
Abstract
Introduction
Current guidelines recommend completion axillary lymph node dissection (cALND) in case of a sentinel lymph node (SLN) metastasis larger than 0.2 mm. However, in 50%-65% of these patients, the non-SLNs contain no further metastases and cALND provides no benefit. Several nomograms and scoring systems have been suggested to predict the risk of metastases in non-SLNs. We have evaluated the Tenon score.
Patients and Methods
In a retrospective review of the Swedish Sentinel Node Multicentre Cohort Study, risk factors for additional metastases were analysed in 869 SLN-positive patients who underwent cALND, using uni- and multivariate logistic regression models. A receiver operating characteristic (ROC) curve was drawn on the basis of the sensitivity and specificity of the Tenon score, and the area under the curve (AUC) was calculated.
Results
Non-SLN metastases were identified in 270/869 (31.1%) patients. Tumour size and grade, SLN status and ratio between number of positive SLNs and total number of SLNs were significantly associated with non-SLN status in multivariate analyses. The area under the curve for the Tenon score was 0.65 (95% CI 0.61–0.69). In 102 patients with a primary tumour <2 cm, Elston grade 1–2 and SLN metastases ≤2 mm, the risk of non SLN metastasis was less than 10%.
Conclusion
The Tenon score performed inadequately in our material and we could, based on tumour and SLN characteristics, only define a very small group of patients in which negative non-sentinel nodes could be predicted.
Introduction
Sentinel lymph node biopsy (SLNB) has widely replaced conventional axillary lymph node dissection (ALND) as routine axillary staging in breast cancer surgery. The SLNB method is accurate and safe1–4 and conveys substantially less postoperative morbidity than ALND.5,6
Current guidelines recommend completion axillary lymph node dissection (cALND) in case of a sentinel lymph node (SLN) metastasis larger than 0.2 mm. 7 However, in 50%–65% of patients, the non-SLNs contain no further metastases 8 and cALND provides no benefit. In addition, several studies have demonstrated the incidence of regional recurrence to be much lower than expected when axillary surgery was omitted,9–12 and the need for cALND in all SLN-positive patients has been questioned. It remains, though, that even in the case of only SLN isolated tumour cells, the incidence of non-SLN metastases has been reported to be as high as 20%. 13 The benefit of ALND on survival is debated. In a meta-analysis from the pre-SLN era, ALND improved survival, 14 but in some latter, randomized, pre-SLN studies, the survival was similar in the ALND and the no ALND groups.15,16 Giuliano et al 17 reported that SLNB alone does not result in inferior survival in SLN-positive patients, and in a recent review it was concluded that there is a potential role for avoiding ALND in selected SLN-positive patients. 18
Several authors have suggested nomograms and scoring systems to predict the risk of non-SLN metastases, with the aim of aiding in the decision of further surgery.19–25 Validation studies have demonstrated a reasonably accurate predictive ability,26–33 although far from perfect. In a comparison by Coutant et al, the Memorial Sloan-Kettering Cancer Center nomogram and Tenon score outperformed other predictive models. 27 An advantage of the Tenon score is that a fair estimation of all predictive variables can be made perioperatively, allowing the surgeon to decide whether cALND should be performed directly following frozen section of the SLN.
In the present study we evaluated the Tenon score in a large Swedish multicentre SLN cohort.
Patients and Methods
The swedish sentinel node multicentre cohort study
Between September 2000 and January 2004, 3501 women (with 3535 breast tumours) from 25 Swedish hospitals were included in the Swedish Sentinel Node Multicentre Cohort Study. Patients and surgical methods have been described in detail elsewhere. 34 In short, patients with a unifocal, invasive breast cancer less than 3 cm in diameter were eligible for enrolment. Exclusion criteria were palpable regional lymph nodes, neoadjuvant chemo- or radiotherapy, pregnancy, known allergic reactions to blue dye or isotope, previous surgery in the ipsilateral breast, and preoperatively diagnosed tumour multifocality. After enrolment, data sheets were sent to a research unit, where they were computerised. Data sheets included information on primary tumour characteristics, number of sentinel and non-sentinel lymph nodes with and without metastasis, and size of metastasis. The research protocol postulated annual follow-ups with mammography and clinical examination. Incidence of recurrences and survival were prospectively followed up by a research assistant via reports from the participating centres and on-site visits.
