
Abstract
Cancer biomarkers have provided great opportunities for improving the management of cancer patients by enhancing the efficiency of early detection, diagnosis, and efficacy of treatment. Every cell type has a unique molecular signature, referred to as biomarkers, which are identifiable characteristics such as levels or activities of a myriad of genes, proteins, or other molecular features. Biomarkers can facilitate the molecular definition of cancer, provide information about the course of cancer, and predict response to chemotherapy. They offer the hope of early detection as well as tracking disease progression and recurrence. Current progress in the characterization of molecular genetics of HIV-associated cancers may form the basis for improved patient stratification and future targeted or individualized therapies. Biomarker use for cancer staging and personalization of therapy at the time of diagnosis could improve patient care. This review focuses on the relevance of biomarkers in the most common HIV-associated malignancies, namely, Kaposi sarcoma, non-Hodgkin's lymphoma, and invasive cervical cancer.
Introduction
Cancer is a genetically and clinically diverse disease, whose pathogenesis, aggressiveness, metastatic potential, and response to treatment can be different among individual patients. 1 Great variations exist, even between individuals with the same type of cancer, suggesting the role of genetic factors in cancer pathogenesis. The risk of developing cancer is greatly increased in human immunodeficiency virus (HIV) setting, and it is increasingly recognized as a complication of HIV infection.2,3 Cancers with an increased incidence in HIV patients include the AIDS-defining malignancies [Kaposi's sarcoma, non-Hodgkin's lymphoma (NHL),and invasive cervical cancer] and other non-AIDS-defining cancers (Hodgkin's lymphoma, hepatocellular carcinoma, and lung cancer). 4 Due to the complexity and diversity of cancer, the application of personalized medicine in the management of cancer patients has been suggested and encouraged.
Personalized medicine hinges on biomarkers, which are highly sensitive and specific in revealing information that is relevant for diagnosis, prognosis, and therapy.5,6 Thus, biomarker discovery and development are one of the cores of personalized medicine for cancer. Cancer biomarkers may be discovered using molecular, cellular, and imaging methodologies focused on drug and disease mechanisms, thus providing critical feedback about the interaction of novel therapies with their intended target and about the disease itself. 7 Biomarkers play a role in cancer screening, early diagnosis, prognosis, cancer stratification, prediction of treatment efficacy, and adverse reaction. A biomarker can consist of genomic and proteomic patterns, single genes or proteins, chromosomal abnormalities, epigenetic signatures, aberrant microRNA (miRNA), as well as imaging changes observed on magnetic resonance imaging (MRI) or positron emission tomography (PET) scan. However, most biomarkers have both prognostic and predictive value.
Biomarker Definition
Biomarkers are characteristics that are objectively measured and evaluated as indicators of normal biological processes, pathogenic processes, and pharmacological responses to a therapeutic intervention.8,9 In cancer, biomarkers are defined as biochemical substances elaborated by cancer cells either due to the cause or effect of malignant process. 10 However, cancer biomarkers must be detectable only in the presence of cancer. Cancer biomarkers may be detected in sample matrices such as serum, plasma, whole blood, urine, and tissue. 11 They can be normal endogenous products that are produced at a greater rate in cancer cells or the products of newly switched on genes that remained inactive in normal cells. Biomarkers may include intracellular molecules or proteins in tissues or may be released into the circulation and appear in serum, and their presence in significant amount may indicate the presence of cancer. However, the usefulness of a biomarker lies in its ability to provide early indication of a disease or its progression, and it should be easy to detect and should be measurable across populations. 12
Cancer Biomarker Classification and Utility
It has been well established that a variety of biomarkers are used in risk assessment, early detection, diagnosis, treatment, and management of cancer.13,14 Molecular analyses at the protein, DNA, RNA, or miRNA levels can contribute to the identification of novel tumor subclasses, each with a unique prognostic outcome or response to treatment. 15 Biomarkers enable the characterization of patient populations and quantitation of the extent to which drugs reach intended targets, alter proposed pathophysiological mechanisms, and achieve clinical outcomes. 16 The most valuable biomarkers are highly sensitive, specific, reproducible, and predictable, and the majority of US Food and Drug Administration (FDA) approved that cancer biomarkers are serum-derived single proteins.17,18
Biomarkers can be classified based on different parameters such as characteristics and function. Biomarkers that are classified according to their functions include type 0 biomarkers, which measure the natural history of a disease and they should correlate over time with known clinical indicators; type I biomarkers are associated with the effectiveness of pharmacologic agents; and type II biomarkers, also known as surrogate endpoint biomarkers, are intended to substitute for clinical endpoints. 19 Current cancer biomarkers may be grouped into a variety of categories including proteins, glycoproteins, oncofetal antigens, hormones, receptors, genetic markers, and RNA molecules. 11
Cancer biomarkers are also classified into prediction, detection, diagnostic, prognostic, and pharmacodynamics biomarkers. 20 Prognostic biomarkers are based on the distinguishing features between benign and malignant tumors. Predictive biomarkers (also known as response markers) are used exclusively in assessing the effect of administering a specific drug, thus, allowing clinicians to select a set of chemotherapeutic agents, which will work best for an individual patient. Pharmacodynamic biomarkers are cancer markers utilized in selecting doses of chemotherapeutic agents in a given set of tumor-patient conditions. Diagnostic markers may be present in any stage during cancer development.
