
Abstract
Benign mammary lumps and mastalgia are the most common breast disorders; yet, there is no clear-cut consensus about the best strategy for their treatment. We hypothesized that a combination, including boswellic acid, betaine, and myoinositol, would be beneficial in breast disorders by exerting a pleiotropic effect on multiple pathways. Indeed, myoinositol has already been proven to modulate some factors involved in the genesis of breast diseases, such as fibrosis and metabolic and endocrine cues. In our study, 76 women were randomly assigned to either the experimental or the placebo arm. After six months of treatment, statistically significant differences between the two groups were recorded for pain relief (56% vs 17%) and breast density reduction (60% vs 9%). Furthermore, benign breast mass dimension showed a reduction in the experimental group (40% vs 16%). The combination of boswellic acid, betaine, and myoinositol has been demonstrated to be effective in the treatment of breast pain and radiologically and histologically confirmed benign breast mass and in the reduction of breast density, one of the pivotal risk factors for the development of breast cancer, without any side effects.
Introduction
Breast pain (mastalgia) is a very common disorder experienced by women, and it was recognized as a relevant medical issue even before its first description, reported in the scientific literature in 1829.1,2 Pain is usually associated with mammary masses, and it represents a major symptom belonging to benign breast disorders. Clinical surveys have estimated the occurrence of breast ache, from mild discomfort to severe pain, at 60%–80% in women, and the real prevalence is likely to be higher, given that fewer than half of women with severe pain are willing to report this symptom to a physician. 3 Breast pain may be severe enough to interfere with usual daily activities, and its effects on the quality of life as well as its psychological implications are often underestimated. 4
Mastalgia is usually thought to be inextricably linked to fibrocystic disease, as reported in many textbooks, and breast pain is generally deemed to be a dysfunctional consequence of the benign dysplasia. Undeniably, benign breast diseases (BBDs) are frequently associated with breast pain or discomfort. However, the association between breast pain and fibrocystic histology is far from consistent, given that the same incidence of a wide array of fibrocystic histological findings has been reported in women with or without breast pain.5,6
There are three main clinical categories of breast pain: cyclic mastalgia (arising during the luteal phase of the cycle), noncyclic mastalgia, and extramammary pain (musculoskele-taltenderness or pain associated with breast discomfort and/or benign lumps). 7 The odds of treatment success may vary according to the different types of pain. 8
Current available therapies are inadequate and a search for an optimal strategy is still warranted. In some cases, pain relief can be obtained even without pharmacological intervention by means of psychological care, while in some instances medications are effective. 9 Promising results have been obtained with evening primrose oil, 8 although a subsequent randomized, multicentric study does not support previous reports. 10 In some studies, about two-thirds of patients with noncyclic breast pain or associated musculoskeletal ache responded to oral or topical anti-inflammatory, nonsteroidal treatment,11,12 evidencing how important inflammatory processes could be in the emergence of BBDs. Consistent results have been obtained with a few endocrine manipulations, but the concomitant side effects led a relevant fraction of patients to discontinue the drugs. Danazol, tamoxifen, gonadotropin-releasing hormone agonist, and bromocriptine are usually recognized to be effective in selected groups,13–16 but ultimately, the large number of hormonal approaches and remedies promoted to alleviate mastalgia attests the lack of a single effective agent with ew adverse effects. 17 Moreover, various approaches highlight our limited understanding of the complexity of BBDs.
Actually, mastalgia is still an enigmatic condition, as its causes are poorly understood and are likely to be multifactorial. Molecular alterations typical of malignant breast carcinomas do not seem to occur in benign breast lesions. 18 Hormonal imbalances, 19 metabolic and inflammatory processes, 18 and disorders of the crosstalk among epithelial cells and the surrounding stroma are deemed to have roles in the etiology of benign breast pain, as evidenced by the increased rate of mastalgia in women with simple duct ectasia.20,21 Moreover, while no relevant changes in circulating steroid sex hormones have been related in women with BBDs, 22 it has been suggested that hormonal disorders play a part in the genesis of mastalgia. Indeed, breast pain arises in a relevant fraction of women undergoing endocrine, estrogen-based treatments. Moreover, mastalgia is frequently observed in women suffering from premenstrual syndrome, 23 but only rarely observed after menopause. 24 Additionally, patients suffering from breast pain have been found to have disorders of lipid metabolism that may affect cell wall constitution, locally enhancing cells' responsiveness to endocrine stimulation in a significant manner.25,26 Accordingly, some studies have been undertaken in order to investigate whether women suffering from mastalgia could benefit from interventions targeting lipid metabolism.27,28
Myoinositol, a sixfold alcohol of cyclohexane, has been proven in separate studies to modulate inflammatory, metabolic, oxidative, and endocrine processes in a wide array of human diseases, including cancer.29–32 Similarly, both boswellic acid and betaine (three-methyl glycine) inhibit inflammation and exert protective effects on breast physiology.33–36 Given that some reports have documented anecdotal improvement of mastalgia in women suffering from polycystic ovary syndrome 37 or premenstrual dysphoric syndrome 38 after treatment with myoinositol, we hypothesized that a combination including boswellic acid, betaine, and myoinositol would be beneficial in relieving breast pain via a multitargeted effect on different pathways, including inflammatory, metabolic, and endocrine processes.