The study was approved by the ethics committee of Karolinska Institutet, Stockholm, and each region's local ethics committee. All patients gave written informed consent.
Surgical procedure
After the preoperative sub- or intradermal injection of 40–60 mBq Technetium-99 nanocolloid (Solco Nanocoll®) and 1 ml blue dye (Patent Blue V®), SLNB was performed. If no sentinel node could be identified, ALND of levels I and II was performed. A cALND was performed in the event of a positive SLNB diagnosed peri- or postoperatively, or if the primary tumour in the breast was found to be multifocal on pathological examination.
Pathological assessment
Frozen sections were obtained from each SLN and examined during surgery. If a sentinel lymph node was smaller than 4 mm, two sections were analysed separately. Nodes larger than 4 mm were bisected, and two sections from each half analysed. For paraffin-embedded histopathology, at least three sections were prepared from the sentinel node or each part of a bisected node. Sections were stained with haematoxylin and eosin (HE). If no cancer cells were detected, immunohistochemistry (IHC) with cytokeratin antibodies was also performed.
Non-sentinel lymph nodes were examined by routine staining (HE) according to the protocol of each pathology department.
At the time of inclusion into the cohort, pathologists rarely differentiated micrometastases from isolated tumour cells. To update the classification of metastases for the present study according to the revised American Joint Committee on Cancer Staging System for Breast Cancer, 35 all pathology reports describing SLN micrometastases after routine pathological work-up were scrutinised by a breast pathologist and three surgeons. When differentiation was not possible from the original report, original slides were re-examined and reclassified by the pathologist. Four groups of patients were identified based on the finding in the SLN: node-negative (pN0), isolated tumour cells (<0.2 mm, pN0(i+)), micrometastases (0.2–2 mm, pN1mi), and macrometastases (>2 mm, pN1).
The present analysis
For the present study, a positive SLN was defined as any SLN containing tumour cells, including isolated tumour cells. Patients who had at least one positive SLN and underwent cALND were included from the prospective database. Patients with positive non-SLNs were compared with those who had negative non-SLNs regarding age, size, histological type and grade of the primary tumour, oestrogen and progesterone receptor status, the number of positive and negative SLNs and SLN status.
The Tenon score was calculated for all patients by adding the point values for the presence of macrometastases in the SLN (yes = 2, no = 0), the histological tumour size in mm (>20 = 3, 11–20 = 1.5, <11 = 0) and the ratio between positive and total SLNs (1=2, 0.5–1 = 1, <0.5 = 0). 19 Applying the recommended threshold value of 3.5 or less, the predicted non-SLN status was compared with the actual status.
The incidence of axillary recurrence was compared with a smaller group of patients from the same SLN cohort who were diagnosed with SLN metastases but did not undergo cALND (n = 86).
Statistical analysis
Continuous variables (age, tumour size and number of SLNs), dichotomous variables (oestrogen and progesterone receptor status) and categorical variables (histological type and grade of the tumour, SLN status and ratio score between number of positive and total number of SLNs as defined in the Tenon score) were analysed in a univariate logistic regression model. All variables that demonstrated a statistically significant difference in univariate tests were then analysed in a multivariable regression model. A receiver operating characteristic (ROC) curve was drawn on the basis of the sensitivity and specificity of the Tenon score, and the area under the curve (AUC) was calculated.
SPSS 14.0® software was used for all analyses and statistical significance was set at the 0.05 level for all tests.
Results
Patient and tumour characteristics are given in Table 1. We identified 869 patients with SLN metastases where cALND was performed (282 cALNDs in a second session). Most of these patients (n = 691) had SLN macrometastases, but 20% (178/869) had metastases of ≤2 mm (11% micrometastases (98/869) and 9% isolated tumour cells (80/869), Table 2).
Patient and tumour characteristics in 869 SLN-positive patients who underwent completion axillary lymph node dissection.