HIV-associated Kaposi Sarcoma and its Problems in Diagnosis
Kaposi sarcoma (KS) is an endothelial neoplasia that is found typically in cutaneous lesions, whose development stages entail macules, plaques, and nodules. 21 KS is the most common malignancy in HIV patients. HIV-associated Kaposi sarcoma (HIV-KS) is a low-grade vascular tumor associated with human herpesvirus 8 (HHV8)/KS-associated herpes virus infection and is the most aggressive and frequent type of KS.22,23 KS primarily involves the skin but can also involve the viscera. 24 Multiple mucocutaneous lesions typically evolve from flat macule (early or patch stage) into plaques (plaque stage) and then nodules (tumor or nodular stage) containing spindle-shaped tumor cells. KS has a variable clinical course, ranging from minimal disease presenting as an incidental finding to a rapidly progressing neoplasm that can result in significant morbidity and mortality, depending on the specific site of involvement.
It poses problems in histologic diagnosis due to its broad morphologic spectrum and mimicry of many benign vasoproliferative lesions and tumors with a prominent spindle component. 25 Distinguishing KS from other benign or malignant vascular tumors, as well as other nonvascular spindle cell soft tissue neoplasms, can be challenging. 26 Early-stage KS represents a reactive lesion that can either regress or progress. Progression is related to the long-lasting expression of HHV8 latency genes in KS lesions, including latent nuclear antigen-1 (LANA-1), 21 cyclin-D1,27,28 and bcl-2. 29 HHV8-related induction of the receptor tyrosine kinase c-kit was shown by gene expression profiling in cultured endothelial cells to play a key role in KS tumorigenesis.30,31
Biomarkers Used in HIV-KS Diagnosis/Prognosis
The differential diagnosis of KS may include cutaneous angiosarcoma, spindle cell hemangioma, dermatofibrosarcoma protuberans, vascular transformation of lymph nodes, pilar leiomyoma, stasis dermatitis, pyogenic granuloma, and spindled melanoma among others (Table 1). 26 Histologically, all epidemiologic forms of KS are characterized by the progressive proliferation of spindle-shaped cells and are associated with KSHV/HHV8. 32 Thus, immunohistochemical detection of HHV8 in fixed tissues would be diagnostically useful, enabling one to differentiate KS from other entities. In latency, HHV8 genes produce numerous proteins that induce or maintain KS lesions, including K12, K13/viral FADD-like interferon converting enzyme inhibitory protein (vFLIP), vCyclin, and the LANA-1 that modulates cellular transcription.33–35
Summary of current biomarkers in HIV-KS.
