
Abstract
Breakthrough pain (BTP) management is an unmet clinical need. BTP is poorly diagnosed, rarely evaluated and inadequately treated. BTP is transitory exacerbation of pain experienced by the patient who has relatively stable and adequately controlled baseline pain. BTP is reported to be common in adults and children with cancer as well as in non-cancer diseases associated with acute/chronic pain. Successful management of breakthrough pain depends on adequate assessment, appropriate treatment (cause of pain and symptomatic) and adequate reassessment. Ideal medication for BTP should be characterized with good efficacy and minimal side effects. Pharmacodynamic profile should mimic dynamics of BTP. Strong, short acting analgesics (e.g. opioids) administrated by route which allow quick action had potential to fulfil criteria for ideal ‘rescue’ medication for BTP. Fentanyl Buccal tablets (FBT; Fentora®, Frazer, PA, Cephalon Inc.) is novel delivery system for fentanyl citrate. FBT utilize OraVescent (r) technology to improve bioavability and speed of transmucosal delivery. Alternate routes of administration could further improve efficacy of BTP management. Intranasal and intrapulmonary routes are under exploration. Recently introduced new delivery systems for opioids medication do represent an improvements in BTP management, however BTP is still a major challenge to pain and palliative physicians.
Introduction
Breakthrough pain (BTP) remains on of the most challenging clinical problems for physicians and patients alike. Itt is poorly diagnosed, rarely evaluated and inadequately treated. 1 BTP is reported to be common in adults and children with cancer2–6 as well as in non-cancer syndromes associated with acute/chronic pain.7,8 Currently there is growing interest in BTP management generated by a greater awareness of the problem of breakthrough pain (secondary to improvement in the management of background pain) as well as its significant negative impact on quality of life, and fuelled by an increasing range of pharmacological options for the treatment of breakthrough pain. 9 BTP has a significant negative impact on quality of life.10,11 Complications of BTP are summarized in Table 1.3,5,10–12
Breakthrough pain could lead to following complications.

Definition of BTP
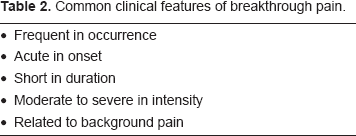
BTP is a transitory exacerbation of pain experienced by a patient who has relatively stable and adequately controlled baseline pain. 13 Bennett proposed a similar definition: BTP is an abrupt, short lived and intense pain that ‘breaks through’ the around the clock analgesia that controls persistent pain. 14 Other names include: episodic pain, exacerbation of pain, pain flare, transient pain, transitory pain. 9 The Expert Working Group of the European Association for Palliative Care (EAPC) has suggested that the term ‘breakthrough pain’ should be replaced by the terms ‘episodic pain’ or ‘transient pain’. 15 Common clinical features of BTP are summarized in Table 2. 10
Common clinical features of breakthrough pain.
Classification of BTP
Classification of BTP is presented in Table 3 (modified from 12 ). End-of dose failure is not a subtype of breakthrough pain it should rather be simply classified as inadequately controlled pain. 12 Patients with no background pain but who have severe episodic bouts of pain are classified as having transitory pain 16 and patients with poorly controlled background pain with or without severe transitory episodic exacerbations of pain are classified as having uncontrolled pain. 16
Classification of breakthrough pain.
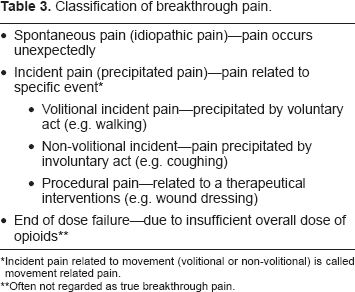
Incident pain related to movement (volitional or non-volitional) is called movement related pain.
Often not regarded as true breakthrough pain.
