
Abstract
Objective
To study cytosolic cathepsin D behavior and possible relationship with other clinical and biological parameters in women affected by breast invasive ductal carcinomas and older than 70 years (range: 71–88).
Material and methods
cytosolic levels of cathepsin D were determined by an Immunoradiometric Assay (IRMA-CIS France). Clinical and biological factors analyzed were: size, axillary lymph node involvement, distant metastasis, histological grade, ploidy, S phase cell, cytosolic estrogen receptor, progesterone receptor and pS2, and concentrations of epidermal growth factor receptor (EGFR) in cell membranes.
Results
Cathepsin D concentrations ranged between 13 and 1228 pmol/mg prot. Median value of 41 was considered as threshold of positivity. Cathepsin D positive tumors showed higher S-phase values (P = 0.046) and were most often histological grade III (P = 0.047). However, the most important finding was the existence of a positive correlation (r = 0.51786) and statistically significant (P < 0.05) between S-phase values and cathepsin D in the overall group of tumors, and those ER+, but not in ER-. We determined cathepsin D concentrations in 131 women with invasive ductal breast carcinomas, but aged between 50 and 70 years (median 61) and we did not find differences based on those values in women >70 years. In addition, we found no correlation between S-phase values and Cathepsin D, both overall and in relation with hormone dependence (ER).
Conclusions
Those results led us to the following conclusions: (1) cytosolic concentrations of cathepsin D in invasive infiltrating breast carcinomas in women over 70 are similar to those seen in women with the same type of tumor, but aged 50 to 70 years and are associated with increased cell proliferation measured by S phase, and histological grade III; (2) in women older than 70 years, cathepsin D concentrations are statistically significantly correlated with phase synthesis values in hormone-dependent tumors, but not in hormone-independent, fact not observed in infiltrating ductal breast carcinomas of women aged between 50 and 70. This could reflect a different mitogenic role of the aspartyl protease enzyme linked to hormone dependence as age function parameter.
Introduction
Breast cancer is one of the most common tumors in women. The primary risk factor for breast cancer is age. Overall incidence is almost 50% in women ≥65 years, modified to 47% in women with more than 70 years.1,2 In addition, life expectancy of women aged over 70 is 15.5 years and half of them live longer, so their risk may increase significantly. Women older than 70 years old are an important group we must focus our attention because of its significant social importance.
Several papers in the literature on breast tumors in women over 70 years confirm a high rate of co-morbidity and ER positivity (85%). 3 It is accepted that those tumors show better clinical and histological features. 4 However, our group has observed that characteristics and clinical and biological behavior of breast carcinomas in women over 70 differs depending of their origin. Tumors were bigger with greater axillary involvement and distant metastases if come from a normal breast medical visit; however, from screening there were no differences with tumors of women aged 55–70 years. 5 We also appreciate that hormone dependence has less influence on tumor characteristics in women older than 70 years versus those aged from 50 to 70. 6 We must remember that age defines treatment, tending to be less aggressive and, sometimes, out of protocol.3,7
Cathepsin D is an aspartic protease of the pepsin superfamily. Similar to other aspartic peptidases, mature cathepsin D is formed after several proteolytic changes occurring in different cellular compartments. Procathespsin D (MW 52 kDa) is transported to lysosomes and in the acidic milieu undergoes further proteolytic processing forming cathepsin D (MW 44 kDa) that becomes two-chain molecules of 31 and 14 kDa. The major function of cathepsin D is the intracellular catabolism within the lysosomal compartment 8 and is necessary for postnatal tissue homeostasis maintenance 9 and tissue remodeling. It also plays an important role in immunity, 10 in cellular senescence induced by ionizing radiation or certain drugs, 11 apoptosis12,13 and in degradation of advanced glycation-end products (AEGs). 14 Recently, a new and important role was described in adipogenesis control, with an increased expression in adipose tissue, which confers a high pathophysiological interest, because obesity increases cancer breast incidence. 15 In addition to these physiological functions, cathepsin D is involved in the pathogenesis of neurodegenerative, skin, cardiovascular and tumoral diseases. 9 In these pathologies, cathepsin D is aberrantly produced and processed in malignancy, and in tumors is over-secreted to the cell microenvironment, acting as tumor and stromal cells mitogen, also its hypersecretion lead to excessive degradation of the extracellular matrix, which contribute to tumor progression and metastases. 16 The majority of cathepsin D is found in soluble parts of most of human cells, while about 20% is apparently membrane bounded. 17
Parallel to cathepsin D, there is also great interest in procathepsin D because it is the most abundant protein secreted by breast cancer cell line MCF7. 18 It is found in the Golgi complex, enzymatically inactive and over-expressed and secreted by certain mammary tumors in the presence of estrogen and progesterone. The secreted procathepsin D has the ability to stimulate growth, cancer cell proliferation and metastasis formation. 9 For this skill, the entire 27–44 amino acid region of the activation peptide 19 is essential. It is also involved in programmed cell death-apoptosis. 20 In estrogen receptor positive cell lines, procathepsin D is secreted only after estrogen stimulation, meanwhile it is constitutively secreted in ER- cell lines. 17
The similarity of some biological actions between procathepsin D and cathepsin D, the different dosing methods that occasionally detect both molecules, and the lack of standardization of them have caused conflicting results about its clinical usefulness. 21
There are several studies about cathepsin D behavior in breast carcinomas where it appears as an indicator of a poor outcome, 14 especially in ER+ patients,22–25 although guidelines do not accept its use as a routine prognostic factor because of the aforementioned discrepancies in the literature. 26 Also, procathepsin D level increases in plasma of patients with metastatic breast carcinoma. 27 However cathepsin D behavior in breast tumors of women over 70 is less known, together with the fact these women represent a high health impact group leading us to perform this study, analyzing the cytosolic tumor content of this and its relationship with tumor-related clinical and pathological parameters.
