
Abstract
Background
Several studies have evaluated histologic features of nonneoplastic breast parenchyma in patients with BRCA1/2 mutations, but the results are conflicting. The limited data suggest a much higher prevalence of high-risk precursor lesions in BRCA carriers. Therefore, we designed this study to compare the clinicopathological characteristics of peritumoral benign breast tissue in patients with and without deleterious BRCA mutations.
Methods
Women with breast cancer (BC) who were referred for genetic counseling and underwent BRCA genetic testing in 2010 and 2011 were included in the study.
Results
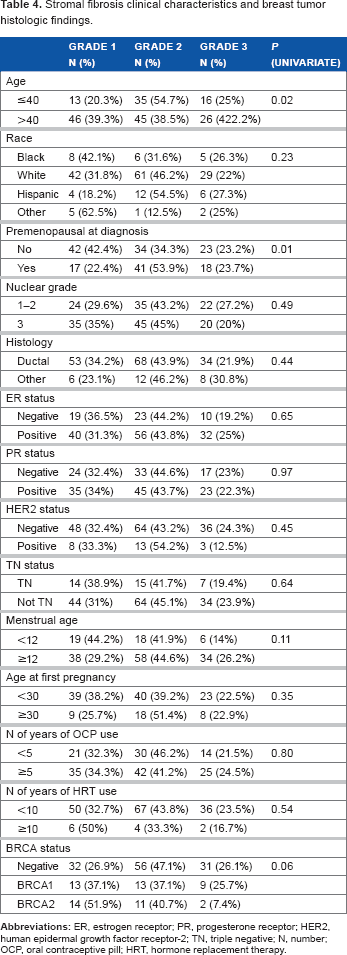
Of the six benign histological features analyzed in this study, only stromal fibrosis grade 2/3 was found to be statistically different, with more BRCA noncarriers having stromal fibrosis grade 2/3 than BRCA1/2 carriers (P = 0.04).
Conclusion
There is no significant association between mutation risk and the presence of benign histologic features of peritumoral breast parenchyma.
Keywords
Introduction
About 5% to 10% of all breast cancers (BCs) are hereditary.1,2 Known mutations in the BC susceptibility genes BRCA1 and BRCA2 account for more than 50% of hereditary BC. 3 Women who carry a germline mutation in BRCA1 or BRCA2 have a 43% to 84% BC risk and a 22% to 39% ovarian cancer (OC) risk by the age of 70 years.4–6
The majority (90%) 7 of lesions that occur in the breast are benign. Benign breast diseases (BBDs) become more common during the second decade of life and peak during the fourth and fifth decades; incidence of malignant disease, however, continues to rise after menopause.8–10 Family history (FH) of BC,11,12 obesity, 13 fibroglandular breast tissue density of at least 25%, 14 and estrogen-receptor (ER) expression in epithelial hyperplasia lacking atypia and in adjacent normal lobules 15 have been identified as risk factors for BBDs.
BBDs include a spectrum of lesions ranging from developmental abnormalities, inflammatory lesions, and epithelial and stromal proliferations to various neoplasms. 16 Fibroadenoma and fibrocystic changes are the two most common BBDs.13,17,18 Although nonproliferative disease does not appear to be associated with increased BC risk, 19 proliferative disease without atypia and that with atypia (ductal carcinoma in situ, atypical hyperplasia, and sclerosing adenosis) have been associated with a 1.5- to 4-fold increased risk for BC, respectively.16,20,21
Although monitoring may be thorough and frequent, more than 50% of tumors in patients with BRCA1/2 mutations are identified between screening evaluations (interval carcinomas). It has been postulated that BRCA-associated carcinomas may develop and progress more rapidly than sporadic (nonhereditary) BC.22,23 Preneoplastic lesions associated with BRCA1/2 mutations and sporadic BC are different. Several studies have evaluated histologic features of nonneoplastic breast parenchyma in patients with BRCA1/2 mutations, but the results are conflicting.24–32 Overall, the limited available data suggest a much higher prevalence of high-risk precursor lesions in BRCA carriers.26,29,31,33–35 Moreover, studies examining histopathologically normal breast parenchyma adjacent to BRCA-associated BCs suggest a field effect of genetic changes preceding morphologic changes in the mammary glands.36–39 Loss of heterozygosity (LOH) of the wild-type BRC A1/2 allele in normal breast epithelial tissue and benign breast lesions was detected in 56% to 81% of BRCA1/2 carriers with BC.40,41 Importantly, LOH was more commonly seen with benign proliferative changes such as sclerosing adenosis, which suggests that these nonmalignant tissues harbor significant amounts of genetic alterations that may predispose to malignant transformation.40,41 Cytogenetic abnormalities in prophylactic mastectomy specimens characterized by hyperplasia without atypia in patients with a positive FH of BC (but unknown BRCA status) were also present.42,43 It is not known whether benign histopathological changes are related to the BRCA-associated hereditary breast-ovarian cancer spectrum.