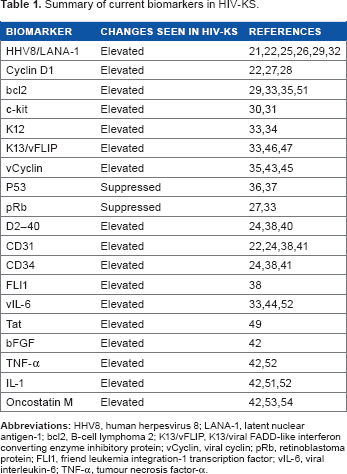
HHV8 LANA-1 is a protein encoded by open reading frame-73 (ORF73) of the virus’ genome. The protein is expressed predominantly during viral latency and appears to play a role in viral integration into the host genome. It has also been shown to interfere in apoptosis via interactions with p53. 36 LANA-1 protein may cause dysfunction of cell cycle regulatory checkpoints by degrading p53 and inactivating pRb. 37 It has been previously shown that positive immunostaining for HHV8 LANA-1 exhibits high sensitivity and specificity, and it is a reliable and cost-effective method for the diagnosis of KS and is also useful for distinguishing it from the mimickers.21,25,29
Recently, it has been reported that immunohistochemical staining with D2-40, CD31 (a platelet/endothelial cell adhesion molecule, PECAM1), CD34 (a hematopoietic progenitor cell surface protein), and FLI1 (Friend leukemia virus integration 1) is useful for distinguishing cutaneous KS from other diseases.24,38 D2-40 is a novel monoclonal antibody, directed against Mr 40000 O-linked sialoglycoprotein, which reacts with a fixation resistant epitope on the lymphatic endothelium. 39 It is considered to be a selective marker of lymphatic endothelium. 40 Monoclonal antibodies directed against CD31 and CD34 are sensitive and specific markers of endothelial differentiation that are expressed by the majority of vascular tumors. It has been previously demonstrated that immunostaining for CD31 and CD34 can be used as an aid in KS diagnosis in routinely processed tissues. 41 In a study by Rosado and colleagues, it was reported that CD31, CD34, D2-40, and FLU markers demonstrated high sensitivity in both AIDS-related and non-AIDS-related KS as well as in stages of tumor progression. 38
A number of inflammatory cytokines, peptide growth factors, HIV encoded Tat protein, and KSHV/HHV8 gene products contribute to KS cell growth and development. 42 HHV8 antigens target cell signaling pathways and deregulate apoptosis and immune response through vCyclin, vFLIP, bcl-2 oncogene, viral interferon regulating factor, and vIL-6.33,43–47 The alterations of immune cells (lymphocytes, monocytes, histiocytes, and dendritic cells) have been suggested to play a role in the neoplastic process. 48 Immune activation can cooperate with some growth factors and HIV-1 Tat protein in the development and progression of KS. 49 HIV-KS cells have been shown to produce angiogenic growth factors and cytokines such as fibroblast growth factors (FGFs), tumor necrosis factor-α (TNF-α), interleukin 1 (IL-1), IL-6, Tat, and oncostatin M, and express high affinity receptors for several cytokines.50,51 Elevated levels of IL-1, IL-6, and TNF-α have been reported in patients with HIV-KS. 52
Oncostatin M, a cytokine produced by microphages and activated T-lymphocytes, has been shown to be a mitogen for HIV-KS derived spindle cells. 53 Oncostatin M appears to be a major cytokine responsible for maintaining the long-term growth of HIV-KS in cell cultures. 54 In addition, inflammatory cytokines induce the production of a potent autocrine growth factor for spindle cells known as basic fibroblast growth factor (bFGF). The autologous production of bFGF is an important stage in KS tumorigenesis since antisense bFGF or anti bFGF antibodies interfere in KS cell growth in tissue culture. 42 It has been shown that oncostatin M, IL-1, and TNF-α induce KS cell growth by inducing the expression of various bFGF isoforms.
