
Abstract
The relationship between cancer and inflammation is a complex but intimate one. Decades of work has shown to us that cancer progression is influenced by a multitude of factors, including genetic, environmental, and immunological factors. We often overlook that cancer progression is also a pathological consequence of a dysregulated inflammatory control in the body. A current emerging topic in cancer research is the role of inflammasomes in carcinogenesis. The inflammasome is a multicomplex protein platform that when activated results in the release of proinflammatory cytokines, such as interleukin (IL)-1β. There is increasing evidence suggesting that IL-1β plays a pivotal role in cancer progression. This short review proposes the possibility of using IL-1β as a potential cancer progression biomarker and discusses the use of saliva as a model biological fluid for measuring physiological IL-1β levels in the body.
Introduction
Saliva is a clear, slightly acidic liquid, which is secreted from the salivary glands into the oral mouth cavity. Several years of research into identification of an array of biomolecules in saliva has opened new avenues into the field of salivary diagnostics. Given its noninvasive and rapid collection process, saliva possesses the qualities of a bodily fluid with high potential for the diagnosis, monitoring, and study of several diseases. 1 Saliva is able to provide reliable clinical data and cellular information concerning biologically active molecules that can be used to evaluate and monitor the health-disease process.2,3 Approximately 27% of proteins are common between saliva and blood plasma. 4 Furthermore, saliva has an advantage over blood in that it contains low background of normal material and inhibitory substances and fewer complexes than blood. 5 Therefore, saliva is a good alternative to blood for diagnostic tests and presents a potential reservoir for researchers to identify new biomolecular markers.
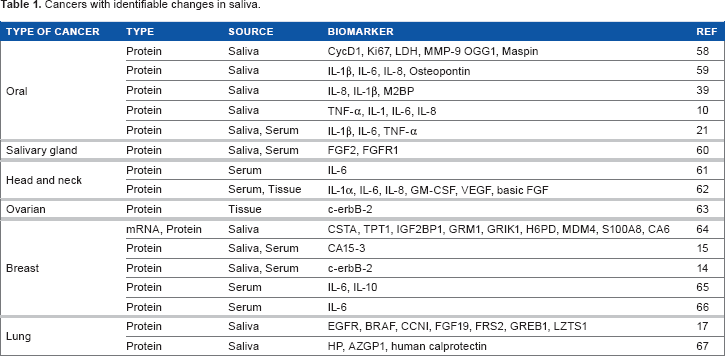
Cancers with identifiable changes in saliva.
This review focuses on one potential cancer biomarker, interleukin (IL)-1β (also known as catabolin, IL-1, and IL1F2), which has recently received attention in immune-cancer biology research.
IL-1β: A Potential Cancer Progression Biomarker?
IL-1β is a key inflammatory cytokine released upon infection, cellular injury, or antigenic challenge. This cytokine directly acts on various cell types, either alone or in combination with other inflammatory cytokines, to induce an inflammatory state or the “fever response.” IL-1β is a proinflammatory cytokine released upon activation of a multi-protein innate immune pathogen-sensing complex called the inflammasome. 18 The preformed IL-1β has to be proteolytically processed by an important cysteine protease, caspase 1, upon inflammasome activation to result in the secretion of an active and mature form of IL-1β. Inflammasomes can be induced to a variety of stimuli, including microbial components (eg, bacterial toxins) and environmental par-ticulates (eg, silica and asbestos). 18
Inflammasomes have been linked to carcinogenesis and the maintenance of a tumorigenic microenvironment.19,20 It is likely that inflammasomes may play a critical role in the formation and progression of cancer through their contribution to inflammation, immune responses, and tissue homeostasis. Although macrophages are the largest producers of IL-1β, other cell types from various tissue sources can also produce epidermal tissue, mucosa epithelial cells, acinar, and ductal cells of the salivary glands. However, limited work has been put into studying the levels of IL-1β and its relationship with different types of cancers. Given the growing number of evidences that cancer progression correlates with an increase in IL-1β, 21 it is reasonable to suggest that IL-1β could be a potential biomarker as a predictor of cancer risk or cancer prognosis.