This retrospective analysis evaluated histopathologic features of nonneoplastic peritumoral breast parenchyma. The goal was to determine whether there are histopathologic differences in nonneoplastic breast parenchyma in patients with BRCA1/2 mutation-associated BC and sporadic BC.
Materials and Methods
Patient population and data collection
The prospectively maintained Breast Cancer Management System database at the University of Texas MD Anderson Cancer Center (UTMDACC) identified 181 women with BC who were referred for genetic counseling and underwent genetic testing for BRCA1 and BRCA2 gene mutations in 2010 and 2011. All women were physician-referred to the Clinical Cancer Genetics Program at the UTMDACC Breast Center based on a multigenerational FH of BC and/or OC, Ashkenazi Jewish ancestry, or young age (≤50 years). Patients with metastatic BC or those with BRCA mutations that indicated a variant of uncertain significance were excluded from the analysis.
This study was approved by the UTMDACC Institutional Review Board. The retrospective analysis of prospectively collected data included age at the time of BC diagnosis, reproductive history, FH of BC and/or OC, oral contraceptive pill use, hormone replacement therapy (HRT) use, meno-pausal status at the time of BC diagnosis, previous history of BC, and tumor characteristics.
Pathologic assessment and mutation analysis
All patients underwent definitive surgery either before or after genetic testing, and the pathologic specimens were reviewed by dedicated breast pathologists at UTMDACC. Invasive BC (IBC) was confirmed on initial core biopsy specimens. Histologic type and tumor grade were defined according to the World Health Organization classification system 44 and the modified Black's nuclear grading system, 45 respectively. Immunohistochemical (IHC) analysis was used to determine ER and progesterone-receptor (PR) status. Negative ER and PR status was defined as nuclear staining of 1% or fewer cells on IHC. Human epidermal growth factor receptor-2 (HER2)-negative status was defined as either 2+ or fewer cells or no staining by IHC and/or absence of gene amplification by fluorescence in situ hybridization.
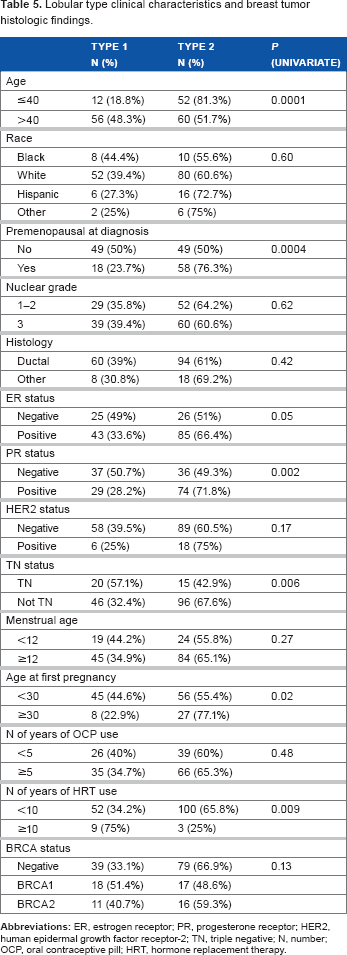
Peritumoral breast parenchyma was reviewed retrospectively for six histological features: benign proliferative breast disease (BPBD) with and without atypia, stromal fibrosis (SF), lobular type (LT), lobular contour (LC), lobular sclerosis (LS), and lobulitis (L). We classified LT based on the predominant pattern as type 1 (<12 acini), type 2 (~50 acini), and type 3 (>50 acini) (Fig. 1).
