
Abstract
Breast cancer is the most common cancer worldwide with significant global burden. Insulin-like growth factor 1 (IGF1) is an important regulator of cellular growth, differentiation, and apoptosis and mitogenic and antiapoptotic activities. Some studies suggested an association between cytosine adenine (CA) repeats gene polymorphisms of IGF1 and the risk of developing breast cancer while other studies did not find such an association. This study aims investigate the role of IGF1 (CA) repeats gene polymorphisms in the risk of developing breast cancer among Omani women.
Methods
We analyzed (CA) repeats gene polymorphisms of IGF1 by extraction of genomic DNA from the peripheral blood of 147 patients with breast cancer and 134 control participants and performed genotyping using DNA sequencing.
Results
Approximately 46% of patients carried the IGF (CA)19 repeat allele, with 31.3% carrying two copies of this allele and 50% of controls carried the IGF (CA)19 repeat allele with 30.1% carrying two copies of this allele. The difference of the IGF CA repeat groups was significant between cases and controls with (
Conclusion
Overall there was no association between the IGF (CA)19 repeat and breast cancer in Omani females.
Introduction
Breast cancer is the most common malignancy in women throughout the world. 1 It accounts for 18% of all female cancers and approximately 600,000 annual deaths worldwide.1,2 Among Omani women, breast cancer is the most common cancer accounting for one in every five new cancer cases detected among females, with an age standardization incidence rate (ASR) of 21.3 per 100,000.3,4 Even though the incidence is increasing in Oman, it remains low compared to western countries, but is consistent with other Asian countries.3,5 However, cases of breast cancer in Oman often present in advanced stages with poor prognostic features, as well as poor differentiation and prevalence of estrogen and progesterone receptor-negative and Her-2/neu positive tumors. 6
Insulin-like growth factor 1 (IGF1) is part of a large family of peptide hormones including insulin and IGF2 and it is located in chromosome 12q22-q24. IGF1 is composed of 70 amino acids spanning 100 kilobase (kb) pairs long with 6 exons. 7 IGF1 is an important regulator of cellular growth, differentiation, and apoptosis in combination with growth hormone (GH), insulin, and sex steroids. It exhibits strong mitogenic and antiapoptotic activity on breast cancer cells and acts synergistically with estrogen to enhance breast cancer growth.8–10 IGF1 is regulated by GH and is secreted mainly from the liver. Breast tissue secretes IGF1 from the mammary connective tissue and from adipocytes for their differentiation. 11
Short tandem repeats (STRs) are repeated DNA sequences of 1–6 base pairs and up to <60 bp in total length. 12 STRs are highly polymorphic and distributed throughout the mammalian genome. 12 In the 5′ untranslated region of the IGF1 gene, a polymorphic sequence consisting of multiple cytosine adenine dinucleotides (CA) is located 1 kb upstream from the transcription site. The number of CA repeats ranges from 10–24, with the most common allele containing 19 CA repeats. 10
Recent studies have examined CA repeat polymorphisms in the IGF1 gene because of its proximity to the promoter region, 1 kb upstream from the transcription start site. Polymorphisms are associated with IGF1 levels. 10 A functional relationship was found between this type of polymorphism and the circulating levels of IGF1. People with the 192 bp allele (19 repeats) or 194 (20 repeats) have higher levels of IGF1 than non-carriers of these alleles. 13 Moreover, some studies have shown an association between increased levels of IGF and increased cancer risk.14,15 In contrast, a study conducted in the Netherlands concluded that people with (CA)19 repeats have lower levels of IGF1, particularly among postmenopausal women, suggesting that this polymorphism is not associated with breast cancer. 11 Another study showed that the breast cancer risk is higher among people with fewer than (CA)19 repeats and the association is strong among premenopausal women. 8 In the same study, there was increased breast cancer risk among postmenopausal women who lacked (CA)19 repeats, in particular in those with lower body mass index (BMI). 8
However, no study so far has been carried out in Oman or Arab World to evaluate the relationship between IGF1 (CA)n repeats and breast cancer risk. This study is of particular significance, given the high rate of obesity and metabolic syndrome (MS) in Oman, and the association of increased circulating IGF1 influencing the predisposition to obesity-related diseases including cancer. In Oman, the crude prevalence of MS was (17.0%) and the overall age-adjusted prevalence was (21.0%), among women the ASR was (23.0%). 16
The aim of this study was to investigate the role of IGF1 and the CA repeat gene polymorphism in the risk of developing breast cancer among Omani women.