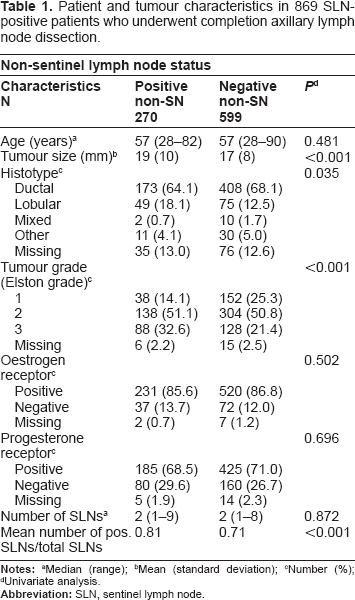
Median (range)
Mean (standard deviation)
Number (%)
Univariate analysis.
Sentinel lymph node (SLN) status in 869 SLN-positive patients who underwent completion axillary lymph node dissection.

Number (%)
<0.2 mm
0.2–2 mm
>2 mm.
Additional axillary metastases
Non-SLN metastases were identified in 270/869 (31.3%) patients, and 251/691 (36.3%) of the pN1, 11/98 (11.2%) of the pN1mi, and 8/80 (10.0%) of the pN0(i+) patients. Of these, non-SLN macrometastases were revealed in 8/11 (72.7%) of the pN1 mi and 3/8 (37.5%) of the pN0(i+) patients. The proportions of positive non SLNs according to total number of SLNs and number of positive SLNs are given in Table 3.
Cross tabulation of number of positive sentinel lymph nodes (SLNs) by total number of SLNs removed. Each cell represents the proportion of patients with positive non SLN.

We identified two groups of patients where the risk of non-SLN metastases was less than 10%. In pN1mi or pN0(i+) patients with a tumour smaller than 2 cm and Elston grade 1 or 2 (n = 102), it was 6.7%, and in pN1mi or pN0(i+) patients with more than two SLNs removed (n = 23), it was 6.0%.
Correlation between clinicopathologic characteristics and positive non-SLNs
Tumour size and grade, SLN status and ratio between the number of positive SLNs and total number of SLNs were significantly associated with non-SLN status, both in uni- and multivariate analyses. Histotype was significant only in the univariate analysis.
Tenon score
The mean Tenon score was 5.29 in patients with non-SLN metastases and 4.49 in those without (
The area under the curve was 0.65 (95% CI 0.61–0.69) for all patients (Fig. 1), 0.63 (95% CI 0.59–0.67) for patients with SLN micro- and macrometastases, 0.57 (95% CI 0.44–0.70) for patients with SLN metastases of ≤2 mm, and 0.54 (95% CI 0.37–0.72) for pN1 mi patients only.

The receiver operation curve (ROC) for 869 sentinel lymph node-positive patients calculated for the Tenon score; blue line, area under the curve (AUC) 0.65. The green, diagonal line represents AUC 0.5 (flipping a coin).
Axillary recurrences
In the study group, there were 10/869 (1.2%) isolated axillary recurrences (8/691 (1.2%) in pN1 and 2/98 (2.0%) in pN1mi patients) after 56.3 months median follow-up. Almost all patients (860/869, 99.0%) had adjuvant treatment (81.5% radiation, 83.2% hormonal treatment and 49.4% chemotherapy).
In a separate group of 86 patients with SLN metastases in whom ALND was omitted (mean Tenon score 3.11), 1/86 (1.2%) patient had an isolated axillary recurrence after 51.8 months median follow-up. In this group, 82/86 (95.3%) had adjuvant treatment (68.6% radiation, 86.0% hormonal treatment and 5.8% chemotherapy).
Discussion
Several authors have, by creating nomograms and scoring systems, attempted to define a subset of SLN-positive patients in whom cALND could safely be omitted. The Tenon score outperformed other scoring systems in a study by Coutant et al 27 and includes characteristics that can be estimated at the time of the SLN biopsy. In the present study, we evaluated the Tenon score in a Swedish multicentre cohort. The AUC was only 0.65 and the performance of the score was thus inadequate in our patient cohort.
