sepsis has been difficult to identify. This, in turn, has made the development of new treatments and interventions slow.
What Makes a Good Biomarker?
The National Institutes of Health defines a biomarker as a characteristic that should objectively measure and evaluate (be an indicator of) normal biological processes or pharmacological response to a therapeutic intervention. 12 Biomarkers should be measured accurately and reproducibly. This is unlike medical symptoms that are restricted to indications of health or illness through the patient's perspective. Biomarkers may be used as a diagnostic tool for the identification (diagnosis) of disease or abnormal conditions, as well as for staging disease, prognosis, and response to intervention. Owing to the broad and vague definition of sepsis along with its various manifestations and severity levels in different patient populations, a definitive biomarker that could aid in therapeutic strategies could be difficult to ascertain. More than 100 different molecules have been suggested as useful biomarkers of sepsis.13,14 The International Sepsis Forum Colloquium on Biomarkers of Sepsis was convened in 2005 to develop a systematic framework for the identification and validation of biomarkers of sepsis. 15 This report proposed that the use of biomarkers could have the potential to alter our view of sepsis, from one of a broad physiologic syndrome to a group of distinct biochemical disorders, and this would help in therapeutic decision-making and ultimately improve the prognosis for septic patients. However, it was noted that in order for biomarkers to be useful in guiding the treatment of sepsis, there needs to be better standardization of assay methodologies, clearly defined and detailed biomarker studies, wider integration of biomarkers into the clinical setting, as well as increased collaboration between investigators, pharmaceutical industry, biomarker industry, and regulatory agencies. Ultimately, a sepsis biomarker should be able to identify either the onset of SIRS or CARS before the onset of multiple organ dysfunction syndrome and aid in the lowering of mortality rates.
Current Treatments/Therapeutics for Severe Sepsis and Septic Shock
One of the most used assays in sepsis diagnosis is a positive blood culture. However, this diagnostic tool has its limitations because of the delay in the time for results and the issue that positive blood cultures are not present in a majority of cases. 16 In addition to white blood cell (WBC) counts and blood cultures, lactate testing in all patients with suspected severe sepsis has become increasingly emphasized and used to expedite aggressive early treatment as well as monitor the impact of therapy. 17 The use of serum lactate testing in patients with suspected and diagnosed sepsis has increased dramatically since 2003. However, in 2013, serial lactate testing rates remained suboptimal, and a majority of patients with severe sepsis and those with clinical markers indicating suspected septic shock did not have serum lactate levels measured. 17 As of 2012, the recommended management for severe sepsis includes care bundles put together by the Surviving Sepsis Campaign, which includes measuring lactate levels, obtaining blood cultures prior to antibiotic administration, broad-spectrum antibiotics, administration of 30 mL/kg crystalloid for hypotension or lactate >4 mm/L, and vasopressors. 18 Currently, no biological molecular markers are used in the diagnosis or prognosis of sepsis or septic shock in the United States. Here we address the identification of septic specific biomarkers and their potential in aiding in the diagnosis and development of new therapeutic targets against sepsis.