Patients and Methods
Patients
Drug formula

Baseline characteristics of all premenopausal randomized patients

To investigate the therapeutic benefit of the experimental treatment, we used a double-blind, randomized, placebo-controlled, parallel group design according to a block randomization model, described elsewhere. 41 In order to ensure a correct balance between the two groups, patients were randomized to treatment using a minimization procedure. 42 The patients of the first group (placebo) received oral capsules (two capsules twice a day), containing a combination of vitamins (B2, B6, folic acid, and N-acetylcysteine). The patients of the second group (treated) received oral capsules (two capsules twice a day), filled with the same vitamins plus boswellic acid, betaine, and myoinositol.
The first visit to the outpatient clinic included a detailed history and a clinical examination by an experienced surgeon. Mammography and ultrasound examinations were performed at the baseline and after the treatment period (>6 months). Clinical assessment of BBDs (fibroadenoma, duct ectasia, and isolated duct papilloma) was obtained by a twice-distinct opinion carried out by two expert radiologists. Suspect lesions were further evaluated by means of magnetic resonance and/or biopsy. Patients suffering from bloody nipple discharge, those affected by premalignant lesions (carcinoma in situ), and those with breast cancer were excluded. Changes in benign breast nodules' response were considered significant for major diameter increase or reduction higher than 20% of their initial value measured by mammography. Qualitative assessment of breast density was performed according to the study by Oza and Boyd, 43 subdividing the patients into four main categories as follows: (1) almost entirely fat, (2) scattered fibroglandular densities, (3) heterogeneously dense, and (4) extremely dense.
Patients were requested not to change their diet during the participation in the trial. Patients were seen at baseline (first visit), at randomization, and three and six months after randomization; the treatment was given for six months. The patient's opinion about the changes in breast complaints was assessed by a questionnaire at the time of randomization and again after three and six months. Patients were also asked to register the daily occurrence of other symptoms (nausea, headache, mood disturbances, and menstrual discomfort) and the changes in breast tenderness and pain. Pain changes, which were relative to pain levels at the time of the previous questionnaire, were scored as –1 (worsening), 0 (no change), 1 (a little better, with residual, mild pain), and 2 (far better, disappearance of breast pain), according to a modified Cardiff Breast Score. Overall response rate was evaluated after six months by comparing the incidence of responsive patients among the two treatment groups. Pain severity was evaluated by patients themselves by means of a 10 cm visual analog scale 4 as mild (from 1 to 4 cm), intermediate (from 5 to 7 cm), and severe (from 8 to 10 cm). Changes in breast density and nodule dimension were obtained by mammography, performed at the beginning of the trial and again after six months.
Statistics
Clinical response—pain relief (descriptive data)

Pain relief (drug vs. placebo comparison)

The scarcity of patients constrained us to adopt the Fisher's exact test for assessing significance instead of chi-square (cells with <5 units). For each pain class and for the whole data set, in addition to Fisher's exact test significance, a confidence interval (CI) at 95% of the odds ratio is reported. The CI was estimated by means of Wald's approximation.
Results
Overall, 62 patients completed the trial, while four patients were lost during the follow-up for nonmedical reasons; two of them, however, reported a significant symptomatic improvement when asked during a telephone interview.
Taken as a whole, the compliance of the two groups was higher than expected (93% in the control group and 96% in the experimental arm), as the treatment was discontinued only in a few cases and for less than a few days.