A validation study demonstrating good accuracy of the Tenon score was also presented by Coutant et al, 36 with both studies from this group evaluating French populations. A French data set was also used to develop the Tenon score. In contrast, validation studies in other populations and also a recent French validation study demonstrate less prediction accuracy (AUC 0.58–0.70),29,37–39 which the results from our study are in accordance with. This could represent differences in populations, surgical technique or pathologic examination.
Unfortunately, we were not able to validate the Memorial Sloan-Kettering Cancer Center (MSKCC) nomogram 24 in our population as we had incomplete information about the occurrence of lymphovascular invasion. The MSKCC nomogram has, however, been validated in several other studies, and the AUC varied between 0.58 and 0.86.27,39 In three studies the AUC was less than 0.70 (the limit used for considering an acceptable predictive ability), possibly reflecting population differences in a similar way as for the Tenon score.
Several studies have tried, but have been unable, to define a subgroup in which cALND can safely be omitted.8,13,40–43 In a meta-analysis by Degnim et al, 8 no subgroup had less than a 10% risk of non-SLN metastases.
We could identify two groups of patients in whom the risk of non-SLN metastases was less than 10%. However, these were very small subgroups (n = 102 and 23, respectively) that were not pre-planned in the study and their clinical significance is therefore questionable. The results of our study, and most of the previously published, similar studies, indicate that the evaluation of primary tumour and SLN characteristics is not sufficient to decide whether to proceed with further axillary surgery.
Interestingly, only one of 86 SLN-positive patients in whom cALND was omitted had an isolated axillary recurrence. In accordance, a low incidence of axillary recurrence was previously demonstrated in other studies.10,12,44 In a review by Rutgers, the 2- to 3-year risk of axillary recurrence in SLN-positive patients was 0 to 1.4% if the axilla was left untreated. 45 In part, this could be explained by better prognostic factors in the patients that did not have cALND, but many studies have reported the axillary recurrence rate to also be lower than expected in SLN-negative patients. Since the false negative rate is known to be about 5%–10%4,46–48 this indicates that not all positive lymph nodes left behind will develop into clinically significant metastases.
Recently, in a report on 97 314 patients who had breast cancer surgery between 1998 and 2005, Bilimoria et al 49 found no significant difference in axillary recurrence or survival for SLN-positive patients who underwent SLNB alone compared with those who had cALND. It is, however, a retrospective study and the completeness of follow-up was not reported. Furthermore, between 1998 and 2000 the number of excised lymph nodes was almost as high in the SLNB as in the ALND group.
Additionally, the American College of Surgeons Oncology Group (ACO-SOG) Z0011 trial found no higher incidence of axillary recurrence 50 and comparable survival 17 in SLN-positive patients randomised to omission of cALND compared with those who completed an ALND after a median follow-up of 6.3 years. However, only 891 of the planned 1900 patients were accrued and the study was closed early. Considering the low accruement rate (despite many participating centres, several of these probably with large patient volumes), one cannot rule out the possibility of a significant selection bias, and included patients were at low risk for recurrence. Furthermore, all patients received whole-breast irradiation, including the lower part of the axilla.
We therefore believe that it is too early to abandon ALND for all SLN-positive patients.
Conclusion
The Tenon score performed inadequately in our material and we could only define a very small group of patients in which negative non-SLNs could be predicted.
Role of the Funding Source
The funding sources had no input in the study design, in the collection, analysis and interpretation of data, or in the writing of the manuscript.
Conflict of Interest Statement
The authors declare no conflicts of interest.
Ethical Approval
The study was approved by the ethics committee of Karolinska Institutet, Stockholm, and each region's local ethics committee. All patients gave written informed consent.
Disclosures
Author(s) have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributorship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.
Footnotes
Acknowledgements
The authors thank the medical staff at all participating hospitals for the inclusion and follow-up of patients. Special thanks are due to Marie-Louise Walker-Engström at the Centre for Clinical Research of Uppsala University, Central Hospital, Västerås, for excellent data management.
The study was funded by grants from the Swedish Breast Cancer Association (BRO), the Swedish Cancer Society and the Centre for Clinical Research of Uppsala University.