Proinflammatory Biomarkers
C-reactive protein (CRP)
CRP is a protein found in blood plasma, synthesized and released by the liver. CRP production is part of the nonspecific acute-phase response to most forms of inflammation, infection, and tissue damage. 19 Currently, CRP is used as a clinical marker to assess the presence of infection. CRP is able to differentiate between viral and bacterial infections. 20 Numerous studies have reported the high sensitivity and specificity of CRP for the diagnosis of sepsis.21–23 In ICU patients, elevated concentrations of serum CRP upon admission are correlated with an increased risk of organ failure and death. 24 However, other studies have demonstrated that CRP levels are not indicative of survival in sepsis patients.25–27
Procalcitonin (PCT)
PCT is a 116 amino-acid protein with a molecular weight of 13 kDa and is a precursor of calcitonin produced by C-cells of the thyroid gland, which is intracellularly cleaved by proteolytic enzymes into the active hormone. 28 PCT was first described for the diagnosis of sepsis in 1993. 29 Since then, it has been widely investigated as a potential biomarker for sepsis and has been used widely in Europe as a biomarker in the management of infection and sepsis. 14 In healthy individuals, serum concentrations of PCT are below 0.1 ng/mL. In response to a bacterial infection, damage-associated molecular patterns (DAMPs) and pathogen-associated molecular patterns stimulate cells to produce PCT, which results in a significant increase in serum concentrations. 30
As of 2011, 46 studies evaluating the efficacy of PCT as a biomarker in sepsis had been published. 30 PCT's value as a biomarker in the diagnosis and prognosis of sepsis is mixed, 14 the suggestion being that initial PCT levels are not reliable as a diagnostic biomarker, but that serial PCT concentrations may have value in monitoring sepsis outcomes.30,31 The concept of PCT clearance has been studied as a potential prognostic biomarker in septic patients. In this regard, studies have reported significant improvement in PCT clearance in survivors compared to nonsurvivors in both severe sepsis and septic shock patients.31–33 Therefore, suggesting that PCT clearance could be indicative of patient outcome and serial PCT readings throughout hospitalization could aid in treatment planning to provide greater chances of improving patient outcome. It has been suggested that PCT levels have the potential to differentiate between sepsis and SIRS resulting from sterile inflammation. 34 PCT-guided therapy may also reduce antibiotic exposure without increasing the mortality rate in ICU patient population. 35 A meta-analysis of seven studies comprising a total of 1,075 patients with severe sepsis or septic shock was performed to investigate the impact of a PCT-guided therapy compared to standard treatment administered to severe sepsis patients treated in an ICU. 36 This meta-analysis concluded that no treatment algorithms for guidance of severe sepsis treatment using PCT levels are well established in this patient population. Also noted was that reliable cut-off values of PCT levels to guide therapeutic decisions need to be defined, as treatment algorithms varied substantially between the studies included in the analysis. Despite the need for further investigation of PCT-guided antimicrobial therapy, recent guide lines issued by the American College of Critical Care Medicine recommended the use of PCT as an adjunctive diagnostic marker to differentiate sepsis from SIRS of a noninfectious origin. 37
Endothelial Proteins as Potential Biomarkers
Angiopoietins
In sepsis, angiopoietins have been associated with vascular leakage, inflammation, and breakdown to the microvascular endothelium. Angiopoietins (Ang-1 and Ang-2) are antagonistic factors in endothelial cell activation. While studied mainly in proliferative diseases such as cancer,38,39 they have also been associated with inflammation.39–41
Ang-1 and Ang-2 compete for a tyrosine kinase receptor Tie2 on endothelial cells. Ang-1 is constitutively released from pericytes. Ang-1/Tie2 binding induces Tie2 phosphorylation and a quiescent vascular endothelial phenotype with upregulation of prosurvival and anti-inflammatory proteins.40,42 However, activated/stimulated endothelial cells rapidly release Ang-2, which binds to Tie2 and serves to destabilize endothelial cell-cell junctions leading to decreased barrier function, tissue edema, endothelial cell apoptosis, and increased inflammation.41,43 High levels of Ang-2 released from stimulated endothelial cells are found in the blood of trauma patients and are associated with endothelial dysfunction and poor outcome.44,45
Activation of this pathway is involved in vessel integrity, vascular permeability, and inflammation.43,46 Ang-1 and Ang-2 levels have been studied as a potential prognostic biomarker in sepsis. Ricciuto et al. 44 demonstrated that low Ang-1 levels at admission were associated with poor outcome and remained a significant predictor of mortality throughout a 28-day period, while Ang-2 levels correlated with disease severity along with organ dysfunction and injury. Another study indentified elevated Ang-2 in patients with suspected infection within the first hour of hospitalization. 47 In addition, Ang-2 levels have demonstrated to differentiate between sepsis and severe sepsis with concentrations correlating also with tumor necrosis factor-α (TNF-α) and IL-6 levels (both proinflammatory markers seen in sepsis). 48 Using an in vitro sepsis model, inhibition of Ang-2 with a monoclonal antibody has been shown to attenuate injury to the microvascular endothelium, 47 while Ang-2 KO mice exhibit greater survival and less vascular inflammation. Overall, these studies conclude that Ang-1 and Ang-2 levels may be potentially useful biomarkers in patient prognosis and a valuable tool in early decision therapies.