Materials and Methods
Study participants
A hospital based case-control design was used to evaluate the association between CA repeats and the risk of developing breast cancer. Breast cancer cases (old and newly diagnosed) were histologically confirmed at the two main teaching hospitals of Sultanate of Oman. Sultan Qaboos University Hospital and the Royal hospital were included in this study from January–September 2010. Control subjects were enrolled from health workers, the blood bank, and the community. Controls were recruited from women who did not have any history of benign breast disease, neoplastic disease, or other major health problems. The controls were not matched to specific cases, but age distributions of the case and control groups were stratified.
The Medical Research and Ethics Committee of the College of Medicine and Health Sciences, Sultan Qaboos University approved the study and all subjects gave their informed consent prior to participating and in accordance with the Helsinki Declaration.
Sample size was estimated using the equation below with 95% confidence and a total of 320 case-control subjects are needed (considering 12.9) 17 of the controls are exposed to (CA non carrier –19/–19) and to have 80% chance of detecting an odds ratio of 3.31. 18

Genetic analysis
The genetic analysis was carried out in line with previously described methodology described by Cleveland et al 10 and briefly, EDTA- preserved blood samples were collected for both cases and controls. The blood samples were frozen at -80 °C until DNA was isolated by extraction using either QIAamp or Gentra method. The number of the CA repeats in the blood samples was assessed using fragment analysis. IGF1 microsatellites (CA) were located 1,000 bp upstream of the transcription site or promoter site and the expected size of polymerase chain reaction (PCR) product was approximately 192 bp, depending on the number of repeats. PCR primer used was: Forward, 5′-GCTAGCCAGCTGGTGTTATT-3′ and Reverse, 5′-ACCACTCTGGGAGAAGGGTA-3′). PCR was performed as follows: one cycle of 5 min at 94 °C, 30 temperature cycles consisting of 1 min at 94 °C, 1 min at 59 °C and 1 min at 72 °C. The final extension was done at 72 °C for 10 min. The PCR amplified products were mixed with 0.7 μL of ROX internal standard (size of 500 bp), 12 μL of form amide and 1 μL of PCR product (the forward primer already labeled with Hex fluorescence). ABI 3130 × 1 sequencer and was used to measure the size (ranged from 174 to 198 bp according to number of CA repeats), and intensity fluorescent products following denaturing for 5 min at 95 °C. In each run, the homozygous allele was tested again using sequencing to confirm the size obtained by the fragment analysis and used as a control for the other samples in the same run.
Statistical analysis
Data were analyzed using SPSS for Windows version 16.0 (SPSS Inc., Chicago, Illinois). Statistical tests were two sided and the level of significance was set at α = 0.05. The difference of the allelic distribution of the IGF1 CA repeats between cases and controls were examined using chi-squared contingency test. In this study, the IGF1 genotypes were divided into five groups according to classification used by Cleveland et al 8 that included as cited in their paper and shown in Table 5.
Unconditional logistic regression method was used to assess the relationship between breast cancer risk predisposition and IGF1 genotype with consideration of the pathological features and menopausal status. The odds ratios were estimated adjusting for age and their 95% confidence intervals were also determined under this model. The goodness of fit of the model was tested using Hosmer and Lemeshow test. 19
Results
A total of 147 patients with breast cancer and 134 control participants were included in the final analysis of study where analytical assays worked. The percentages for successful analysis were 84.5% and 88.6% for patients and control subjects respectively. Table1 show all the clinical-pathological features of breast cancer patients considered in this study. The mean age of the patients was 48.0 (±8.24) years, compared to the controls 45.0 (±8.22) years. Table1 demonstrates that 57.4% of cases developed a lesion in the left breast while 42.6% had cancer in the right breast. A majority of the patients (80.1%) presented with a lump, 4.3% with nipple discharge, 4.3% with both nipple discharge and lump, 1.4% with nipple inversion, 1.4% with change in size or shape of the breast, 1.4% with both nipple inversion and lump, 0.7% with skin dimpling, and 6.4% without any symptoms other than pain or upon discovery of cancer by chance or by mammogram regular check. Out of these patients, 73.3% had surgery, chemotherapy, and radiotherapy, while 7.4% had surgery and chemotherapy, 7.4% had both surgery and radiotherapy, 6.7% had only surgery, and 3.0% only chemotherapy. The type of breast cancer among the majority of patients was invasive ductal carcinoma with 87.9%, followed by invasive lobular carcinoma and only few cases with other types. Out of all patients, the dominant grade was high grade 54.2%, with 70.0% involving lymph node metastasis, and 35.6% had distant metastasis. Estrogen and progesterone receptors were with 55.6% and 61.1% negative, respectively; while 54.7% were HER2 receptor positive.