Pain Relief
Cyclic pain
Among the patients suffering from cyclic breast pain within the control group, only 3 of 18 (16.6%) patients showed a significant clinical response (Table 3). In the experimental arm, 10 of 19 (56.2%) patients reported significantly benefiting from the treatment (P < 0.001, Table 4). In the latter group, 7 of 19 (36.8%) patients showed an almost complete disappearance of breast pain at the end of the clinical trial.
Noncyclic pain
A mild improvement in pain relief was observed in the control group (2/12, 16.6%), whereas 8 of 13 women (61.5%) in the experimental arm experienced significant pain relief.
Relief of associated musculoskeletal pain was inconsistent within the control group, while a mild improvement was observed in three of seven patients (42.8%) in the experimental arm.
Overall, a significant benefit was observed in 18 of 32 patients (56.2%) in the experimental arm, while a clinical response was documented in a small fraction of the control group (5/30, 16.7%). Significant pain relief was observed in the experimental group even after the first three months of treatment (data not shown).
Other Symptoms
Other symptoms—relief recorded in the control and experimental groups

Benign Breast Lumps and Breast Density
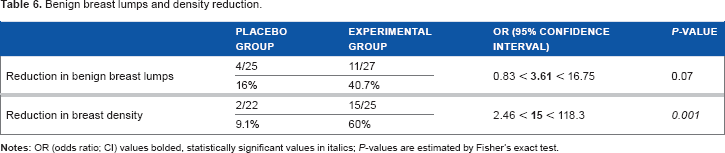
Incidence rates of benign breast nodules were 83% and 84% in the placebo and experimental arms, respectively. Mostly, these lumps were identified as fibroadenomas (18/30 and 18/32 in the control and experimental groups, respectively). The presence of a single cyst was observed in the remaining patients. Dimensions ranged from 0.4 to 0.9 cm for fibroadenomas (mean: 0.6 ± 0.2 cm in the control group and 0.5 ± 0.2 cm in the experimental arm) and from 0.3 to 1 cm for cysts (mean: 0.7 ± 0.3 cm in the control group and 0.7 ± 0.4 cm in the experimental arm).
Benign breast lumps and density reduction
Adverse Effects
Overall, no significant adverse effects were recorded in either arm. One case in the experimental arm experienced transient mild diarrhea.
Discussion
Data presented herein suggest that young women suffering from mastalgia and showing high breast density experience a significant clinical benefit when treated with a balanced composition, including boswellic acid, betaine, and myoinositol. Pain relief was achieved in a relevant proportion of patients enrolled in the experimental arm, and differences in response rate between the control and experimental groups have been shown to be very significant. It is worth noting that a considerable percentage of women in the experimental group experienced a major reduction in breast density. Increased breast density is deemed a pivotal risk factor for breast cancer, 44 because it induces high tissue stiffness and an augmented remodeling rate. Therefore, reducing mammary compactness by means of a simple, natural remedy could bring about very relevant clinical outcomes. 45
There is considerable debate about the choice of the best agent for initial management of mastalgia and BBDs. 46 Although hormonal-based treatments have provided consistent benefits in a large proportion of patients, these drugs are difficult to handle for a prolonged period. Concern over the long-term safety of tamoxifen still remains, and the incidence of side effects with danazol and bromocriptine (ranging from 30% to 46% according to different reports) leads many women to discontinue the therapy. It is generally agreed that hormonally active medications are more effective for patients with cyclic mastalgia and are indicated only for patients with severe, prolonged symptoms.47,48
Some studies have shown obesity and a high fat diet to be risk factors involved in the etiology of mastalgia. For this reason, other approaches include diet and nutritional interventions.46–48 However, there is a lack of direct evidence to support this theory, and, to date, no clear-cut consensus exists about a better treatment strategy in premenopausal mastalgia. Consequently, the search for more manageable and safer treatment options has prompted many clinicians to investigate different alternatives.49,50
Several vitamins have been evaluated as pharmacological support in the management of breast pain. Among many formulations, those including vitamin B1, vitamin B6, and vitamin E have yielded some results. Namely, early studies have evidenced a potential beneficial effect of vitamin E (α-tocopherol) in improving breast pain in women with fibrocystic breast disease.51,52 Tocopherol is thought to exert its effects by modulating steroidal hormone production, correcting abnormal serum cholesterol–lipoprotein distribution, and downregulating reactive oxygen species. 53 However, these preliminary results have not been confirmed by randomized, double-blind studies comparing vitamin E with a simple placebo. 54 To date, even if the evidence supporting routine use of vitamins in the management of breast pain is inadequate, vitamin supplementation is still regularly recommended by general practitioners. 55
Hypothesizing a synergy among three natural active compounds, boswellic acid, betaine, and myoinositol, all of which have anti-inflammatory and endocrine-modulating properties, we have studied their combined effectiveness in a pilot, randomized trial.