Endocans
Another endothelial specific biomarker with potential to be predictive of sepsis severity and organ-specific failure is endothelial cell-specific molecule-1/endocan. mRNA for this sulfate proteoglycan molecule was detected in lung and to a lesser extent in kidney tissue by Lassalle et al. 49 Additional experiments in human cell lines by this group showed that expression of endocan was upregulated following stimulation with proinflammatory cytokines, TNF-α and IL-1β. 49 Additionally, studies by Béchard et al suggest that release of endocan in response to inflammatory stimulation may play a role in regulating endothelial cell/leukocyte interactions by disrupting LFA-1/ICAM–receptor interactions. 50 In a prospective observational study, Lassalle et al reported increased endocan expression in the serum of patients with sepsis. 51 Recent studies have proposed potential correlates between endocan synthesis/release into blood and the severity of sepsis and organ failure. A recent one-year prospective study by Mihajlovic et al showed increased serum endocan protein in septic patients who go on to develop multiple organ dysfunction within the first 48 hours. 52 Concurrently, another prospective observational study showed that initial low plasma endocan levels in septic patients were predictive of delayed (day 3) and increased respiratory failure severity. 53 While plasma endocan appears to correlate with severity, outcome, and/or mortality as reported in the three observational studies described above, the sample size for each of these studies was relatively small.51–53 Still, the predictive value of a biomarker associated with endothelial cell dysfunction remains highly appealing, as respiratory failure/multiple organ failure is a major clinical manifestation in sepsis.
DAMPs/Cell Surface Receptors as Potential Biomarkers
CD64
CD64, a leukocyte surface antigen, is a high affinity Fc receptor (FcγRI), which binds to monomeric IgG. The Fc receptors are involved with the innate and adaptive immune response, stimulating either phagocytosis or antibody-mediated cytotoxicity. 54 CD64 is constitutively expressed on neutrophils, but at low levels during the absence of infection. The upregulation of CD64 on the PMN cell surface is considered to be an early step in the innate immune response to bacterial infection.55,56 Several studies have looked at neutrophil CD64 expression as a potential biomarker/indicator for detection of sepsis/infection in adults, children, and neonates.56–59 CD64 index demonstrated higher sensitivity and specificity than CRP, WBC count, neutrophilic and eosinophilic granulocyte counts, or erythrocyte sedimentation rate in adults. 56 In children, CD64 shows the highest diagnostic accuracy for differentiation between bacterial sepsis and SIRS at the time of suspected sepsis. 59 However, in neonates, the highest diagnostic accuracy was not obtained until 24 hours after suspected sepsis. Overall, there is a high expression of CD64 in septic patients, while low CD64 expression was found in patients without evidence of infection,54,57,58,60 implying that CD64 index can differentiate between sepsis and SIRS patients in various patient populations.