Material and Methods
The study group included 57 women with breast infiltrating ductal carcinomas aged between 71 and 88 years (76.5 ± 4.6, median 76) without previous treatment and diagnosed at the Breast Pathology Unit of Hospital Monte del Naranco of Oviedo (Spain). Cytosols and cell surfaces were obtained following the EORTC protocol for estrogen receptors assay. The analyzed parameters were: size, lymph node involvement (N), distant metastasis (M), histological grade (HG), ploidy, cellular synthesis phase (SP) [measured both by flow cytometry on fresh samples (Becton Dickinson. USA)], cytosolic concentrations of ER, PR (EIA. Abbott. USA), pS2 (IRMA CIS France), cathepsin D [IRMA CIS France, an immunoradiometric assay to determine the amount of cathepsin D (48 kDa and 34 kDa) and procathepsin D (52 kDa), and with a detection limit of 20 fmol/mL], and epidermal growth factor receptor (EGFR; RLG, Viennalab, Austria) levels in cell membrane. All these parameters were expressed by mg of protein determined by Bradford method. 28
Statistical studies were performed using SPSS software for windows. We conducted a descriptive statistics of quantitative variables and after distribution study with Kolmogorov-Smirnov test; with exception of age, all presents a non-Gaussian distribution, so we use non-parametric statistical tests (comparison of means: Mann-Whitney and Spearman correlations between two variables). Additionally a chi-square test with Yates correction was used, when necessary, to compare qualitative variables. Results were considered statistical significant when P value was less than 0.05.
Results
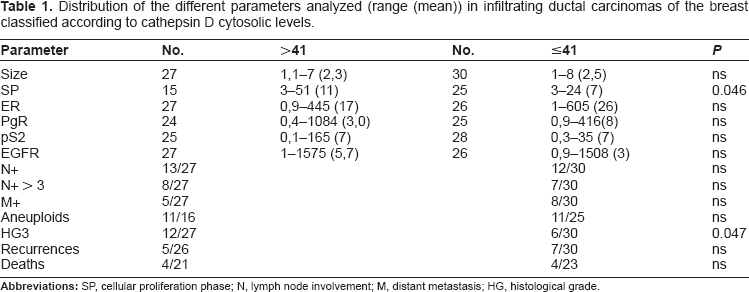
Cathepsin D cytosolic concentrations oscillated between 13 and 1228, with a median of 41, and 25 and 75 percentile values of 34 and 59 pmol/mg prot. respectively. We have taken as the threshold of positivity the value of 41 pmol (mg prot.). When tumors were classified according to this threshold (Table 1), we observed that cases with high concentrations of cathepsin course exclusively with higher values of cell synthesis phase (P = 0.046) and were more often histological grade III (P = 0.047). Furthermore, we find a significant positive correlation (r = 0.51786) between SP values and cathepsin D in the overall group of patients, remained in ER + (> 10 fmol/mg prot.) (r: 0.6835), but not in ER– tumors. We followed 52 patients over a limited time period from 1 to 171 months (40.7 ± 34.3, median 36), and no difference in recurrence number or tumor related-deaths were found between both patient subgroups. Also, we cannot find differences when considering positive or not for estrogen receptors neither.
Distribution of the different parameters analyzed (range (mean)) in infiltrating ductal carcinomas of the breast classified according to cathepsin D cytosolic levels.
Based on our results, we determined cytosolic cathepsin D concentrations in 131 women with infiltrating ductal carcinoma, but aged between 50 and 70 years (60.9 ± 5.4, median 61), founding those ranged from 8 to 201.5 with a mean of 54.0 ± 34.8 and a median of 44.9 pmol/mg prot, with no statistical differences with values over 70 years. In that group, cathepsin D was not related with cell synthesis phase, not as a whole, or in ER+ and ER– tumors.