46
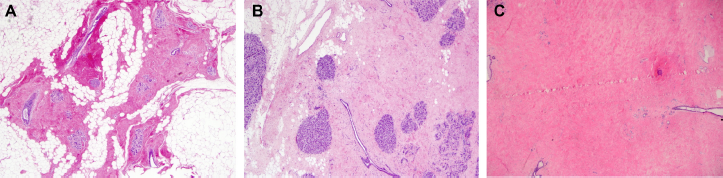
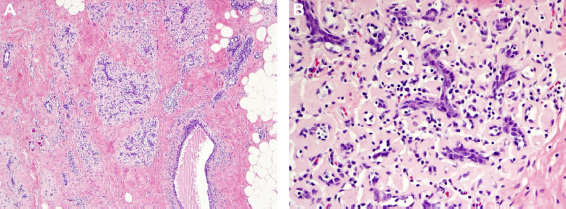
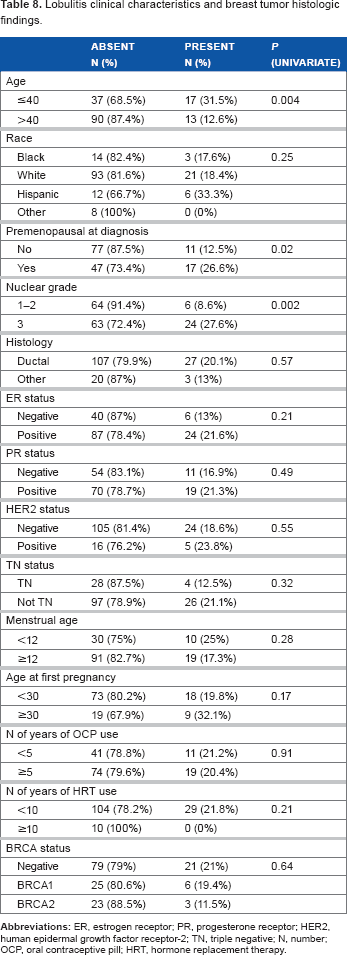
SF was defined as the presence of dense fibrosis occupying more than 90% of the interlobular stroma47,48 and further graded as minimal/absent (grade 1), present (grade 2), or extensive (grade 3) (Fig. 2). L was defined by the presence of more than 100 lymphocytes and/or plasma cells per lobule and in more than one morphologically normal lobular unit not in relation to periductitis or previous biopsy site changes (Fig. 3).
27
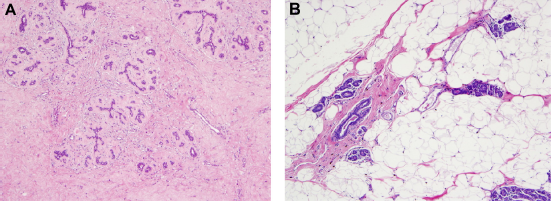
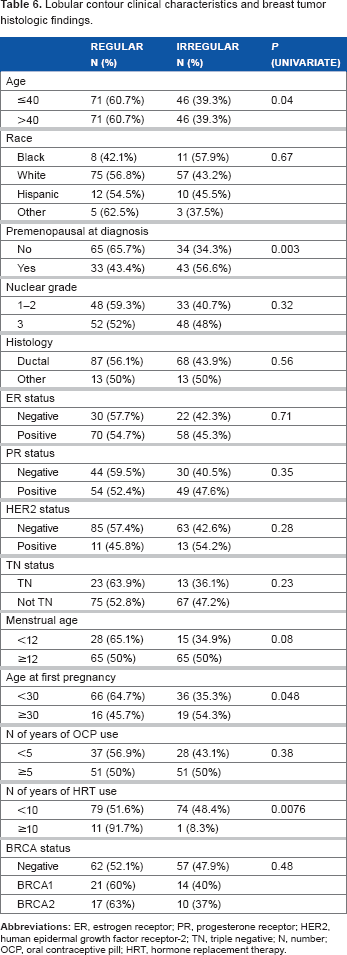
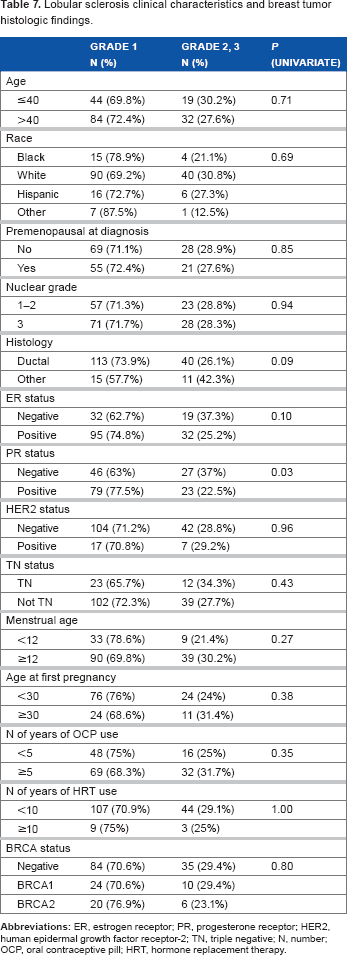
LC was defined as “regular” if the distinct lobular architecture was preserved with smooth borders in more than half of the nonneoplastic lobules. If the borders of nonneoplastic lobular units showed loss of smooth counters and loss of intralobular stroma in at least 50% of lobules, they were classified as “irregular” LCs (Fig. 4). LS was defined as the presence of fibrosis identified as expansion of intralobular stroma with distortion of acinar architecture; it was graded as 1 (mild) if sclerosis was identified in fewer than one-third of lobules, 2 (moderate) if sclerosis was present in more than one-third but fewer than two-thirds of lobules, and 3 (extensive) if sclerosis was present in more than two-thirds of lobules.