Triggering receptor expressed on myeloid cells-1 (TREM-1)
TREM-1 is a recently discovered member of the immunoglobulin superfamily that is expressed on the cell surface of neutrophils, monocytes, and macrophages, which plays a role in the inflammatory response. 61 TREM-1 is upregulated on the cell surface of myelocytes in the presence of bacteria, but not markedly expressed in a noninfectious inflammatory response. 62 Increased upregulation of TREM-1 also results in an increased elevation in the level of soluble TREM-1 (sTREM-1). In a clinical study, plasma sTREM-1 levels higher than 60 ng/mL were found to be more accurate than any other clinical or laboratory finding for indicating infection. 63 Various studies have shown the potential of sTREM-1 in evaluating disease severity and outcome.64–66 In neonatal septic patients, sTREM-1 values were higher in both culture-positive and culture-negative samples. 66 This is valuable as sTREM-1 could be used as an indicator in neonatal sepsis, thus allowing the initiation of broad-spectrum treatment before obtaining blood culture results, or when neonates have clinical evidence of sepsis except for a positive culture result. In adult populations, sTREM-1 levels were useful in the prognosis of septic patients with a positive culture, with sTREM-1 levels being significantly higher in nonsurvivors compared to survivors, but failed to have any value in culture-negative septic patients. 67 While studies evaluating sTREM-1 as a potential biomarker are promising, sample sizes in these studies are small, and many of the studies contradict whether sTREM-1 has any clinical value.
Circulating cell-free DNA (cf-DNA)
Recently, there has been interest in the use of cf-DNA as a potential biomarker in critically ill patients. The measurement of cf-DNA has been shown to be useful for early risk stratification and prediction of in hospital and overall morbidity and mortality in a range of conditions, including stroke, myocardial infarction, cancer, and trauma. 68 Studies have found that nonsurviving patients in the ICU present higher cf-DNA concentrations than surviving patients,68,69 and maximum plasma DNA concentration measured during the first 96 hours of intensive care is associated with the degree of organ dysfunction, disease severity, and mortality. 70 However, recently Garnacho-Montero et al. 71 contradicted these findings by determining that levels of cf-DNA do not predict outcome and were not sufficient in predicting mortality. More work must be done in order to determine whether cf-DNA has any potential value as a biomarker in sepsis. This includes determining its origin, as some say it originates from DNA fragments released by apoptotic cells, 72 while others believe that cf-DNA is a result of a novel neutrophil killing assay called NETosis. 73 Only then it can be determined if cf-DNA holds any clinical value in critically ill patients.
Cytokine/Chemokine Signaling
Sepsis can be divided into two stages: a hyperinflammatory phase early in the onset of disease involving the innate immune response that is subsequently followed by a extended immunosuppressive phase that involves both innate and adaptive immune responses (Fig. 1).10,74 Cytokines are immune-modulating agents that are produced by almost all nucleated cells and are thought to mediate important aspects of the pathophysiology of SIRS. In septic patients, both proand anti-inflammatory cytokines are produced and secreted simultaneously. 75 Cytokine serum levels are raised in patients with sepsis and severe sepsis as compared to those in nonseptic patients, 76 and therefore, from a historical prospective, these were posited as some earlier molecular/serum protein-based biomarkers for the development of SIRS and sepsis.
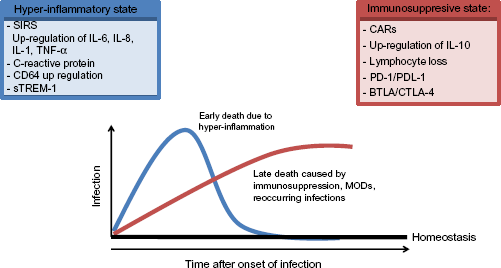
Sequential stages of Sepsis: activation of the pro and anti-inflammatory stages of the host immune response to severe injury and/or sepsis often occur concurrently. Cells of the innate immune system including monocytes and neutrophils release large amounts of pro-inflammatory cytokines leading to a “Cytokine storm”. Early death in sepsis is usually due to this hyper-inflammatory response. Over the course of the disease, there is a systemic deactivation of the immune system (CARs) which is responsible for restoring homeostasis from the inflammatory state. This leads to immune dysregulation and a state of persistent immune suppression along with a high risk for reoccurring infections. Death is generally caused by this inability to clear either initial infection or secondary infections.