Clinico-pathological features of breast cancer patients.

Number of patients where information is available.
IGF1 genotype and breast cancer risk
The distribution of IGF1 alleles is shown in Table 2. Alleles ranged from (CA)10 to (CA)22 with 174– 198 bp in size. Approximately 46% of the cases carried the (CA)19 repeat allele with 31.3% carrying two copies of this allele and 50.74% of controls carried the (CA)19 repeat allele with 30.1% carrying two copies of this allele, followed by (CA)18, and (CA)20. The difference in the percentage distributions of the CA groups between the cases and controls was statistically significant (
Allelic frequencies of IGF1 (CA)n genotype in study population.

Table3 shows the distribution of IGF1 alleles in cases and controls according to the premenopausal and postmenopausal status of the women. In both premenopausal and postmenopausal case-control subjects, the (CA)19 allele was the most common allele and (CA)18 was the second most frequent, followed by (CA)20. The difference in cases and controls was significant among postmenopausal women (
Allelic distribution of IGF1 (CA)n genotype in study population.

Combined analysis of IGF1 genotype and breast cancer clinico-pathological features
After adjusting the most significant risk factors (family history of breast cancer, previous breast surgery, age at menarche, and use of contraceptives), the participants were classified into five groups based on Cleveland et al 8 classification as shown in Table 4. There was no significant association with breast cancer in all the five groups as shown in Table 4. Even though, the two populations are different but the distribution of the allelic frequencies of CA repeats is similar so we adopted the same classification as Cleveland's study.
Odds ratio (OR) and 95% confidence interval (CI) for IGF1 (CA)n genotype among pre and postmenopausal Omani women using unconditional logistic regression method.

Adjusted for family history of breast cancer, previous surgery, contraceptives
both alleles > (CA)19 repeats
both alleles < (CA)19 repeats
number of CA repeats from both alleles added together.
Comparison of IGF1 genotypes and the pathological features of breast cancer.
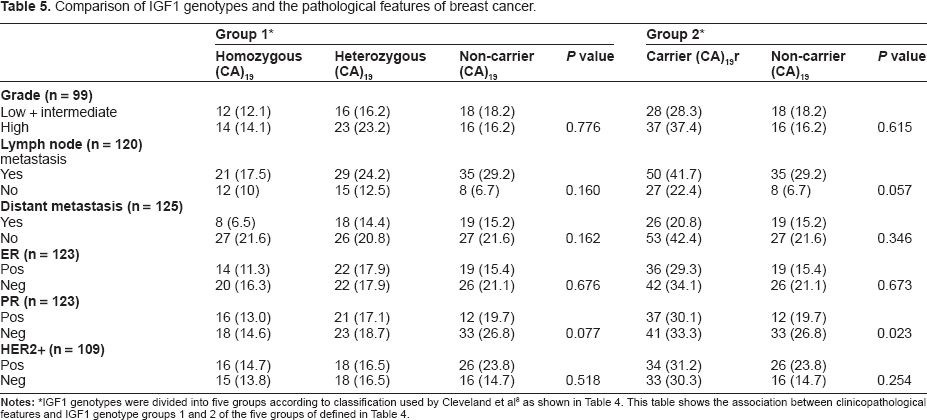
IGF1 genotypes were divided into five groups according to classification used by Cleveland et al 8 as shown in Table 4. This table shows the association between clinicopathological features and IGF1 genotype groups 1 and 2 of the five groups of defined in Table 4.