It is well known that polymorphisms of IL-1 receptor 1 (IL-1R1) and IL-1β have been associated with disease progression and prognosis.22,23 IL-1β has been found to be elevated in various types of cancers, and it is known that IL-1β producing tumors have bad prognoses. 4 The IL-1 family of cytokines are a group of pleiotropic cytokines that can induce several genes that significantly promote cancer growth and metastasis, such as vascular endothelial growth factor (VEGF) and tumor growth factor (TGF)-β. It is important to note that like many other proinflammatory cytokines, IL-1β exerts both beneficial and harmful effects in human beings. In cancer, IL-1β is the most clinically important IL-1 subtype and has attracted a lot of attention in the past decade, especially in the way this cytokine is activated. Therefore, tumors that express IL-1β must be proteolytically processed into its active form, via the inflammasome, before it can exert its physiological effects. IL-1β can induce the expression of adhesion molecules, increase prostaglandin production, and chemokine release. 24 All these contribute to cell chemotaxis, angiogenesis, and increase in cell adhesiveness, the typical hallmarks of cancer growth and spread.
There is growing evidence that inflammasomes may be playing a critical role in tumorigenesis. Inflammasomes play an active role in regulating proinflammatory signals and shaping the adaptive arm of the immune system (eg, T-cells). Therefore, it is no surprise that a dysregulation of inflammasome activity could influence disease outcomes and tumorigenesis. Cancer development can arise from various physiological stresses evoked by typical cancer risk factors such as viral infections, tobacco smoke, obesity, and aging, which results in inflammation. Once tumors arise, the maintenance of the tumor is critical for the cancer to spread and survive. It is suggested that inflammatory immune cells like macrophages and T-cells construct and orchestrate this favorable tumorigenic microenvironment by supplying cancer cells with cytokines, chemokines, and growth factors.
Despite the beneficial effects of inflammasome activation (as in the case of combating microbes), adverse effects of inflammasomes have been reported. Overt or excessive inflammasome activation could possibly drive and sustain tumorigenesis (eg, skin cancer). However, the loss of inflammasome activation could also increase the likelihood on cancer progression (eg, gastrointestinal cancer).
In gut-associated malignancies, loss of inflammasome components has been shown to increase tumor growth in several colitis mouse models.25–29 This was shown to be attributed to the lack of IL-18 production, an important cytokine secreted in response to inflammasome activation. Normally, IL-18 functions as a factor to maintain tissue homeostasis and promote an antitumorigenic microenvironment.
In melanomas, the most malignant type of skin cancer, important inflammatory cytokines such as IL-6, IL-8, and IL-1β are upregulated. Interestingly, all these cytokines can be regulated by active IL-1β.30,31 Elevated levels of IL-1β in melanomas can influence tumorigenesis and also increase the recruitment of immune suppressor cells to further reduce antitumor immune surveillance. 32 Indeed, loss of IL-1R and caspase 1 genes resulted in significantly reduced tumor growth and incidence in a chemical-induced skin cancer mouse model. 33 This suggests that there is a possible strong interplay between inflammasomes and skin cancer progression.
There is some evidence to show that inflammasome activation may play an important role in breast cancer. The crucial inflammasome mediator IL-1β plays an important role in the progression of breast cancer, although direct evidence linking to inflammasomes has yet to be established. However, there is a strong correlation between breast cancer tumor aggressiveness and IL-1β levels. 34 Work by Kurtzman et al 35 demonstrated that IL-1β expression is increased in 90% of invasive breast carcinomas and that it is localized to both tumor cells and stromal cells. Elevated IL-1β levels in breast cancer are associated with a more aggressive phenotype and higher tumor grade.36,37 Furthermore, in a mouse model of human breast cancer, fibroblast growth factor (FGF) 1-induced mammary tumorigenesis is associated with local production of IL-1β. 38 Overall, it is possible that the levels of IL-1β might be related to different stages of breast cancer.