Mortality from sepsis and septic shock was traditionally thought to be a consequence of an exacerbated early innate immune response, caused by an overproduction of early proinflammatory cytokines, such as TNF-α, IL-1, IL-6, and IL-8, in both adults and neonates.75,77–79 Clinical studies looking at cytokine levels at various points throughout hospital admission showed that levels of IL-6 and IL-8 are closely related to the severity and outcome of septic patients.78,79 Levels of TNF-a profiled at the time of admission and 48 hours later were higher in patients who succumbed as compared to survivors. 79 Neonatal studies have concluded that increased levels of IL-6 and IL-8 could be used as early prognosis tools to detect both early and late onset sepses.80–82 However, while proinflammatory cytokine profiles are good indicators of infection, they are also produced with sterile inflammation (SIRS), such as surgery, as well as in autoimmune disorders, viral infection, and transplant rejection,83–88 thus, reducing their specificity.
On the other side of the spectrum, there are anti-inflammatory cytokines. IL-10 is the key cytokine in anti-inflammatory responses. IL-10 is produced by CD4+ T2 cells, monocytes, and B-cells, 89 and has been proposed as the main contributor to CARS as an attempt by the immune response to control hyperinflammation. 90 Measurement of serum cytokines in patients with severe sepsis indicated that the IL-10 levels were significantly increased78,79,91 and had marked correlation to worse outcome and death. This suggested that patients who succumb to disease are severely immunosuppressed. However, here too sensitivity and specificity relative to diagnosis and/or prognosis have not been clear.
Multiplex approaches to the measurement cytokines in patient serum have made the measuring of cytokines levels relatively easy. Commercially available multiplex kits can measure as many as 31 cytokines simultaneously from 25 μL of sera, and the limits of these tests are usually because of funds, not because of lack of a kit. 92 Additionally, interpreting these many different cytokines while looking for patterns of upregulation and/or suppression in its relation to the diagnosis of sepsis or septic shock has proven to be difficult and should be interpreted with caution.
Potential Immunomodulatory Biomarkers
Lymphocyte loss
Lymphocyte cell loss results in the diminished capacity to fight and eliminate pathogens, and is the main feature of immune suppression in critically ill patients. Septic patients' inability to effectively fight and eliminate infections often leads to the development of secondary infections. Recent research has given rise to the idea that septic patients often succumb to persistent primary infection or development of secondary infections because of this impaired adaptive response. It has been reported that 63% of deaths in septic patients occur more than six days after the diagnosis of sepsis, while 37% of patients died in the acute phase of sepsis. 93 An important feature of sepsis-induced immunosuppression is apoptosis-related loss of immune cells, including CD4 and CD8 T- and B-cells. Prolonged lymphopenia is a potential marker of persistent immunosuppression in septic patients, and absolute lymphocyte counts are easy to measure during routine care. Low absolute lymphocyte counts are predictive of postoperative sepsis and are a better predictor of bacteremia than conventional infection markers, such as CRP and WBC measurements, in the emergency care unit. 94 A clinical study looking at lymphopenia as a potential biomarker concluded that persistent lymphopenia was associated with increased development of secondary infection and that persistent lymphopenia on the day 4 following the diagnosis of sepsis predicts early and late mortalities and thus may serve as a biomarker for sepsis-induced immunosuppression. 95
Concurrently, dentritic cells, which are a group of antigen-presenting cells (APCs) that interact with T- and B-cells, display increased susceptibility to sepsis-induced apoptosis that leads to further B- and T-cell impairment. 96 Septic shock patients display a significant and prolonged depletion of circulating dendritic cells (DCs), which has been correlated to severity of disease, development of ICU-acquired infections, and increased mortality.97,98 Therefore, it has been suggested that DC depletion plays a role in septic shock and may be useful as a potential biomarker of septic shock severity.