We further investigated the relationship of CA repeats (Group 1 and 2) and breast cancer by considering the pathological features of the caner as shown in Table 5. Among group 1 there were no statistically significant associations with breast cancer clinico-pathological features (Type, Grade, Lymph Node Metastasis, Distant Metastasis, ER status, PR status, HER2 status) between cases and controls. However, there was a statistical trend towards association between positive PR among carriers in Group 1 genotype with (OR = 2.444; 95% CI: 0.925–6.279;
Discussion
We examined the association between IGF1 CA repeat polymorphisms and breast cancer in an Omani population where there is high rate of metabolic syndrome. We found that the most frequent allele was (CA)19 with approximately 46% of the cases carried the (CA)19 repeat allele with 31.3% carrying two copies of this allele and 50.74% of controls carried the (CA)19 repeat allele with 30.1% carrying two copies of this allele. In comparison, the allele containing (CA)19 repeats was the most frequent in Chinese population, but with lower frequency rates of 38% in cases and 35% in controls.10,20 A large study in a Caucasian population reported relatively higher occurrence of the most common allele containing (CA)19 repeats with rates of 63% and 65% in cases and controls respectively. 8 The frequency rates of allele containing (CA)19 repeats is similar to those reported in African American observed in a large multiethnic study. 21
We found no association between breast cancer and IGF1 CA repeats genotypes among Omani women. Previously, two studies showed that the (CA)19 allele increases the risk of developing breast cancer.8,20 Other studies found an inverse association between the (CA)19 allele and breast cancer.
11
Some studies found there is no association between IGF1 genotype and breast cancer consistent with the current study.22,23 The reason behind the conflicting results between the studies is still unknown but one explanation could be the variation in the ethnic composition of the study populations. Two other studies showed similar genotype distributions as in our study, and both studies reported no association between (CA)19 repeat genotype and breast cancer.23,24 The association between IGF1 CA repeats and breast cancer is not conclusive, where the true relationship between this polymorphism and the regulation of IGF1 expression is unknown. However, effect of CA repeats may have an effect on the transcription activity of IGF1. Because of the proximity of CA repeats to the IGF1 transcription start site, it is possible that depending on allelic size, transcription may affect IGF1 levels.
8
In vitro studies reported that IGF1 has mitogenic activity for both normal and cancerous breast cells.25,26 Many studies suggest an association between circulating IFG1 and breast cancer risk, with higher levels of IGF1 than controls among premenopausal women.14,15 However, not all studies found that association.27,28 A large collaborative study found that IGF1 and IGFBP3 genes polymorphisms correlated with circulating levels of IGF-I and IGFBP-3, respectively, but did not predict breast cancer predisposition.
29
In contrast, a pooled analysis of data from 17 prospective studies demonstrated that breast cancer risk was associated higher levels of IGF1.
30
However, this study did not correlate the IGF1 serum concentration with IGF1 polymorphisms and there was great variation in concentration of serum IGF1 between the studies reflecting differences in assay methods. In the current study, there was no significant association between breast cancer risk among both pre- or postmenopausal women and the (CA)19 allele even after adjusting for significant risk factors. However, we interestingly found that in postmenopausal group there was a difference in (CA)20 repeat allele between the cases and controls (
In the current study we found a significant association between IGF1 CA repeat genotypes and both PR status and cancer type. (CA)19 carriers are more likely to express progesterone receptors compared to non-carriers [OR 2.482, CI 95%: 1.119–5.503,
In conclusion, the current study has the strength of being the first report from this part of the world that studied the IGF1 repeats in almost 300 individuals and confirmed that the most common allele was (CA)19, in keeping with other ethnic groups. However, we found no association between breast cancer and IGF1 CA repeats genotypes among Omani women in accordance with several large size studies.
Author Contributions
Conceived and designed the experiments: MSM. Analysed the data: KA, SG. Wrote the first draft of the manuscript: KA. Contributed to the writing of the manuscript: SG, MSM. Agree with manuscript results and conclusions: MSM, KA, SG, AA, ZM. Jointly developed the structure and arguments for the paper: MSM, KA, SG. Made critical revisions and approved final version: KA, SG, AA, ZM, MSM. All authors reviewed and approved of the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.
Footnotes
Abbreviations
Acknowledgements
This work would have not been possible without the support of Sultan Qaboos University, particularly the College of Medicine and Health Sciences and Royal Hospital. We would like to thank all the participants, cases and controls, Dr. Hamza Babiker, Mr. Mohammed Al Kindi, and Ms. Hamida Al Barwani for their valuable contributions.