
Abstract
Breast cancer is the most common cancer in women and the second leading cause of cancer deaths in women. The key to surviving breast cancer is early detection and treatment. Current technologies rely heavily on imaging of the breast, and although considered the gold standard, they have their limitations. There is a need for a more accurate screening test for women of all ages, which can detect the cancer at a cellular level and before metastasis. There have been extensive studies into markers for breast cancer including protein and nucleic acid biomarkers, but to date, these have been unsuccessful. A growing field of interest is the association between breast cancer (tissue and cells) and lipids, which is documented in the literature, and may be considered as a leading candidate in the breast cancer detection space.
Breast Cancer
Incidence by Age
Breast cancer occurs in women of all ages, although, as a woman ages, her risk of developing breast cancer increases. Women between the ages of 20 and 29 years account for only 0.3% of breast cancer cases. Around 20% of breast tumors are found in women younger than 50 years, and 40% of breast tumors are found in women aged 65 years and older. 4 About 80% of women with breast cancer are older than 50 years at the time of diagnosis.
Current Recommended Screening
Ademuyiwa et al 5 have recently stated that screening for breast cancer, via annual mammography and clinical breast examination, should begin at the age 40 years for average-risk women. Breast self examination is an additional option, although it is not recommended in some countries. 6 For women under the age of 40 years with no other risk factors, routine mammography is not recommended. Instead, these women are encouraged to undergo clinical breast examination every three years, with breast self examination being optional. Given this, Ademuyiwa et al state that most malignancies in women under 40 years will be detected by patients themselves. The limitation of these methods is that they rely on a visible or palpable lump for detection, which means that in practice the tumor has to be of a minimum size (at least 5–10 mm), by which time it may have metastasized.
Mammography is not recommended for younger women as their breasts are denser and the identification of masses is less obvious in breast imaging.7,8 Since most breast cancers occur in older women, this is not considered a major problem, but for young women who have a genetic risk factor for breast cancer, the relative lack of effectiveness of mammograms is a serious issue because breast cancer often develops at a younger age in these women 9 and is often more aggressive than in older women.10–12
The Importance of Early Detection
Although the overall incidence of breast cancer has been increasing for more than two decades, there has been almost a 30% reduction in mortality beginning in 1990. 13 The two factors that have been attributed to improved mortality rates are 14 early detection (primarily by mammography screening) and more effective and increased application of antihormonal drugs and chemotherapy. This has been the basis for developing improved methods for the early detection of various forms of breast cancer, prior to it metastasizing, in order to maximize the treatment outcomes. 15 It is estimated that 40% of breast cancer patients have regional (stages II–III) or distant (stage IV) spread of their disease at the time of diagnosis 16 and this has changed little in the past 20 years despite the introduction of screening mammography in many countries for women in the target age group of 50–69 years. If breast cancer could be reliably detected prior to metastasising, there would be a significant reduction in individual mortality in the community. 17 This is not achievable by current breast screening technologies.
A Better Screening Test is Necessary
Simply stated, “if a tool, such as mammography, with only 40–70% sensitivity can reduce breast cancer mortality, then not only is early detection valid, but it is also a more powerful approach than ever imagined”. 18 The impact of a technology that has 90% sensitivity or more and has the potential to find 30%–60% of currently undetectable cancers 19 would have the potential to achieve an enormous reduction in breast cancer mortality.
A screening test should satisfy several criteria in order to reach the guidelines of public health and to reduce the morbidity and mortality of the diseased or symptomatic population. The criteria are as follows
20
:
high precision and accuracy, high sensitivity and specificity, useful for medical decision making, high predictive value, favorable cost/benefit ratio, and high throughput.
In addition, a screening test should be able to detect the disease at an early enough stage to allow for effective treatment.21,22 Attaining all of these requirements, while achievable in theory, is still highly challenging considering today's current breast cancer screening technologies.
A biological marker, the measurement of which is objective, provides the direction required to develop a screening test for breast cancer that can address these requirements.