HIV-associated NHL and its Problems in Diagnosis
NHL refers to a heterogeneous group of hematopoietic malignancies originating in the lymphocytes.55–57 The majority of NHL cases (85–90%) arises from B-cell progenitors and develops into the various entities largely grouped into low, intermediate, and high-grade NHL based on the treated natural history and survival patterns. 58 NHL comprises many subtypes, each with distinct epidemiology, etiology, and features (ie, morphology, immunophenotype, and clinical manifestations).59,60 Epstein–Barr virus (EBV) has been implicated in the development of many NHL subtypes in HIV-infected individuals. 61 NHL is the second most common malignancy in HIV-infected patients, with diffuse large B-cell lymphoma (DLBCL) as the most common subtype of HIV-associated NHL (HIV-NHL) followed by Burkitt's lymphoma (BL). 62
DLBCLs are heterogeneous diseases that differ in nature of the genetic abnormalities, morphologic appearance, clinical features, and patients respond differently to treatment and vary in prognosis.63,64 Most DLBCLs are thought to arise from normal antigen exposed B-cells that have migrated to or through germinal centers. 65 Gene expression profiling has identified two broad subgroups: those of germinal center origin, known as germinal centre B-cell like (GCB) lymphomas (typically CD10+ and BCL6+); and those arising from cells resembling activated B-cells (non-GCB) (typically IRF4/MUM-1+/– and CD13+).56,66 It has been shown that patients with GCB DLBCL have a better progression free and overall survival than those with non-GCB DLBCL, irrespective of the international prognostic index (IPI) score.67–71 Therefore, the subclassifications of DLBCL into GCB and non-GCB may serve as important predictive prognostic factors. BL is an aggressive form of NHL derived from germinal center B-cells. 72 HIV-associated BL is characterized by cMYC translocations and overexpression; 73 however, EBV infection is not necessarily a precursor to transformation. 74 NHL is a very complex malignancy consisting of several types that are also divided into subclasses that differ in treatment response and prognosis. This may pose problems in the initial diagnosis of NHL. Biomarkers are necessary in the initial evaluation of the patients with newly diagnosed NHL, which must establish the precise histologic subtype, the extent, and site of disease (localized or advanced, nodal or extranodal). This is important in the determination of treatment approach and predicting the response to chemotherapy.
Biomarkers Used in HIV-NHL Diagnosis/Prognosis
The first step in the diagnosis of NHL is to obtain good quality and adequate sample of tissue by excisional biopsy of an affected lymph node or other mass lesion for assessment of cellular morphology and nodal architecture (Table 2).75–77 After the initial tissue biopsy provides a diagnosis of NHL, the following laboratory tests are performed: complete blood count, white blood cell differential, platelet count, and examination of the peripheral smear for the presence of atypical cells, suggesting peripheral blood and bone marrow involvement; biochemical tests including blood urea nitrogen (BUN), creatinine, alkaline phosphatase, aspartate aminotransferase (AST), alanine aminotransferase (ALT), lactate dehydrogenase (LDH), and albumin; serum calcium, electrolytes, and uric acid; serum protein electrophoresis; HIV, hepatitis B, and C serology; and beta-2 microglobulin levels (in patients with indolent lymphomas). 78
Summary of current biomarkers in HIV-NHL.
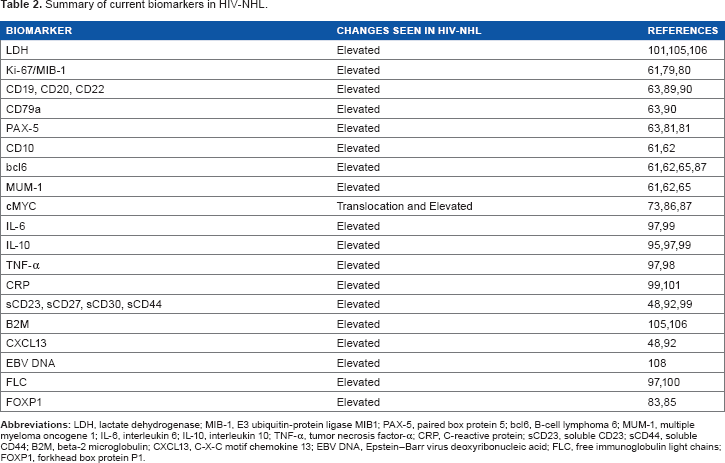
This is followed by pathological evaluations, which include flow cytometry or immunohistochemical staining for immunophenotype. 75 For aggressive lymphomas, this includes evaluation of proliferative fraction using Ki-67 or MIB-1 staining as a more aggressive regimen may be indicated for high growth fraction tumors. 77 The expression of Ki-67 has been associated with poor outcome and survival in DLBCL patients.79,80 Immunophenotypic expression patterns of DLBCL include positivity for various pan B-cell markers such as CD19, CD20, CD22, CD79a, PAX-5, and demonstration of immunoglobulin surface light chain restriction by flow cytometry in the majority of cases. 63 The presence of positive PAX-5 immunostaining has been strongly associated with B-cell differentiation as PAX-5 is a B-cell restricted transcription factor.81,82 Staining for CD10, bcl-6, and MUM-1 are usually routinely performed in order to distinguish GCB from non-GCB DLBCL.