Saliva: A Model Biological Fluid for Measuring IL-1β
In the tumor microenvironment, both malignant and infiltrating immune cells secrete these cytokines, influencing tumor progression and eventual tumor dissemination. The levels of IL-1β have been shown to increase in oral types of cancers.21,39,40 Elevated IL-1β levels are detected in the human lung, colon, breast carcinoma, and skin melanomas. 4 However, in all these studies, IL-1β have only been measured in the serum, not saliva. Out of all cancers studied, salivary IL-1β has only been measured in oral cancer patients (Table 1). Indeed, several groups have also measured IL-1β from saliva in other noncancer-related pathologies, including peri-implant inflammation in patients with dental implants, 41 periodontitis,42,43 and graft-versus-host disease. 44 This suggests that saliva can be used as a diagnostic tool for detecting early stages of cancer.
Tumors are heterogeneous and consist of many cell types in addition to cancer cells, including cancer-associated fibroblasts, different tumor infiltrating immune cells, adipocytes, and endothelial cells to list a few.45,46 All these cells have the ability to secrete immune-important cytokines and chemokines, which can directly affect cancer cells or cause cancer-associated inflammation. In malignancies where there is a low survival rate from time of diagnosis, high serum concentrations of IL-1 cytokines (ie, IL-1β and IL-1α) are usually present. 4 In general, tumors that produce IL-1 have bad prognoses and high IL-1 concentrations within the tumor microenvironment are usually associated with a more virulent tumor phenotype. 47
Researchers working with saliva biomarkers and diagnostics are always faced with the dilemma of whether the levels of target biomarker in saliva correlate with that in the blood circulation. Some studied biomarkers show correlated changes between saliva and serum or plasma. For example, a positive correlation exists between salivary and serological levels of antigen CS 15-3 and the oncogene, c-erb, where it was shown to be significantly higher in breast cancer patients than in healthy controls.14,15,48 On the other hand, biomarkers such as IL-8, a potential biomarker for oral squamous cell carcinoma (OSCC), could be detected at higher concentrations in saliva than serum. 49 However, the relationship between salivary and blood IL-1β is not clear. However, what is now clear is that circulating IL-1β in the blood of healthy individuals is very low and often below the detection limit, 50 whereas it is generally higher in saliva. 21 Resende et al 44 showed that salivary IL-1β levels increased progressively from the time before diagnosis until weeks after diagnosis, whereas blood IL-1β peak levels could be observed only within the time allotted for diagnosis in an acute graft-versus-host disease clinical study.
The other challenge in salivary biomarker research is the variability in the levels of potential salivary biomarkers in both healthy individuals and cancer patients. The best examples of this are the salivary biomarkers IL-6 and IL-8, which have been proposed as diagnostic markers for OSCC. Wide variation in the reference levels of these biomarkers have been reported in several different studies, 51 making it impossible to determine what ranges of salivary IL-6 or IL-8 levels are likely to indicate OSCC development. These wide variations in the levels of the same salivary constituent across different studies could be due at least partly to the different processing methods used or inherent biological variations within different individuals and groups. Although some degree of heterogeneity in the levels of IL-1β from healthy individuals have been reported, the variation is not as diverse as those reported for IL-6 and IL-8.21,52 Furthermore, variation in salivary IL-1β levels from healthy individuals is only seen at different time periods of the day (ie, higher levels at awakening and lower during sleep). 53 This is not surprising as disruption in circadian system affects directly the production of inflammatory cytokines. 54 From a sample collection aspect, the timing of saliva collection is crucial to avoid such high background noise of salivary IL-1β levels to ensure that it does not mask the changes during disease progression, such as in cancer progression.
Summary
IL-1β is well known as a potent promoter of carcinogenesis.