The lobular type was classified based on the predominant pattern of lobules. (A) An example of type 1 lobule (<12 acini per lobular unit, x2). (B) An example of type 2 lobule (12–50 acini per lobular unit, x2). (C) An example of type 3 lobule (>50 acini per lobular unit, x2). Stromal fibrosis is defined as the presence of dense fibrosis of the interlobular stroma. (A) An example of a case with minimal fibrosis occupying <50% of interlobular stroma and graded as grade 1 (x2). (B) An example of a case with moderate fibrosis occupying between 90% and 50% interlobular stroma and graded as grade 2 (x2). (C) An example of a case with extensive fibrosis occupying >90% of the interlobular stroma and graded as grade 3 (x2). Lobulitis is defined as the presence of >100 lymphocytes and/or plasma cells per lobule and in more than one morphologically normal lobular unit. (A) Lobulitis view at low power showing multiple lobules with lymphoplasmocytic infiltrate (x4). (B) Lobulitis view at high power showing lymphoplasmocytic infiltrate (x20). Lobular contour is defined as “regular” if the distinct lobular architecture was preserved with smooth borders in more than half of the nonneoplastic lobules. If the borders of lobular units showed loss of smooth contour in at least 50% of lobules, “irregular” lobular contour was classified. (A) An example of regular lobular contour (x4). (B) An example of irregular lobular contour (x4).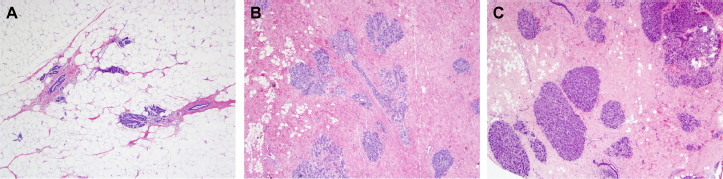
BRCA testing was performed using germline DNA (from blood) by Myriad Genetics Laboratories, Inc. (Salt Lake City, Utah), and test results were categorized as either positive or negative for a deleterious mutation.