Discussion
Cathepsin D is an aspartyl-protease with many physiological functions mainly linked to cleave structural and functional proteins and peptides. Three molecular forms of cathepsin D are found in the cell: the precursor (Procathepsin D), the intermediate single-chain and the mature double-chain. 21
This enzyme plays an important role in mammary gland remodeling 29 and can be detected in nipple fluids, where their concentrations are higher in patients with breast cancer compared to benign conditions. 30 Experimental studies have shown this to be related to the development and progression of many tumors and thus made were used as a tumor marker for clinical. With regard to breast tumors and using immunological techniques (EIA and IRMA) it has been demonstrated that its cytosolic concentration were associated with large tumors, with axillary lymph node involvement, infiltrate ductal subtype, hormone dependence, advanced histological grade and aneuploidy. Also cathepsin D cytosolic levels were an independent poor prognosis factor, either in cases with nodal involvement, 31 or regardless of menopausal status and axillary involvement.32,33
We know that principal risk factors for breast tumors are sex and age, and at present women over 70 years acquire a strong interest because they represent a large candidate cluster to develop this tumor. Although there are many current studies about these tumors, few analyze the interest of cathepsin D. Using a positive threshold value of 41 pmol/mg prot., which represents the whole group analysis median, we found that positive cases were associated with increased cell proliferation (measured by cell synthesis phase) and histological grade III. They are not associated with lymph node involvement or distant spread. This could suggest a possible value of cathepsin D as an indicator of poor prognosis, as described in the literature.34,35 However, our most significant finding was the existence of a statistically significant correlation between SP values and cathepsin D when all tumors were considered, results that persisted in hormone-dependent tumors (ER > 10 fmol/mg prot.), but not in hormone-independent. This correlation between cathepsin D and S phase was not found in women with the same histological subtype, but with an age between 50 and 70.
The relationship between cathepsin D and tumor cell proliferation has been known for many years, but this effect is preferably achieved through procathepsin D, it has been shown that secreted procathepsin D has the ability to stimulare growth and cancer cell proliferation.36–38 It is interesting to note that role of procathepsin D is not only as a precursor of a hydrolytic enzyme within the lysosomes but also included an interaction with other molecules which has a mitogenic effect in certain tissues. Also tumor cells overexpressed and secreted procathepsin D modify tumor neighboring cells growth acting in a paracrine or autocrine way. 17 Further, the fact that cathepsin was correlated with S phase only in hormone dependent tumors support the important role of procathepsina D, because in estrogen receptor positive (ER+) cell lines, it is secreted only after estrogen stimulation, while it is secreted constitutively in ER– cell lines. 17 Recently, Mazouni et al 22 have not observed differences in cathepsin D concentrations or hormone dependence, but in patients with breast tumors that are positive or highly positive, high concentration of cathepsin D was associated with a worse prognostic being tumor size value as a predictor of a poorer behaviour and evolution. We could not study the prognostic value of cathepsin D because our follow-up period was very low (median 36 months). However, the most relevant data of our study was a significant statistical correlation between cathepsin D and cell proliferation measured by S phase found in the group of patients with infiltrating ductal breast carcinomas over the age of 70 years taken together and in the hormone dependent type, whereas we could not find it in women with the same histological subtype, but with an age between 50 and 70. Perhaps all this could reflect a clear mitogenic role (due to estrogenic hormonal effect of aspartyl protease) in women with breast cancers and age >70 years, without being able to clarify the contribution of procathepsin D and other molecular forms.
Those results led us to the following conclusions: (1) cytosolic concentrations of cathepsin D in invasive infiltrating breast carcinomas in women over 70 are similar to those seen in women with the same type of tumor, but aged 50 to 70 years and are associated with increased cell proliferation measured by S phase, and histological grade III; (2) in women older than 70 years, cathepsin D concentrations are statistically significantly correlated with phase synthesis values in hormone-dependent tumors, but not in hormone-independent, fact not observed in infiltrating ductal breast carcinomas of women aged between 50 and 70. This could reflect a different mitogenic role of the aspartyl protease enzyme linked to hormone dependence as age function parameter.
Author Contributions
Conceived and designed the experiments: AR, MH and JIA. Analysed the data: AR and JIA. Wrote the first draft of the manuscript: AR and MH. Contributed to the writing of the manuscript: AR, MH and JIA. Agree with manuscript results and conclusions: AR, MH and JIA. Jointly developed the structure and arguments for the paper: MH and JIA. Made critical revisions and approved final version: AR, MH and JIA.
Disclosures and Ethics
Author(s) have provided to the publisher signed confirmation of: Authorship and contributorship, Conflicts of interest, Privacy and confidentiality Protection of human research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Authors reflect there is no conflict of interest that might pose a disagreement in connection with this paper.