Fork box protein P1 (FOXP1), an essential transcription regulator of B-cell development, has been shown to be overexpressed in non-GCB DLBCL as compared with GCB DLBCL.71,83,84 FOXP1 has also been associated with poor survival and prognosis. 85 It is now recognized that FOXP1 may serve as an additional biomarker for distinguishing non-GCB from GCB DLBCL and should be included in the diagnosis/prognosis of DLBCL. In addition, fluorescence in situ hybridization (FISH) analysis for cMYC is performed as translocations involving the cMYC occurs in 10–15% of DLBCL lymphomas and is associated with a worse outcome. 86 MYC translocations confers a worse prognosis in patients treated with cyclophosphamide, hydroxydaunorubicin, Oncovin, and prednisone (CHOP), and CHOP plus rituximab (R-CHOP) regimens. 87 BL expresses agerminal center B-cell phenotype, 88 and the immunophenotypic expression include B-cell antigens CD19, CD20, CD22, CD79a, and PAX-5 along with CD10, bcl-6, CD77, Ki-67 or MIB-1 and monotypic surface light chains such as IgM. 89 BL also expresses CD43, TCL1, and CD38 but is negative for CD5, CD23, CD44, CD138, CD34, and TdT.90,91
Altered immune mechanisms play a critical role in the pathogenesis of NHL, as evidenced by increased rates of NHL among HIV-positive patients, transplant recipients, and autoimmune disease patients.92,93 A marked increase in B-cell activation is commonly seen in HIV infection, which is driven by the overproduction of B-cell stimulatory cytokines, such as IL-6 and IL-10, as well as by stimulation of B-cells by HIV and other microbial antigens. 94 In addition, HIV itself induces the production of inflammatory cytokines that cause B-cell stimulation, proliferation, and activation, and the cell lines derived from HIV-NHL have been found to express cytokines including interleukin 6, 10, and tumor necrosis factor-α.95–98 B-cell activation is characterized by lymphocyte proliferation, class switch recombination (CSR), and somatic hypermutation, all of which are prone to resultant errors in DNA that may lead to lymphomagenesis. B-cell activation leads to the expression of activation induced cytidine deaminase (AICDA), a DNA modifying enzyme that mediates immunoglobulin gene CSR and somatic hypermutation. 99
Various factors associated with B-cell activation, including B-cell stimulatory cytokines, as well as soluble serum molecules that are associated with B-cell activation, including serum immunoglobulins (Ig) and Ig components such as free light chains, have been seen to be elevated preceding the appearance of HIV-NHL.99,100 In a nested case–control study by Breen and colleagues, it was shown that serum levels of molecules associated with B-cell activation including IL-6, IL-10, C-reactive protein (CRP), sCD23, sCD27, and sCD30 are elevated for several years preceding the diagnosis of systemic HIV-NHL.99,101 In addition, De Roos and colleagues, in a case–control study within Women's Health Initiative study cohort of 491 cases and 491 controls, showed that women with high serum levels of soluble sCD23, sCD27, sCD30, sCD44, and CXCL13 biomarkers were at 2.8- to 5.5-fold increased risk of B-NHL. 92 Furthermore, this was confirmed by Hussain and colleagues, in a nested case–control study of 3768 women, where it was shown that elevated levels of sCD27, sCD30, CD23, and CXCL13 were associated with subsequent diagnosis of HIV-NHL. 48
Factors associated with poor clinical outcome and shorter survival in patients with HIV-NHL include CD4 cell count <100 mm3, advanced stage disease (III or IV), age over 35 years, history of injection drug use, elevated serum LDH (above normal), Eastern Co-operative Oncology Group performance status (ECOG PS) of more than 2, and the involvement of more than 2 extranodal sites.102–106 Matthews and colleagues, in a cohort of 7840 HIV-positive patients, showed that age, nadir CD4 cell count, and no prior cART are significantly associated with the development of systemic NHL. 107 In addition, Tedeschi and colleagues showed that low CD4 and CD8 cell count and detectable EBV viremia are three independent prognostic biomarkers that might help in the management of HIV-NHL patients. 108 Furthermore, higher HIV viral load accompanied by lower CD4 count have been associated with the development of HIV-NHL.109,110 It has been shown that the risk of HIV-NHL rises substantially in patients with HIV RNA levels greater than 100 000 copies/μL and those with CD4 lymphocyte counts of less than 50 mm3/μL. 111