Statistical analysis and outcome measures
Demographic and clinical characteristics were summarized and compared between the three groups and defined by the BRCA status (noncarrier, BRCA1 carrier, or BRCA2 carrier), with the chi-square test for categorical variables or the Kruskal-Wallis test for continuous variables. The chi-square test or Fisher's exact test was used to identify the significant factors predictive of a BRCA mutation status. A multivariate logistic regression model was fitted to examine the relationship between BRCA status and benign histological features after adjustment for significant patient and clinical characteristics identified in univariate analyses. P-values ≤0.05 were considered statistically significant; all tests were two-sided. Given the small number of BRCA1 and BRCA2 cases and the exploratory nature of the study, we report P-values without adjusting for multiple testing. Statistical analysis was carried out using SAS 9.2 (SAS Institute Inc.) and S-Plus 8.0 (Insightful Corporation) software.
Results
Association between BRCA positivity, patient demographics, and baseline disease characteristics.
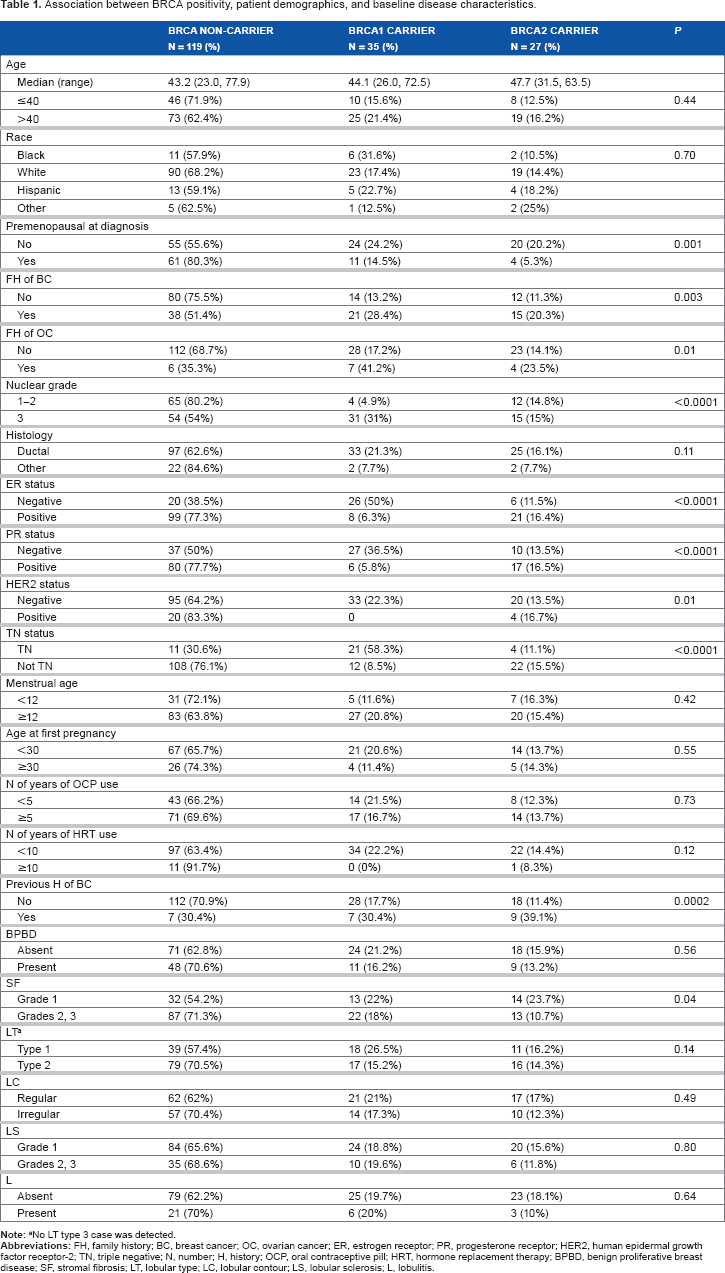
No LT type 3 case was detected.