The Association of Altered Composition of Phospholipids and Breast Cancer
Lipids
Lipids, also known as fatty acids, are carboxylic acids composed of a carboxyl group and hydrocarbon chain with a polar hydrophilic end and a nonpolar hydrophobic end. 23 Lipids are known to play a multitude of roles in cellular biology. They make up at least 50% of the cellular membrane, serving as structural molecules, 24 and are influential in signaling pathways within cells through their interaction with transmembrane proteins.25–27
There is considerable evidence that some lipids are elevated in breast cancer cells and tissue.28–38 A study on breast and tumor tissues has found that the distribution of individual lipid species varied and was “not uniform, reflecting microenvironment differences” due to the integration of tumor tissue into healthy breast tissue. 39 The same group also found that the level of a particular lipid was 28% higher in high-grade tumor tissue than in low-grade tumor tissue. 40 Mimmi et al 41 also reported highly increased levels of phosphocholine (PCho), total choline, and PCho/glycerophosphocholine ratio in tissue samples taken from patients with breast cancer than in healthy tissue. It has also been reported that there is a significant difference in serum lipid content between breast cancer patients and disease-free individuals, in particular, in a class of lipids called phospholipids.42–44
Phospholipids as Biomarkers of Breast Cancer
Phospholipids are a class of lipids consisting of two fatty acyl molecules esterified at the sn-1 and sn-2 positions of glycerol and contain a head group linked by a phosphate residue at the sn-3 position. 45 They are composed of hydrophobic fatty acyl chains and a hydrophilic head group, which defines the phospholipid species (Fig. 1).

Schematic representation of a phospholipid species structure. Adapted from Ref. 45.
Phosphatidylcholine (PC), phosphatidylethanolamine (PE), and sphingomyelin are the most dominant phospholipids in the majority of biological membranes, comprising up to 80% of the membrane. 46 Most studies report an increase in phospholipid metabolism in breast cancer tissue, particularly PC and PE or their precursor molecules (PCho and phosphoethanolamine).35,47–49 Some studies have found specific changes in choline metabolism that were linked to more aggressive carcinomas.50,51 It has been proposed that the altered cellular lipid structure is associated with altered cellular functions, such as protein trafficking, which promotes the onset of cancer or contributes to the progression of the disease.52–54
Measuring Phospholipids using Mass Spectrometry
Lipid extraction from biological samples requires the use of solvent. Membrane-bound lipids need polar solvents (ethanol and methanol) to disrupt the hydrogen bonds and to release the lipids, whereas other lipids can be extracted using nonpolar solvents such as chloroform and diethyl ether. 55
Once extracted, species identification and analysis are currently performed using mass spectrometry, as this technique allows the most sensitive and selective identification and quantification of a variety of lipids. 56
Mass spectrometry measures the molecular mass of a sample using the following three functional components: an ionization source, an analyzer, and a detector. 57 The sample is injected into the ionization source where molecules of the sample are ionized making them easier to manipulate than neutral molecules. 58 The ions then enter into the highly vacuumed region of the spectrometer, the analyzer, and the detector. This vacuum ensures that the ions travel through the instrument without an interference from air molecules. There are two analyzers; the first separates the ions according to their mass-to-charge ratio (m/z), and the second monitors specific fragment ions. They are then identified on the detector as a signal on an attached computer. The m/z ratios along with the relative abundance present the sample as an m/z spectrum and allow qualitative and quantitative detections. Raw data from the mass spectrometer are processed using the commercial software, which contains information about the masses identified from the precursor scans and subsequent analysis, and the spectra are matched against a lipid library.