Tregs
Regulatory T-cells (Tregs) are a lymphocyte sub-population that plays an important role in preventing autoimmunity. 99 Tregs function primarily at the site of inflammation where they modulate the immune reaction through three major mechanisms: direct killing of cytotoxic cells, inhibition of cytokine production by cytotoxic cells, and direct secretion of immunomodulatory cytokines, such as TGF-β and IL-10. 99 Natural Tregs are classified as CD4+CD25+ Tregs, which are derived from the thymus and have been extensively studied. 100 The use of CD4+CD25+ Tregs in peripheral blood as a potential biomarker has been evaluated in aiding in the prognosis of septic patients. 101 In septic patients, CD4+CD25+ Treg cell counts were increased in circulation and have been associated with poor outcome, with the median ratio of CD4+CD25+ Tregs in peripheral blood being significantly higher in nonsurvivors compared to survivors.101,102 Thus, CD4+CD25+ Treg cells may offer a possible biomarker to be able to accurately assess prognosis of sepsis patients.
CD39 has been demonstrated to be a useful marker for CD4+CD25+ Tregs with CD39+ Tregs having been reported to be a more powerful subset of Tregs in suppressing the immune response and playing a key role in the pathogenesis of some inflammatory diseases through the generation of adenosine.103,104 Huang et al. 105 demonstrated that circulating levels of CD39+ Tregs increased significantly in septic patients compared with SIRS patients and healthy control subjects. In addition, there was a significant positive correlation between CD39+ Treg expression and the sequential organ failure assessment (SOFA) score, concluding that increased expression of CD39+ Tregs was associated with a poor prognosis for sepsis patients.
A multicohort analysis of sepsis gene expression data sets attempting to define genes that distinguish patients with sepsis from patients with sterile inflammation showed that the 11-gene set of interest displayed an upregulation in Tregs and a decrease in DCs, 106 thus, implicating Tregs as a potential driving force in differential gene expression between sterile SIRS and sepsis. Overall, these data indicate that Tregs may be a potential target in identifying sepsis immunosuppression and aid the therapy decisions to combating the dysfunctional immune response in sepsis.
PD-1/PDL-1 pathway
Programed cell death receptor (PD-1) is a negative co-inhibitory molecule that is expressed on lymphocytes, myeloid, and DCs. PD-1's main ligand, PD-L1, is expressed by epithelial cells, endothelial cells, and APCs. 107 PD-1/PD-L1 binding results in the tyrosine phosphorylation of the PD-1 internal immunoreceptor tyrosine-based inhibitory motif (ITIM) or immunoreceptor tyrosine-based switch motif (ITSM) domain. This leads to recruitment of phosphatases such as Src homology region 2 domain-containing phosphatase (SHP)-1/SHP-2 and results in an inhibitory signal for T-cells. The PD-1/PD-L1 pathway has been implicated as an important modulator of host immune responses in regulation of autoimmunity, tumor immunity, transplantation immunity, allergy, immune privilege, and ischemia/reperfusion injury. 108
Experimental models of sepsis have shown that the PD-1/PD-L1 pathway plays a pathologic role in altering microbial clearance. In a mouse CLP model, PD-1–/– mice were protected from the lethality of sepsis, along with a decreased bacterial burden and had a suppressed inflammatory response. More specifically, macrophages were shown to express higher levels of PD-1 during sepsis, and elevated expression was associated with macrophage dysfunction. 109 Additionally, PD-L1 was also shown to have a role in the immune response to septic insult. High expression of PD-L1 was found on neutrophils and was associated with worse outcome/reduced survival from sepsis in an experimental sepsis model, which was correlated to elevated circulating inflammatory cytokine levels. 110 It has been well documented that proinflammatory cytokines as well as the immunosuppressive cytokines are higher in those patients who succumb.79,111 Thus, it is suggested that an increased frequency of PD-L1 expression might be used as an indicator to predict lethal outcome of sepsis.
