
Abstract
Chelation therapy has been the major treatment for heavy metal poisoning. Various chelating agents have been developed and tested for treatment of heavy metal intoxications, including mercury poisoning. It has been clearly shown that chelating agents could rescue the toxicity caused by heavy metal intoxication, but the potential preventive role of chelating agents against heavy metal poisoning has not been explored much. Recent paper by Siddiqi and colleagues has suggested a protective role of chelating agents against mercury poisoning, which provides a promising research direction for broader application of chelation therapy in prevention and treatment of mercury poisoning.
Mercury poisoning, also referred to as hydrargaria, usually results from exposure to mercury-containing substance, such as mercury, mercury salts and organomercury compounds.
Mercury exists in several oxidation states: metallic (Hg0), mercurous (Hg+) and mercuric (Hg2+). 1 All forms exert toxic effects to a variety of organs of humans, including the kidneys, the central nervous system, gastrointestinal tract, and endocrine system, etc. 2 The toxicity of mercury is mainly mediated through their interaction with the reduced sulfur of free thiol containing molecules such as glutathione, metallothionein and proteins containing free cysteines. 3 The depletion of free thiol also results in the increase of oxidative stress with enhanced formation of hydrogen peroxide and other reactive oxygen species (ROS). Both metallic mercury vapor and oraganomercury compounds are lipophilic and can penetrate cellular membrane easily and therefore, deposit into various organs. 4 Moreover, they can penetrate blood-brain barrier and placenta barrier and result in neurotoxicity and fetotoxicity. Compared to metallic mercury vapor and organomercury compounds, inorganic mercury salts are relatively poorly absorbed. 5 Inorganic mercury salts are mainly absorbed through the intestines and deposited in the kidney.
Chelation therapy refers to the treatment of human heavy metal intoxications with the administration of chelating agents, which forms a stable complex with the toxic heavy metal species and prevents them from attacking biological targets. The first example of chelation therapy dates back to 1941 when Kety et al tried to use sodium citrate to treat lead poisoning. 6 After that, more effective heavy metal chelating agents have been developed for detoxification of heavy metal poisoning. For example, synthetic amino acids containing no mercaptans such as ethylenediamine tetraacetic acid (EDTA), ethylene glycol tetraacetic acid(EGTA)and aminophenoxyethane-tetraacetic acid (BAPTA) as well as thiol-containing chelating agents such as 2,3-dimercaprol, also known as the British Anti Lewisite (BAL); meso 2,3-dimercaptosuccinic acid (DMSA) and its derivatives monoisoamyl DMSA (MiADMSA), monomethyl DMSA (MmDMSA) and monocyclohexyl DMSA (MchDMSA); 2,3-dimercapto-1-propanesulfonic acid (DMPS) (Fig. 1).7–11
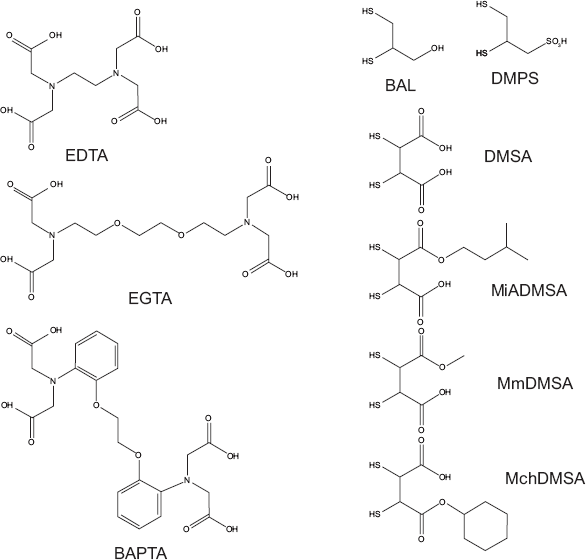
Common heavy metal chelating agents.
Extensive studies have shown that oral or parenteral administration of heavy metal chelating agents such as DMPS and DMSA after mercury intoxication reduces mercury deposition and retention in various organs and increases the urinary excretion of mercury.12–16 Data collected from experimental animals and limited human case suggests that DMPS is among the most efficient and safest heavy metal chelating agents for inorganic mercury compounds, including metallic mercury and mercury salts while DMSA works better for detoxification of organic mercury compounds.16–17
However, the potential preventive role of heavy metal chelating agents against mercury intoxication has not been explored much. In the paper entitled “Renal Toxicity of Mercuric Chloride at Different Time Intervals in Rats” published in this issue of Biochemistry Insights, Siddiqi and colleagues reported that administration of DMPS before HgCl2 treatment protects the rats from the acute renal damages caused by HgCl2. 18 The authors characterized in detail the renal toxicity of HgCl2 administration in rats after one or two days, demonstrating that HgCl2 administration results in renal damages, causing decrease of urinary volume and glomerular filtration rate, decrease of urinary excretion of urea and creatinine as well as increase of urinary excretion of protein, albumin and γ-glutamyltransferase. The pre-treatment of rats with DMPS before mercury intoxication by HgCl2 significantly maintains the urine biochemical indices at close to normal values and minimizes the histological damage, indicating protection of rats from HgCl2-induced renal damage by DMPS pre-treatment.
Interestingly, an earlier paper by the same group showed that pre-treatment of DMPS does not protect the rats against the collagen damages induced by HgCl2, which are reflected by elevated serum hydroxyproline and elevated excretion of hydroxyproline in urine. 19 The elevated hydroxyproline level mainly results from the secondary effect of mercury poisoning, namely, production of ROS induced by depletion of thiol-containing reducing agents. It seems that addition of thiol-containing chelating agent such as DMPS deprives mercury species of their targets to restore the target molecules’ free thiol groups for their proper functions, but cannot provide enough reducing capacity at the level administrated to reverse the hydroxylation of prolines by ROS. Therefore, administration of DMPS together with the antioxidant treatment might be beneficial for protection and treatment of mercury poisoning.
Disclosures
The authors report no conflicts of interest.