HIV-associated Cervical Cancer and its Problems in Diagnosis
Human papillomavirus (HPV) infection is the most important cause of cervical cancer; however, only 2% of cervical HPV will develop into cervical cancer. 112 Cervical cancer is caused by a persistent infection with high-risk human papillomavirus (hrHPV) types, which lead to premalignant precursor lesions known as cervical intraepithelial neoplasia (CIN). 113 The most common histologic types of cervical cancer are squamous cell (69%) and adenocarcinoma (25%). 114 CIN is characterized by abnormal cellular proliferation, maturation, and nuclear atypia. 115 CIN may regress to normal or progress to invasive cervical cancer if left untreated. Approximately, one-third to one half of the cases of CIN I and CIN II regress without treatment. However, the more severe the abnormality of the lesion, the less likely it is to regress. The accurate grading of CIN lesions is important for clinical management of patients, because CIN I and CIN II/III lesions are treated differently and inaccurate grading results in over or under treatment. This emphasizes the need for specific biomarkers to aid objective CIN grading and to achieve more accurate diagnosis.
Biomarkers Used in HIV-associated Cervical Cancer Diagnosis/Prognosis
The detection of HPV DNA in cervical cancer has been proven to be a good diagnostic and risk predictor tool for cervical cancer (Table 3). 116 The oncogenic process in cervical cancer is initiated and mediated by the upregulation of HPV E6/E7 oncoproteins, and thus, overexpression of these oncoproteins is a marker for an increased risk of cervical cancer.117–119 The hrHPV subtypes such as 16 and 18 are thought to play a role in malignant transformation of cells by producing E6 and E7 viral regulatory proteins. 33 E6 and E7 are involved in cell proliferation and survival. HPV and oncogene E6 and E7 expressions are the most important markers implicated for cervical cancer. 20 Some studies suggest that HPV oncogenes E6 and E7 mRNA levels in the uterine cervix may be more specific early indicators of predisposition to carcinogenesis than DNA levels. 120
Summary of current biomarkers in HIV-associated cervical cancer.
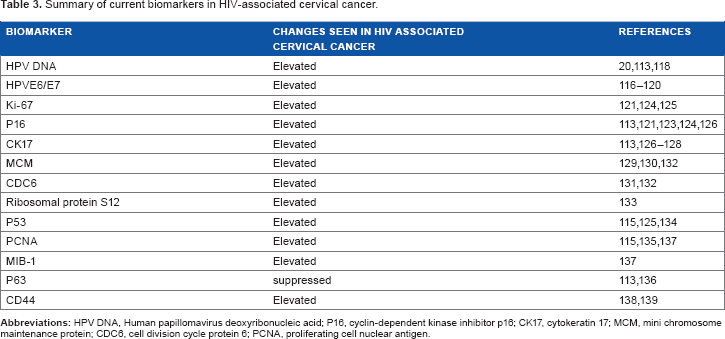
Ki-67 is a well-known cell proliferation marker, useful for confirmation of the diagnosis in ambiguous cases of cervical cancer and CIN grading. 121 Ki-67 detects a nuclear antigen that is present only in proliferating cells but absent in resting cells. 122 Ki-67 has been found to be more intensely stained in HPV-positive than HPV-negative epithelium. P16INK4A (p16) is a cyclin-dependent kinase (cdk) inhibitor that functions as a specific biomarker used for identification of squamous and glandular dysplastic cervical epithelium with tendency to invasive cervical cancer. It has been suggested that p16 is overexpressed in cervical epithelial cells that are transformed in response to the expression of the hrHPV E7 oncoprotein. 113 In a nested study by Carozzi and colleagues, it was shown that p16 overexpression is a marker for CIN2 or worse or for its development within 3 years in HPV-positive women. 123 Ki-67 and p16 are complimentary alternative biomarkers for HPV-related neoplasia.124,125 Cytokeratin (CK) 17 is a useful marker for endocervical reserve stem cells, which gives rise to metaplasia and antibody to CK17 is used to differentiate between immature squamous metaplasia and high-grade CIN (CIN III). 126 CK17 is specific for reserve cells and immature metaplastic cells; it is not expressed in cervical glandular epithelial cells, squamous cells, or mature squamous metaplastic cells.127,128