55
The potential molecular mechanisms by which IL-1β can promote tumor growth and invasion is depicted in Figure 1. However to date, there has been no detailed study investigating the levels of IL-1β at different stages of cancer, let alone in the salivary compartment. The use of salivary biomarkers has been explored for several types of cancers in the past including salivary gland cancer,
56
and cancers remote from the oral cavity such as breast and pancreatic cancer.
57
Furthermore, several studies have reported that salivary constituents can discriminate oral and systemic types of cancers (eg, lung cancer, breast cancer, pancreatic cancer, and ovarian cancer). We have briefly summarized the potential use of saliva as an alternative diagnostic fluid compared to blood. Although there have been many studies that investigated different types of cytokines and chemokines as potential biomarkers for early diagnosis and progression of cancer, limited amount of research has been done to investigate the correlation of IL-1β and cancer. Recent studies also suggest that the level of IL-β is significantly higher in cancer patients compared to healthy controls, especially oral cancer. Furthermore, IL-1β is more detectable in saliva than in blood serum, suggesting that saliva serves as a good biological fluid for assessing changes in IL-1β levels.
21
Studying the dynamics of IL-1β changes in different cancers will shed light on linking the possible role of inflammasomes in cancer pathogenesis, a field that has gained attention among immunologists in the past decade. Identifying a cancer progression biomarker, especially in saliva, can hopefully predict the progress of the cancer and allow a more personalized anticancer treatment to be given to the patient. Current research has identified deregulated cytokines, such as IL-1β, in some cancers mentioned above. Robust and reproducible methods for the assessment of IL-1β in saliva, and the possibility of a rapid salivary test as an indicator of disease and risk of malignancy are important to qualify IL-1β as a putative cancer progression salivary biomarker. Ongoing development of such a method will have profound impact on cancer screening and the early diagnosis of cancers, potentially resulting in early treatment and a decrease in the high levels of morbidity and mortality associated with different types of cancers.
The inflammasome is a multicomplex system whose activation can be induced by exposure to carcinogens or intrinsic genetic aberrations, the basis of cancer initiation. Upon inflammasome activation, caspase 1 becomes activated, which leads to a cascade of proinflammatory events via the activation of cytokines, such as IL-1β, which then interact with their own membrane receptors amplifying the inflammatory response. On the other hand, active caspase 1 can lead to cell pyroptosis with the consequence of membrane rupture and release of various factors, including IL-1β. Inflammasome effectors (IL-1-like cytokines and pyroptosis) can influence the adaptive immune response and cell proliferative responses in different ways. The activation of the inflammasome complex can lead to the recruitment of suppressive immune cells, such Type 2 helper T-cells (Th2) and regulatory T-cells (Treg), which can favor tumor progression. The inflammasome is also involved in tumor progression through the release of growth factors [eg, fibroblast growth factor 2 (FGF2) and vascular endothelial growth factor (VEGF)], which facilitate angiogenesis and tumor invasiveness.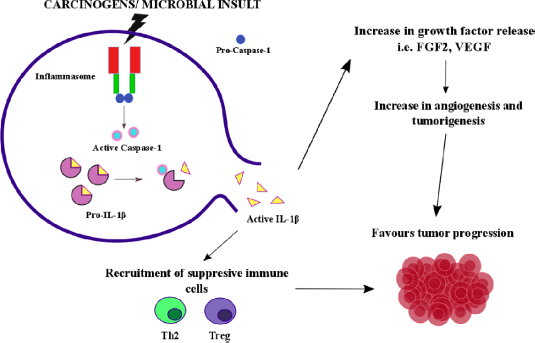
Author Contributions
Prepared the first draft of the manuscript: AI. Contributed to the writing of the manuscript: AI, NBG, and DK. Jointly developed the structure and arguments for the paper: AI, NBG, and DK. Made critical revisions and approved the final version: AI and DK. All the authors reviewed and approved the final manuscript.