Prevalence of BTP
In a recent international survey, clinicians reported BTP in 23%–90% of adult cancer patients,3–6,11,16–19 and 74% in opioids treated non-cancer pain patients. 8 BTP appears to be more common in patients with advance disease. 20 In majority of studies the prevalence of incident related BTP (range 43%–64%) was higher than the prevalence of spontaneous BTP (relevance range: 17%–38%).4,10,11,16,19 Only one study observed opposite prevalence (spontaneous 59%, incident 24%). 6 Prevalence of BTP varies between different groups of patients 21 and is affected by certain language/geographical variables.17,22 BTP is a poor prognostic indicator. 23
Assessment of BTP
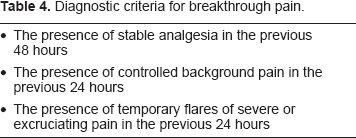
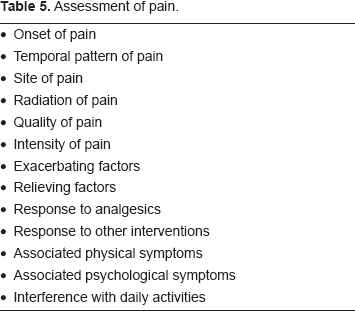
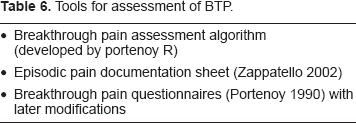
Breakthrough pain is not a single entity, but a spectrum of very different entities. The clinical features vary from individual to individual, and may vary within individuals over time. 24 Table 4 summarizes diagnostic criteria for BTP. 16 Successful management of breakthrough pain depends on adequate assessment 25 (Table 5), appropriate treatment (cause of pain and symptomatic) and adequate reassessment. 26 Many patients have more than one type of breakthrough pain10,16 and an association between the presence of breakthrough pain and the intensity/frequency of the background pain has been reported.10,17 Circadian variation in the occurrence of BTP has been reported (86% patients experienced BTP during day and only 45% during night). 4 Formal assessment tools for BTP are presented in Table 6.12,16,27
Diagnostic criteria for breakthrough pain.
Assessment of pain.
Tools for assessment of BTP.
Treatments of BTP
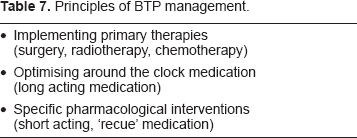
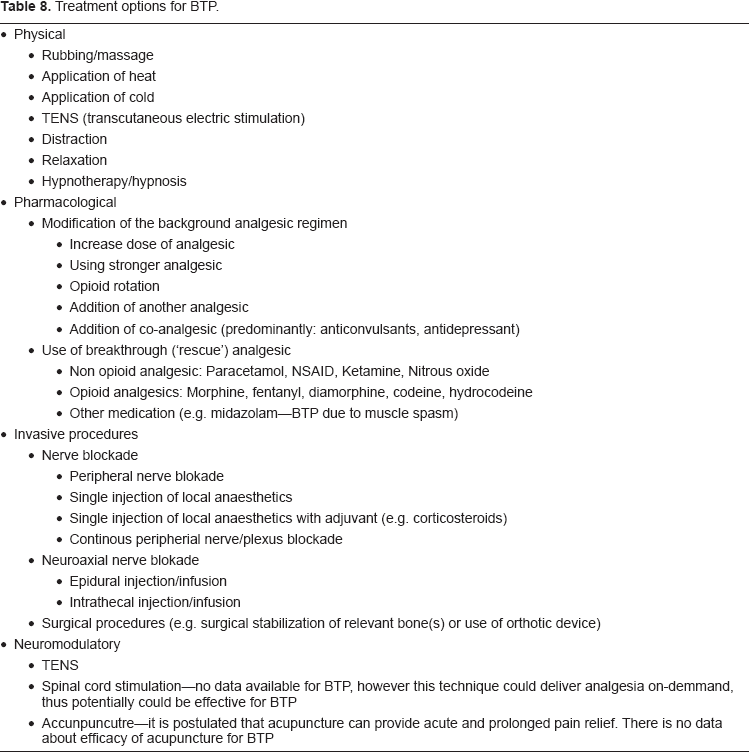
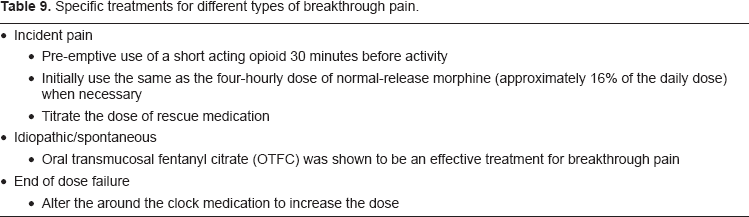
Holistic/multimodal approachs for BTP treatment have been proposed. Principles of BTP management 24 are presented in Table 7. Physical, pharmacological, neuro-modulatory treatments and invasive procedures are used in BTP management4,12,15,18,21,24,28–33 (Table 8). Pharmacological management should be tailored to the type of breakthrough pain34–36 (Table 9).