Lipogenesis and Breast Cancer
The loss of breast cancer susceptibility gene 1 (BRCA1) is associated with breast cancer. 59 BRCA1 is a tumor suppressor gene and is also an inhibitor of lipogenesis, and the loss of BRCA1 has been shown to increase lipid production in breast cancer cells. 60 In addition, it has been demonstrated that the activation of fatty acid synthase expression and concomitant lipid synthesis is a common event in breast cancer. 61
There is further evidence that increased lipogenesis is closely linked to tumorigenesis in breast cancer. Chajes et al 29 found that mechanisms specifically related to malignant transformation and tumor progression influence the membrane lipid profile of breast carcinoma as determined by thin layer chromatography.
In Vitro Association of Lipids and Breast Cancer Cells
Increased expression levels of specific choline transporters and of PCho occur in breast cancer cells than in normal mammary epithelial cells.28,30,32,37,38,62
Singer et al 36 found a 16–19-fold increase in PCho content in two primary breast cancer cell lines and a 27-fold increase in PCho content in a metastatic breast cancer cell line compared with normal breast epithelial cells. There are other indications that an altered phospholipid profile correlates with alteration in tumor characteristics. Total phospholipids in malignant breast cancer cell lines differ between hormone-sensitive and highly hormone-resistant tumors. 63 In particular, two phospholipid components, a PC and a PE, that were absent or at very low levels in hormone-sensitive cells were significantly increased in highly hormone-resistant cell lines.
Phospholipids in Body Fluids Associated with Breast Cancer
Levels of phospholipids have been reported in a small five-patient pilot study in urine64,65 and serum or plasma43,66–68 of patients with breast cancer. The urine analysis showed that PC, PE, and two phosphatidylserine molecules (18:1/18:1 and 18:2/18:0) were significantly increased in some of the breast cancer patients and decreased to baseline levels following surgery. Feldman and Carter's 66 study failed to show any difference in the levels of phospholipids between women with breast cancer and healthy women, but in later studies, significant differences were found. In Hammad et al's 43 study, the most significant differences in lipid profiles among disease-free and cancer subjects were attributed to three PCho species (precursors to PC) and to three unidentified fatty acid species. Yang et al 67 also reported that specific phospholipids found in the plasma of patients with benign breast tumors, malignant breast tumors, and healthy controls were able to discriminate between the groups and suggested that these phospholipids have potential in the clinical diagnostic space. The concentration of serum lipids has been shown to be affected following treatment of the disease as Ray et al 68 found that those lipids that were elevated in breast cancer decreased after treatment.
Plasma is known to contain multiple lipoprotein pools, each consisting of many lipid classes that contain up to thousands of separate lipid species. 69 Their composition is highly influenced by dietary sources. Meikle et al showed that many of the phospholipid classes of interest in the association of changes of levels of phospholipids with breast cancer are altered following consumption of soy or dairy diets. For example, they reported that plasma PC, PE, phosphatidylinositol, and phosphatidylglycerol increased significantly after a dairy-based meal. However, after a soy-based meal, several phospholipids decreased, in particular sphingomyelin and the ether-linked and lysophospholipids. 70 This needs to be taken into account when attempting to determine an association between plasma phospholipids and diseases such as breast cancer.
Therefore, to be able to discern a consistent pattern of phospholipid species across different breast cancer types above the noise of dietary lipids is a significant challenge. Exosomes from breast tumors provide a more specific source of cancer-associated lipids than whole serum.
Exosomes
Extracellular vesicles (EVs) are produced by the outward budding and release of lipid-bound particles from cells into the extracellular environment.71,72 One type of these EVs is of endosomal origin, called exosomes. Exosomes are released into the extracellular environment when an endocytic invagination forms a multivesicular body, which fuses with the plasma membrane.71–74
Another type of EVs is derived from the plasma membrane, called microvesicles, which are directly pinched off the plasma membrane toward the extracellular environment.71–74 These extracellular vesicles have been postulated to have a role in intercellular communication as transport vehicles of proteins, lipids, and RNA 75 and also appear to be involved in tumor progression. 71 They have been suggested to facilitate malignancy, invasiveness, and the evasion of the immune response.76–79
The cellular origin of these extracellular vesicles determines their make up, and once they are released into the extracellular environment, they may be involved in the transfer of molecules between cells and also enable the deposit or removal of molecules at distal sites. 71 As a result, they have been identified in numerous bodily fluids including blood, urine, breast milk, and saliva, which make them a candidate as markers for identifying intracellular changes.80–82 Once these fluids have been collected, exosomes can be easily isolated using differential ultracentrifugation. 80 The ubiquitous nature of exosomes in bodily fluids makes them ideal for use in diagnostic biomarker studies. 80
It has been observed that there are significantly elevated exosome concentrations in the blood of patients with cancer than in that of controls. This could be due either to an increased production of exosomes per vesicle (endosome/multivesicular body)83,84 in cancer cells or to an increased production of these endosomes and multivesicular bodies in cancer cells (see Fig. 2).