In a clinical setting, septic shock patients displayed an increase in PD-1 and PD-L1 CD4+ T-lymphocyte expressions at days 1–2 and 3–5 after the onset of shock in comparison with patients with trauma and healthy volunteers. 112 These increased PD-1-related molecule expressions on monocytes were significantly associated with increased mortality and higher risk of developing secondary nosocomial infections after septic shock. In addition, increases were also associated with immune dysfunction, including decreased mitogen-induced lymphocyte proliferation and increased circulating IL-10 concentrations. Another cohort study of 19 patients also demonstrated that PD-1 on T-cells and PD-L1 on monocytes are upregulated dramatically in septic shock patients and exhibited accelerated apoptosis of all major lymphocyte subpopulations as compared with healthy controls. 113 These data suggest that the PD-1/PD-L1 pathway might be a useful target in identifying sepsis-induced immunosuppression.
B- and T-lymphocyte attenuator (BTLA) and cytotoxic T-lymphocyte antigen-4 (CTLA-4)
BTLA and its ligand herpesvirus-entry mediator are expressed by a wide range of cells, including B-cells and T-cells, and are known to negatively regulate T-cell responses. 114 Recent research has suggested that T-lymphocyte dysfunction may contribute to sepsis-associated morbidity and mortality. BTLA is a recently characterized co-inhibitory receptor that is known to inhibit CD4+ T-cell and B-cell functions as well as reduce prosurvival signaling in CD4+ T-cells.115,116 In ICU patients with sepsis, the percentage of peripheral blood BTLA+/CD4+ lymphocytes was significantly higher compared with critically ill nonseptic individuals and was associated with a subsequent secondary infection. 117 Furthermore, BTLA expression on innate populations has been demonstrated to enhance susceptibility to septic morbidity and mortality in mice. 118 CTLA-4, which when bound to CD80 or CD86, is another inhibitory regulator of early stages of T-cell activation and proliferation. 119 CTLA-4 has been shown to be an important inhibitor of immune cell function and is increased in patients with sepsis. 120 Additionally, antibodies to CTLA-4 improved survival in two different models of fungal sepsis as well as prevented lymphocyte apoptosis and immunosuppression in a murine CLP model.120,121 This makes BTLA as well as CTLA-4 potential biomarkers of sepsis-induced immunosuppression. However, bigger clinical studies are needed to determine whether BTLA expression can serve as a useful biomarker to identify critically ill patients who are at risk of developing infection. In addition, while in vivo modeling has shown the importance of CTLA-4 in immune suppression, in-depth clinical studies are needed to understand its importance in human sepsis and its potential use as a biomarker of septic immune suppression.
Potential Genomic Regulators of Sepsis
In addition to identifying measurable biological markers in the diagnosis and prognosis for septic patients, current research has focused on using high throughput technologies to better identify the pathophysiology of sepsis as well as aid in the treatment of patients. A popular approach has been to study gene expression in patients. Genome-wide expression analysis offers the advantage of surveying the entire transcriptome of a cell or tissue and evaluating changes in expression without any preexisting bias. In an attempt to find a genomic profile for injury/sepsis, the National Institute of General Medical Sciences funded the Inflammation and Host Response to Injury Large-Scale Collaborative Research Program, also known as the Glue Grant (GG). The genomics core of this collaborative goal was to evaluate global changes in whole blood leukocyte gene expression based on the Affymetrix GeneChip technology in order to identify patterns of gene expression that result from severe injury and are associated with different clinical trajectories. Data showed that severe blunt trauma produced significant changes in the leukocyte messenger RNA abundance of 16,820 out of 20,720 Entrez genes on the microarrays, which represents more than 80% of the human genome over the first 28 days. The term genomic storm was created to describe the magnitude and speed with which the leukocyte transcriptome reorganized and reprioritized its expression patterns. 