Principles of BTP management.
Treatment options for BTP.
Specific treatments for different types of breakthrough pain.
Ideal ‘Rescue’ Medication for BTP
The ideal medication for BTP should be characterized by good efficacy and minimal side effects. The pharmacodynamic profile should mimic the dynamics of BTP (Table 10). A potent, short acting analgesic (e.g. opioid) administrated by a route which allows for a rapid onset of action has the potential to fulfil the criteria for an ideal ‘rescue’ medication for BTP. A new class of opioids, Rapid Onset Opioids (ROOs), has been developed in an attempt to address the “unmet need” of breakthrough pain management.
Features of ideal ‘rescue’ medication for breakthrough pain.
Patients on chronic intake of opioids would have developed some tolerance to opioid side effects. Since the side effects associated with taking a breakthrough dose of opioid are similar to those associated with taking any dose of opioids (e.g. somnolence, nausea, vomiting, and dizziness); 37 one can infer that significant increse in the intensity of side effects from BTP medications should be less likely to occur when BTP medication is administered to an opioid tolerant patient. This concept led to the use of these potent ROOs only in opioid tolerant patients. While only approved for use in cancer pain, the utility of ROOs for pain in opioid tolerant non-cancer pain patients has been reported.38–40
Traditionally it has been suggested that one should use the same opioid to treat background and breakthrough pain. 41 The current approach utilizes opioids according to their pharmacodynamic properties and their pharmakokinetics: long acting for background pain and short acting (and preferably rapid onset) for breakthrough pain. Sometimes the same opioid is used for background and BTP as when a fentanyl patch is used to treat background pain and a rapid onset buccal or nasal fentanyl (transmucosal) preparation is used to treat BTP. At other times an opioid such as a controlled or sustained release morphine product is used for background pain and a transmucosal fentanyl is used for breakthrough pain. 12
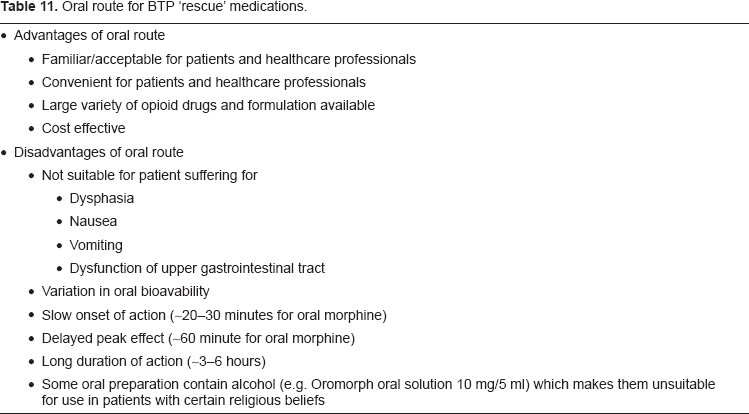
Traditionally, it was recommended to use a fixed ratio of the total daily dose of opioids to treat the breakthrough pain. 41 Randomize trials have demonstrated that there is no correlation between the dose of opioid needed to control background pain and the dose of OTFC needed to control the breakthrough pain.37,42,43 Thus, the dose of breakthrough pain medication should be titrated in the same manner as dose of background medication. 15 That is, the background pain medication and the BTP medication should be titrated independently. The World Health Organization (WHO) guidelines promote the use of the oral route for the management of cancer pain. 44 There route has the highest patient acceptability for route of administration. 45 The oral route is usually effective for the treatment of background pain; however, there are significant disadvantage of the oral route for breakthrough pain management. The oral route is associated with delayed onset of action (~20–30 minutes for oral morphine), 46 delayed peak effect (~60 minute for oral morphine) 15 and long duration of action (~3–6 hours). 46 Advantages and disadvantages of the oral route for BTP management12,15,41,45–47 are summarized in Table 11. Alternative routes of administration was proposed: oral transmucosal5,14,37,42,43,48Intravenous, 49 Subcutaneous, 50 Intranasal, 51 and Intrapulmonary. 52
Oral route for BTP ‘rescue’ medications.