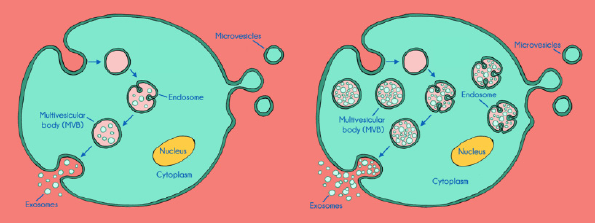
Schematic illustration of exosome production in a normal cell (left) versus exosome production in a cancer cell (right), which illustrates the elevation of exosome production and the potential amplification of metabolites.
Tumor-derived exosomes have a distinct protein and lipid composition resembling that of the cells from which they are derived. 85 Phospholipids isolated from exosomes in plasma from patients with breast cancer are reported to be different to those identified in plasma from patients with lung cancer, which are distinguishable from healthy individuals. 86 Therefore, this makes phospholipids from exosomes a potentially specific biomarker for the detection of breast cancer, possibly even at an early stage.
Therefore, the lipid composition of blood-borne exosomes originating from tumor cells is likely to reflect tumor-specific membrane alterations independent of dietary lipids in the blood. Smith et al 87 recently reported that cancerous cell-derived exosomes are relatively depleted in cholesterol and enriched in phospholipid compared to noncancerous cell-derived exosomes.
In support of the influence of dietary lipids as a confounding variable in determining an association between phospholipids and the presence of breast cancer, measurement of the phospholipids in the plasma from fasting breast cancer patients was able to accurately distinguish cancer patients from healthy controls. 44 This indicates that when dietary lipids are removed as a confounder, the endogenous phospholipids provide specificity for the detection of the presence of breast cancer. It is likely that these endogenous phospholipids originate from exosomes shed from the tumors.
Conclusion
Despite the widespread use of mammography, there is an acknowledged need for a more reliable screening test for breast cancer. The optimal biomarker would be one that could identify specific molecular changes in the body shortly after a breast tumor is formed. Most biomarker studies have failed to deliver an accurate assay, probably due to the heterogeneity of the disease, and the low accuracy of assays that use one or a small number of biomarkers. 88 Panels consisting of multiple biomarkers are likely to be a more sensitive and specific approach to detect the disease. 89 Circulating endogenous phospholipids in the plasma of breast cancer patients originating from tumor-derived exosomes may represent a novel class of biomarkers that could be used as the basis of a blood-based screening test for the detection of the disease. Preliminary reports indicate that a panel of phospholipids is required to achieve high levels of accuracy. More work is needed to overcome issues of scalability of exosome isolation and mass spectroscopy multivariate analysis before such a screening test could be practicable. A combination of mammography and phospholipid analysis may result in an increased accuracy and earlier detection of disease, with a resulting significant improvement in morbidity and mortality.
Author Contributions
Analyzed the data: DM, PF. Wrote the first draft of the manuscript: PF. Contributed to the writing of the manuscript: DM. Agree with manuscript results and conclusions: DM, PF. Jointly developed the structure and arguments for the paper: DM, PF. Made critical revisions and approved final version: DM, PF. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgment
The authors wish to thank BCAL Diagnostics Pty Ltd for their support in funding this review.