Overexpression of mini chromosome maintenance (MCM) proteins is seen in severe dysplastic lesions,129,130 and overexpressed cell division cycle protein 6 (CDC6) is observed in malignant cervical cancer.131,132 The ribosomal protein S12 gene has also been reported as an early molecular diagnostic identifier for the screening of cervical cancer and is a potential target in cancer gene therapy trials.122,133 Tumor suppressor protein p53 is a nuclear phosphoprotein encoded by the p53 gene, whose normal function is to control cell proliferation and apoptosis. Mutations of the p53 gene are frequently found in most invasive cancer, resulting in loss of tumor suppressor functions of wild type p53 and gain of oncogenic functions. Overexpression of p53 has been suggested to be a possible prognostic marker for cervical cancer. 134 Madhumati and colleagues showed that proliferating cell nuclear antigen (PCNA) and P53 expression increases with increasing severity of CIN lesions. 115 It has been previously shown that upregulation of PCNA is closely associated with hrHPV and progressive CIN, but does not predict outcome in cervical cancer. 135 P63, which is a member of the p53 gene family, is expressed in the basal and parabasal cells of mature cervical, vaginal, and vulval squamous epithelium, and also in cervical reserve cells at the transformation zone.113,136 It has been shown that MIB-1 may be a useful marker for identification of low-grade CIN lesion with high proliferative index. 137 CD44 is a cell adhesion molecule that has been reported to be correlated with poor prognosis in invasive cervical cancer.122,138,139 The increased serum CD4+ and CD8+ T-cell levels and the presence of large number of natural killer (NK) cells have been associated with a favorable response in patients with cervical cancer treated with neo-adjuvant chemotherapy.
Discussion/Conclusion
Cancer biomarkers offer a great potential for improving the management of cancer at every point from screening and detection, diagnosis, staging, prognosis, and assessment of treatment response. 20 Biomarkers offer the hope of early detection as well as tracking cancer progression and recurrence. 66 Early detection may help improve survival of HIV-positive cancer patients, as it could help identify HIV-positive individuals at most risk of cancer development distinguish aggressive from indolent malignancies and track disease progression.
Discovery of new biomarkers suitable for clinical application may aid the diagnosis and classification of cancer, which in turn, should lead to better patient stratification. 140 Biomarkers do not need to be cancer specific to be useful; certain proteins may help predict response to therapy or aid in the monitoring of disease progression. 141 As cancer is increasingly defined by dysregulated pathways, relevant biomarkers may cut across tumor types without showing tissue specificity. Abundance of potential cancer biomarkers have been discovered, however, only few of them have been integrated into clinical practice. This is due to the fact that some of these biomarkers are not highly sensitive and specific for cancer detection. It is well recognized that the road from biomarker discovery, validation, and regulatory approval to the translation into clinical setting could be long and difficult. 11
A new era is underway in which cancer detection, diagnosis, and treatment will be guided increasingly by the molecular attributes of the individual patient. 142 The future of cancer therapy lies in the use of biomarkers that offer the potential to identify and treat cancer years before it is either visible or symptomatic. In addition, the future of cancer management is expected to be profoundly dependent upon the use of biomarkers that will guide physicians at every step of disease management. 143 Cancer biomarkers can be used for the accurate evaluation and management of the disease.
Author Contributions
Conceived and designed the experiments: BF, GS, PB, BR. Analyzed the data: BF, GS, PB, BR. Wrote the first draft of the manuscript: BF. Contributed to the writing of the manuscript: BF, GS, PB, BR. Agree with manuscript results and conclusions: BF, GS, PB, BR. Jointly developed the structure and arguments for the paper: BF, GS, PB, BR. Made critical revisions and approved final version: BF, GS, PB, BR. All authors reviewed and approved of the final manuscript.