Fentanyl Buccal Tablets
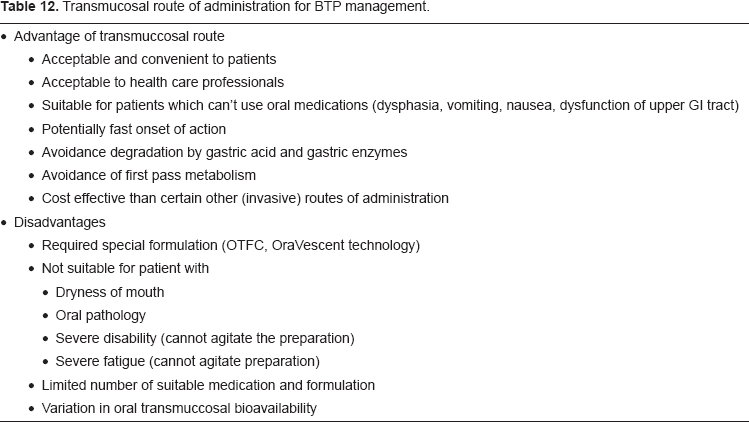
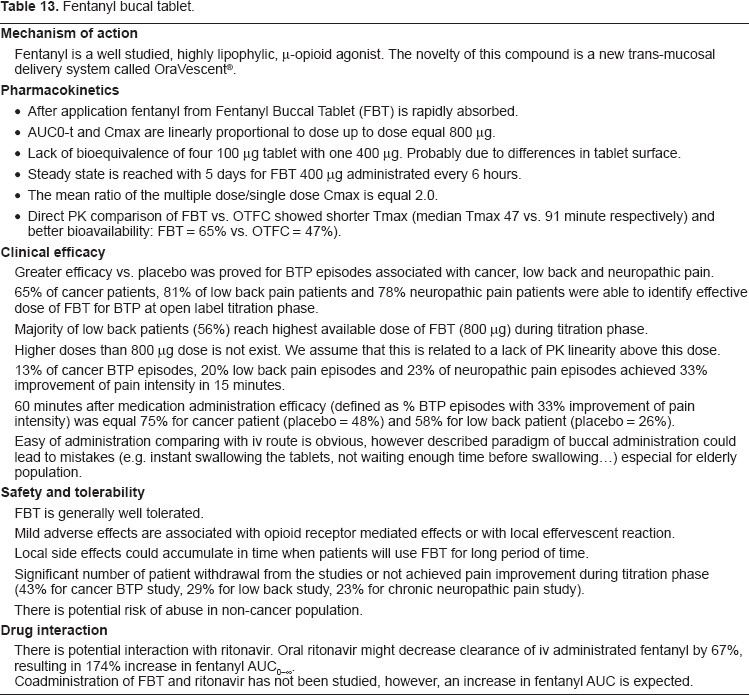
The fentanyl buccal tablet (FBT; Fentora®, Frazer, PA, Cephalon Inc.) is a novel delivery system for fentanyl citrate. Fentanyl is a well studied, highly lipophylic, μ-opioid agonist. The toxicological, pharmacologic effects and mechanisms of action of fentanyl are well characterized. FBT utilizes the oral transmucosal route of administration. The advantages/disadvantages of transmucosal route of administration45,53 are presented in Table 12. Transmucosal absorption allows fentanyl to bypass first-pass cytochrome P450 3A4 (CYP3A4) -mediated gastrointestinal and/or hepatic metabolism and allow more fentanyl to enter the systemic circulation compared with gastrointestinal absorption of oral fentanyl.54,55 FBT utilizes OraVescent (r) technology to improve bioavability and speed of transmucosal delivery. At the site of administration FBT produces an effervescent reaction which causes a pH decrease followed by a pH increase. These changes of pH are hypothesized to optimize pill dissolution and membrane permeability facilitating rapid absorption.54–56 This rapid absorption should decrease the time to onset of analgesia making FBT highly suitable for the management of breakthrough pain. 57 Properties of FBT are summarized 58 in Table 13. The effect of FBT has been studied out to 2 hours and analgesic effect has been shown to persist for the 2 hour study period. In studies on cancer pain FBT has demonstrated a 15 minute onset of action. 59 Fentanyl buccal tablets (FBT) is novel delivery system for fentanyl citrate. FBT utilises OraVescent® technology to improve bioavailability and speed of drug delivery.