Preliminary data presented here support the starting assumptions, evidencing that vitamin supplementation, even if associated with a well-known antioxidant like acetylcysteine, bestows only a minor advantage in ameliorating mastalgia. On the contrary, the combination of boswellic acid, betaine, and myoinositol significantly improves breast pain and reduces mammary density in a relevant percentage of patients, without significant side effects. Additionally, the experimental formula ameliorates other mastalgia-associated symptoms, including anxiety and menstrual discomfort.
This effect is likely to be ascribed to the pleiotropic mechanism of action exerted by myoinositol on several metabolic, inflammatory, and endocrine pathways. Myoinositol has been shown to prevent pulmonary fibrosis after asbestos or inflammatory injury 56 and inhibit chronic colon inflammation, 29 likely by modulating the redox balance. 57 In addition, myoinositol may contrast inflammation-induced fibrosis by modulating TGF-β activity. TGF-β, particularly the TGF-β1 isoform, is a potent profibrogenic agent inducing collagen synthesis and regulating the balance between matrix-degrading metalloproteinases and their inhibitors. 58 In this way, it is a prominent factor in orchestrating cross-talk among epithelial cells and their microenvironment. 59 Myoinositol significantly modulates the expression of genes encoding TGF-βs and their receptors, thereby exerting immune-regulatory effects on the colonic epithelium under inflammatory conditions or during microbe-induced infection/inflammation in order to maintain the colonic mucosa in a noninflammatory state or to counteract infection.60,61 Breast fibrosis is usually recorded as an increase of breast density during mammographic examination and is likely to contribute to both mammary tenderness and pain. Given that TGF-β deregulation has been observed in BBDs, 62 modulation of TGF-β with myoinositol may significantly inhibit some clinical consequences, such as mastalgia. In addition, myoinositol exerts a modulating activity on cell metabolism, by improving glucose uptake and normalizing lipid metabolism. 63 Deregulated lipid metabolism participates in some way in the pathogenesis of BBDs: low levels of gamma-linolenic acid metabolites, as well as changes in serum lipoprotein patterns, may affect breast sensitivity to prolactin or to estrogens via prostaglandins and other signaling pathways.64,65 Therefore, it could be hypothesized that myoinositol may improve the clinicopathological features of both mastodynia and breast compactness by interfering with tissue metabolism at local and systemic levels. In fact, as demonstrated by a compelling body of scientific data, myoinositol improves altered metabolic and hormonal patterns in polycystic ovary syndrome (PCOS) patients.66,67 Myoinositol restores insulin sensitivity, counteracts hyperandrogenism, and modulates estrogen and follicle-stimulating hormone (FSH) activity in the ovaries.68,69 It is therefore likely that such a regulatory effect would be displayed in women affected by mastalgia and BBDs who were treated with myoinositol.
Conclusions
Women suffering from mastalgia and showing high breast density experience a significant clinical benefit when treated with a balanced composition, including boswellic acid, betaine, and myoinositol. However, studies on the clinical management of BBDs are frequently biased by statistical or design inadequacy, thus leading to untrustworthy conclusions. 46 Undoubtedly, our pilot study suffers from limitations and our main findings should be confirmed by a large survey, which should evaluate the length of the clinical response and any significant relapse rate. That study is currently ongoing. Nevertheless, data reported herein have demonstrated that the use of these natural combinations could be an important alternative therapy to current drugs for the management of benign breast disorders without side effects. Indeed, the proposed treatment offers a high response rate, thus making it a reliable option for prolonged treatment.
Author Contributions
Conceived and designed the experiments: MB. Analyzed the data: AG. Wrote the first draft of the manuscript: MB and SD. Contributed to the writing of the manuscript: VP, FT, and AC. Agreed with manuscript results and conclusions: AG, AHH, and SHA. Jointly developed the structure and arguments for the paper: MB, VP, and SD. Made critical revisions and approved the final version: MB. All the authors reviewed and approved the final manuscript.