122 Using existing microarray data from the Inflammation and the Host Response to Injury GG collaborative research program, Cuenca et al. 123 were able to develop novel rapid turn-around multiplex array that can be performed from blood sampling within a 12–18-hour time frame and integrated into a single score that can predict long term, allowing clinicians to identify patients who will be at risk for developing adverse clinical outcomes and permitting them to focus care on prevention of complications, such as secondary infections and multisystem organ failure. Recently, a study used a multicohort analysis of the publicly available sepsis gene expression data sets to define a set of genes for distinguishing patients with sepsis from patients with sterile inflammation. From these data, 11 genes were identified that robustly distinguish sterile inflammation from infectious inflammation. These 11 genes then have the potential to distinguish patients with sepsis from patients with SIRS. 106 In comparing the genome-wide expression signatures of children with SIRS, sepsis, or septic shock, common gene patterns were seen across all the three groups on day 1. 124 Gene expression patterns began to diverge across the three groups with the most notable divergence occurring in the patients with septic shock. These patients demonstrated upregulated signaling pathways related to innate immunity and inflammation through day 3, unlike patients in the other two groups. As these genomic data sets become more readily available, some considerations must be addressed. Mostly, these studies used relatively small patient populations that fit into strict inclusion criteria. It is currently unknown if there is gene expression variability in distinct patient populations. There is also the limitation of analysis. Similarly, as like with cytokine profiling patterns of up-regulation and/or suppression in its relation to the diagnosis of sepsis, gene expression analysis could prove difficult because of the immense size of potential gene data sets. As genomic profiling techniques and assays improve, subsequent data will help further elucidate the complex pathophysiology of sepsis, leading to better diagnostic tools to recognize sepsis vs. SIRS in patients as well as better therapeutic targets.

Biomarkers and Patient Populations
Sepsis is a complex process with a high degree of variability. Immune responses to sepsis cannot be counted on to be the same from patient to patient. Making the challenge more complicated is the incidence and response to septic insult is different between patient populations, as well as observed disparities among races and between men and women. 3 Currently, there is a lack in capacity to delineate distinct populations of patients with a discrete disease, which is a crucial prerequisite to enable the development of specific biologically rational therapies. 125 Better patient age definitions that clarify specific age groups of patients, ie, neonates, pediatrics, adult, and geriatrics, are needed to better gage biological molecular marker trends and determine what biomarkers are significant and possibly useful in diagnosing/treating sepsis in each patient population.
Future of Biomarkers
Thus far, the use of biomarkers has been focused on the diagnosis of sepsis, the ability to differentiate between infectious and noninfectious processes, and to some degree, monitor the response to the treatment in patients with sepsis. Owing to the complex pathophysiology of sepsis, success will be better attained by not just looking at one particular biomarker but more likely a combination of readouts reflecting the various aspects of the host response. Many clinical studies are already looking at combination of readouts in relation to proinflammatory and anti-inflammatory responses, as well as their relation to Acute Physiology and Chronic Health Evaluation and SOFA scores, as an aid in the diagnosing and treating of sepsis.14,20,27,57,71,77,94,117 The combination of several biomarkers may help overcome the limitations of sensitivity and specificity that single biomarker readouts have routinely shown.
The current definition of sepsis/SIRS is vague at best comprising of numerous possible clinical signs and symptoms. Cohorts and patient populations are not well defined leading to high failure rates in clinical trials. 126 These populations need to be better defined as opposed to one heterogenic population in order for success rates to improve. A better understanding of the pathophysiology and various cellular processes involved in sepsis will aid to better define sepsis as a set of distinct biochemical disorders that can be targeted when creating interventions and therapies.
As we hope is clear to the reader, research continues in hopes of identifying highly sensitive and specific biomarkers. Ultimately, prospective biomarkers must be able to translate from the lab to a clinical setting, be easy to implement/interpret, and be cost-effective enough that they can be utilized routinely in patient diagnosis and treatment. As research continues, a greater understanding of the pathophysiologic causes of sepsis will be attained, leading to more accurate definitions of sepsis/SIRS in distinct patient populations and thus leading to better targets and allowing biomarkers to aid in therapeutic decision-making and ultimately improve the outcome for patients.