Transmucosal route of administration for BTP management.
Fentanyl bucal tablet.
Future Perspectives
Alfentanyl and Sufentanyl are the synthetic opioid analgesics, chemically similar to fentanyl but with more rapid onset and shorter duration of action when given parenterally. 60 Sublingual Alfentanyl 61 and sublingual/buccal Sulfentanyl62,63 have been reported as being effective in small groups of patients for BTP treatment. Recently results of intranasal application of non-opioid medication for small group of non-cancer pain patients was published. Intranasal NMDA agonist (S)ketamine was succesful in rapid reduction of neuropathic pain 64 and may therefore be potential future medication for BTP.
Alternate routes of administration could further improve the efficacy of BTP management. Intranasal and intrapulmonary routes are under exploration. The nose can accommodate 150–200 microlitters of drug solution in each nostril. A special feature of the nasal route is the close association of the brain to the olfactory area and the unique physiology of this area (i.e. an absence of the normal blood-brain barrier): this may enable a fraction of the drug to enter the intrathecal space directly. 65
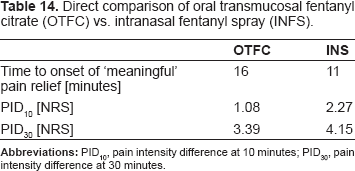
Intranasal fentanyl spray (INFS) was investigated in phase III, double blind, randomised, placebo controlled, crossover, multicenter trial. INFS was titrated to an effective dose (50, 100 or 200 microgram). Efficacy (compared with placebo) as well as safety and tolerability was demonstrated. 66 INFS was also directly compared with OTFC in open-label, randomised, crossover trial. INFS demostrated faster median time to onset of ‘meaningful’ pain relief compared to OTFC 67 (Table 14). Interestingly, there was only a weak association between effective INFS doses and effective OTFC doses. 67
Direct comparison of oral transmucosal fentanyl citrate (OTFC) vs. intranasal fentanyl spray (INFS).
Several explorative studies have looked at the use of intranasal opioids for the treatment of break-trough pain: fentanyl, morphine, diamorphine, and alfentanyl 12 have been studied and this route appears promising. Some agents may not be amenable for nasal administration, for example, methadone administrated by intranasal route caused a burning sensation in healthy volunterers. 68
A case report (two patients) of BTP successfully treated with intrapulmonary fentanyl administration was published. 52 This route may offer a speed of onset rivaling intravenous drug administration due to rapid access to the circulation via the pulmonary capillary bed. Further studies are needed to define the role of intrapulmonary medications in the management of breakthrough pain.
Conclusion
Recently introduced delivery systems for opioid medications represent major improvements in BTP management; however, the ideal drug or delivery system for BTP management is still an unfulfiled. The time to peak analgesia of the new rapid onset opioids, such as FBT, is still longer than the time to peak pain of many BTP episodes. Thus, the ideal BTP medication is yet to be found. Studies are needed to expand our knowledge about the different patho-physiological mechanisms involved in BTP and to help us understand the variability of BTP within the individual patient. If the intensity of BTP is variable within the individual patient, the initial dose titration paradigm used to define the effective analgesic dose of BTP medication could be inappropriate, being too high for some BTP episodes and too low for others. The ideal BTP medication would provide dosing versatility to address this intra-patient variability of BTP intensity. New fentanyl delivery systems offer theoretical advantages over short acting (regular release) oral morphine and patients seem to prefer the rapid onset opioids over morphine for BTP management. Studies that directly compare a rapid onset fentanyl preparation (FBT) and oxycodone are underway in the USA. More studies that compare rapid onset opioids and standard drugs like morphine and oxycodone regular release (short acting) in diverse patient populations are needed to help us define the full benefit of matching the time course of action of the analgesic to the BTP.
Disclosures
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors report no conflicts of interest.