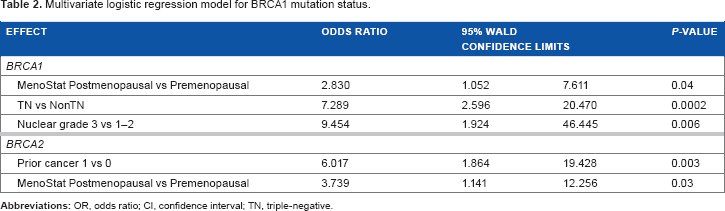
Multivariate logistic regression model for BRCA1 mutation status.
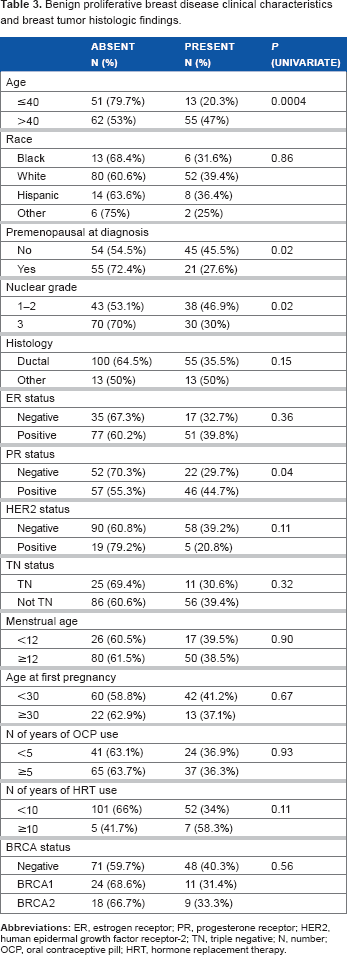
Benign proliferative breast disease clinical characteristics and breast tumor histologic findings.
Stromal fibrosis clinical characteristics and breast tumor histologic findings.
Lobular type clinical characteristics and breast tumor histologic findings.
Lobular contour clinical characteristics and breast tumor histologic findings.
Lobular sclerosis clinical characteristics and breast tumor histologic findings.
Lobulitis clinical characteristics and breast tumor histologic findings.
Discussion
This study investigated whether histopathological features of nonmalignant (peritumoral) breast tissue can help in identifying the risk for BRCA mutation in a selected population of high-risk women with BC. First, we quantitatively assessed the frequencies of the six selected benign histological findings of normal breast tissue of women with BRCA-associated and non-BRCA-associated BC. Although there is a higher incidence of peritumoral grade 2/3 SF in non-BRCA-associated BC than in BRCA1- and BRCA2-associated BC (71% vs 18% and 11%, respectively [P = 0.04]), our data indicate that there is no statistically significant association between mutation risk status and the presence of any of the selected benign histologies. Confirming previous studies,6,34,49–53 we found that postmenopausal status and TN or nuclear grade 3 BC tumors were independent predictors for BRCA1 mutations. BC history or postmenopausal status remained independent, significant predictors for a BRCA2 mutation.
Studies examining peritumoral breast parenchyma have demonstrated histopathological differences between BRCA-associated BCs and non-BRCA-associated BCs. A higher frequency of fibroadenoma54,55 and PR expression 56 (P = 0.0003) was observed in normal breast epithelium adjacent to IBC in BRCA-linked cases than in sporadic cases. Of note, there was no evidence of allelic loss in normal epithelium either adjacent to or at an unknown distance from the tumor in the latter study. 56 Russo et al 57 demonstrated a preponderance of type 1 lobule over type 3 (48% vs 10%) in women who underwent prophylactic mastectomy because they carried the BRCA1 gene or belonged to a pedigree with familial BC. Interestingly, Baer and colleagues 58 suggested that women with predominant type 1 and no type 3 lobules who have breasts that likely have undergone more complete involution have a lower BC risk than those with no type 1 lobules or mixed lobule types (OR, 0.63; 95% CI, 0.44–0.91). We did not find any association between LT and higher mutation risk; however, study design may influence the interpretation of data that assessed LT after BC diagnosis (and consequently may not reflect LT prior to BC development).
Mangia et al 59 examined the histopathological features of peritumoral and primary tumor breast tissue to assess mutation risk associated with BRCA1/2 genes. Among peritumoral lesions, only epithelial proliferative lesions were related to higher mutation risk in patients with familial BC (P = 0.003), and a significant difference in terms of high mutation risk was observed in usual ductal hyperplasia lesions (42% high-risk vs 17% low-risk patients; P = 0.002). A study conducted by Hermsen et al 27 detected T-cell lobulitis more frequently in prophylactically removed breast tissue from women at hereditary high risk for BC (N = 21/41, 51%) compared to controls (N = 8/82, 10%) (P < 0.0001). In another study, 32 lobulitis in nonneoplastic breast tissue was independently associated with TN cancers, younger age at diagnosis, and medullary phenotypes—features that are commonly described in hereditary BC. In our study, lobulitis was more common in younger patients; however, we could not demonstrate an association with a specific BC phenotype.
In addition to overall architectural differences, breast tissues in BRCA carriers have histological differences in intralobular and interlobular stroma. 57 Intralobular stroma contrasts with interlobular stroma, which has fewer cells separated by larger quantities of more compact collagen. In our study, BRCA noncarriers had denser interlobular stroma (SF grade 2/3) than BRCA carriers. Our findings are in agreement with those of Mangia et al, 59 which confirm that atrophy and fibrosis are associated with a lower mutation risk. Worsham and col-leagues 60 demonstrated that fibrosis was protective against BC; in fact, women with fibrosis were at lower risk for BC progression than women without fibrosis. In contrast, Russo et al 57 found that the intralobular stroma was more fibrotic and dense in women with familial BC than in those with sporadic BC who had mastectomy or women without BC who underwent reduction mammoplasty, which explains in part the increased mammographic density in women with familial BC. 61
The pathologic characteristics of BRCA1/2-related BC (eg, being more often medullary-like, TN, and showing a “basal” phenotype of BRCA1-associated BCs) have been taken into account in cancer clinics to help predict which patients may harbor BRCA germline mutations.49,62 At present, however, no BC risk model incorporates proliferative lesions without atypia, high breast density, or benign histopathological breast tissue changes into risk calculations.63–65 Our results suggest that no benign histologic feature is associated with BRCA mutation; consequently, there is no reason to regard these features as predictive factors in BRCA models. These findings, however, do not exclude the possibility that molecular or serologic changes may occur without causing a recognizable histologic change that might be used for early detection. If future studies define histopathological features that can be used to predict BRCA1/2 status, BC risk assessment models may be improved by incorporating the full range of biopsy results into risk calculations. This may have implications for the mutation screening process. Furthermore, studies examining the associations between selected benign histologic findings and normally considered BC-related risk factors may shed light on hereditary BC carcinogenesis models.
This study has several limitations. This analysis was conducted among a small subset of BRCA mutation carriers, which reduced the number of available cases and controls for the analysis and, consequently, the statistical power of the study. Peritumoral benign histological findings may not represent the predominant histology in the rest of the breast, which can lead to some misclassification. However, because the pathologists were blinded to case-control status, any mis-classification would be unrelated to outcome.
In summary, our data show that the selected benign histological features of the peritumoral breast parenchyma should not be used as a marker with which to identify patients who are likely to carry mutations in BRCA1 or BRCA2 genes. The significance of other benign histological changes in normal breast parenchyma among BRCA carriers without a BC history necessitates further evaluation in larger prospective studies and in other populations. Such investigations may reveal carcinogenic pathways specific to hereditary BC. Enhanced knowledge of these pathways potentially may lead to novel therapeutic targets.
Author Contributions
Conceived and designed the experiments: AS, HQ, YS. Analyzed the data: DL, AMG, BA, SB, YS. Wrote the first draft of the manusciprt: SB. Contributed to the writing of the manuscript: SB, HQ, DL, AMG, BA, AS. Agree with manuscript results and conclusions: SB, HQ, DL, AMG, BA, AS, YS. Jointly developed the structure: SB, HQ, DL, AMG, BA, AS. Made critical corrections: SB, HQ, DL, AMG, BA, AS. All authors reviewed and approved of the final manuscript.